Dinesh Singhal, Rahul Kakodkar, Arvinder S Soin, Subash Gupta, Samiran Nundy*
Department of Surgical Gastroenterology, Sir Ganga Ram Hospital. New Delhi, India
- *Corresponding Author:
- Samiran Nundy
Department of Surgical Gastroenterology
Sir Ganga Ram Hospital
New Delhi
India 110060
Phone +91-11.4225.2221
Fax +91-11.4225.2224
E-mail snundy@hotmail.com
Received August 25th, 2006 - Accepted September 12th, 2006
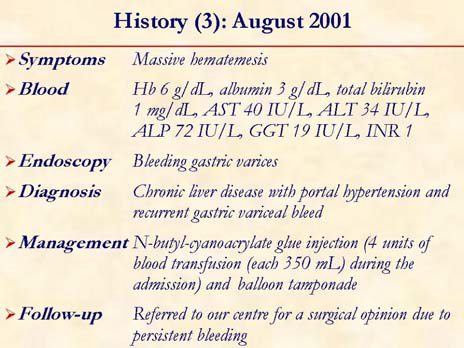
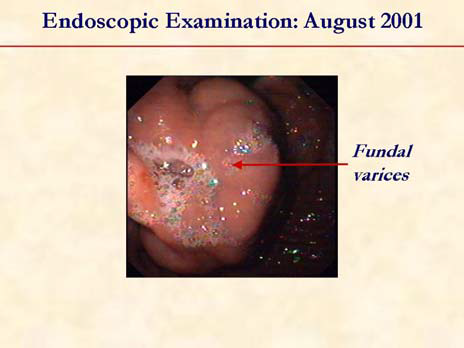
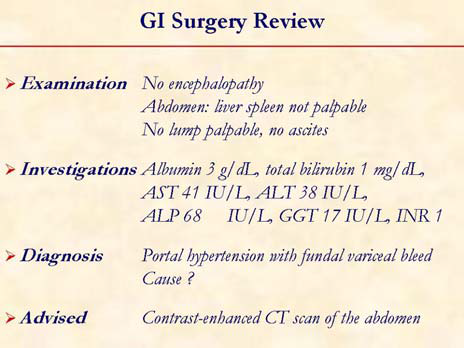
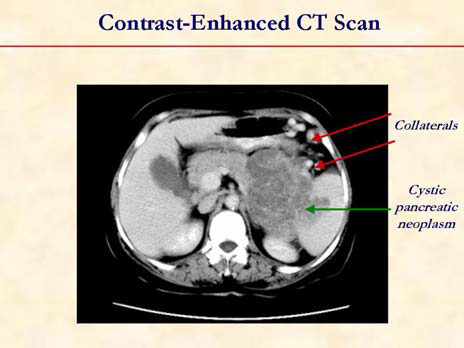
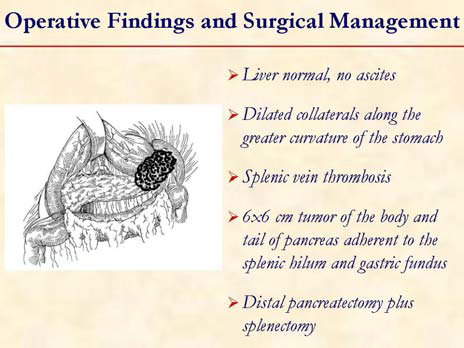
Sinistral portal hypertension is a clinical syndrome of gastric variceal hemorrhage in the setting of splenic vein thrombosis due to a primary pancreatic pathology. The distinguishing features from other forms of portal hypertension are preserved liver function and a patent extrahepatic portal vein. The important causes include acute and chronic pancreatitis, pancreatic pseudocysts and pancreatic carcinomas. Benign pancreatic neoplasms only rarely cause sinistral portal hypertension. Splenic vein thrombosis complicates 7-20% of patients having pancreatitis or a pancreatic pseudocyst; however, bleeding occurs in only approximately 5% of patients. The diagnosis of sinistral portal hypertension is achieved by a combination of gastroscopy, liver function tests, ultrasound examination (with Doppler) and/or contrast-enhanced CT scan of the abdomen.A mere demonstration of sinistral portal hypertension does not warrant intervention. An expectant management is justifiable in asymptomatic patients with pancreatitis. However, concomitant splenectomy may be considered in patients undergoing operative treatment of symptomatic chronic pancreatitis if sinistral portal hypertension and gastroesophageal varices are present. In patients presenting with gastric variceal hemorrhage, splenectomy (with treatment for the primary pancreatic pathology, e.g. distal pancreatectomy) is curative with excellent long term results.
