Case Report - (2025) Volume 9, Issue 5
Pediatric Ulcerative Colitis with Concurrent Budd-Chiari Syndrome: A Rare Case Study
Ghayda Alwahbi*
Department of Pathology, College of Medicine, Qassim University, Buraidah, Saudi Arabia
*Correspondence:
Ghayda Alwahbi, Department of Pathology, College of Medicine, Qassim University, Buraidah,
Saudi Arabia,
Email:
Received: 20-Oct-2024, Manuscript No. IPJCGH-24-21781;
Editor assigned: 22-Oct-2024, Pre QC No. IPJCGH-24-21781 (PQ);
Reviewed: 05-Nov-2024, QC No. IPJCGH-24-21781;
Revised: 16-Oct-2025, Manuscript No. IPJCGH-24-21781 (R);
Published:
23-Oct-2025, DOI: 10.36648/