Keywords
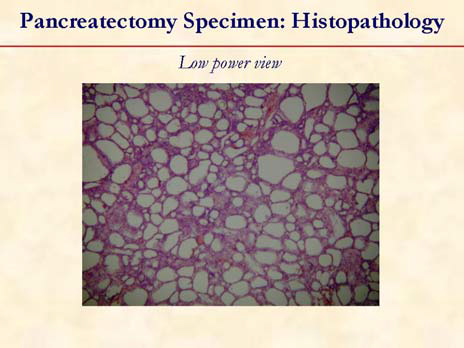
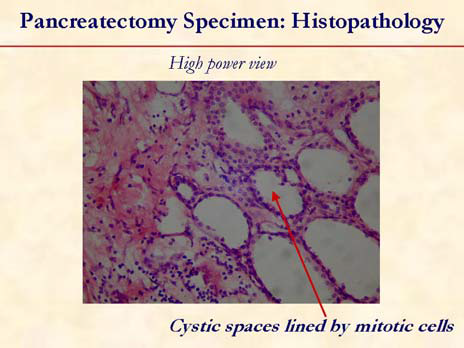
Cystadenoma, Serous; Esophageal and Gastric Varices; Splenectomy; Splenic Vein; Thrombosis
Abbreviations
SPH: sinistral portal hypertension
Summary
Sinistral portal hypertension is a clinical syndrome of gastric variceal hemorrhage in the setting of splenic vein thrombosis due to a primary pancreatic pathology. The distinguishing features from other forms of portal hypertension are preserved liver function and a patent extrahepatic portal vein. The important causes include acute and chronic pancreatitis, pancreatic pseudocysts and pancreatic carcinomas. Benign pancreatic neoplasms only rarely cause sinistral portal hypertension. Splenic vein thrombosis complicates 7-20% of patients having pancreatitis or a pancreatic pseudocyst; however, bleeding occurs in only approximately 5% of patients.
The diagnosis of sinistral portal hypertension is achieved by a combination of gastroscopy, liver function tests, ultrasound examination (with Doppler) and/or contrast-enhanced CT scan of the abdomen.
A mere demonstration of sinistral portal hypertension does not warrant intervention. An expectant management is justifiable in asymptomatic patients with pancreatitis. However, concomitant splenectomy may be considered in patients undergoing operative treatment of symptomatic chronic pancreatitis if sinistral portal hypertension and gastroesophageal varices are present.
In patients presenting with gastric variceal hemorrhage, splenectomy (with treatment for the primary pancreatic pathology, e.g. distal pancreatectomy) is curative with excellent long term results.
References
- Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology 1992; 16:1343-9. [PMID 1446890]
- Evans GR, Yellin AE, Weaver FA, Stain SC. Sinistral (left-sided) portal hypertension. Am Surg 1990; 56:758-63. [PMID 2268102]
- Loftus JP, Nagorney DM, Ilstrup D, Kunselman AR. Sinistral portal hypertension. Splenectomy or expectant management. Ann Surg 1993; 217:35-40. [PMID 8424698]
- Heider TR, Azeem Samreen,Galanko JA, Behrns KE. The natural history of pancreatitis induced splenic vein thrombosis. Ann Surg 2004; 239:876-82. [PMID 15166967]
- Sakorafas GH, Sarr MG, Farley DR, Farnell MB. The significance of sinistral portal hypertension complicating chronic pancreatitis. Am J Surg 2000; 179:129-33. [PMID 10773149]
- Iwasaki T, Nagata Y, Watahiki H,Yamamoto H,Ogawa H. A rare case of serous cystadenoma of the pancreas presenting with left-sided portal hypertension. Surg Today 1996; 26:442-5. [PMID 8782305]
- Takase M, Suda K, Suzuki F, Nakamura T, Futagawa S. A histopathologic study of localized portal hypertension as a consequence of chronic pancreatitis. Arch Pathol Lab Med 1997; 121:612-4. [PMID 9199628]
- Little AG, Moossa AR. Gastrointestinal hemorrhage from left-sided portal hypertension. An unappreciated complication of pancreatitis. Am J Surg 1981; 141:153-8. [PMID 6970001]
- Smith TA, Brand EJ. Pancreatic cancer presenting as bleeding gastric varices. J Clin Gastroenterol 2001; 32:444-7. [PMID 11319321]
- Kakizaki S, Hamada T, Yoshinaga T, Higuchi T, Kashiwabara K, Takagi H, Mori M. Alcoholic chronic pancreatitis with simultaneous multiple severe complications. Extrahepatic portal obliteration, obstructive jaundice and duodenal stricture. Hepatogastroenterology 2005; 52:1274-7. [PMID 16001677]

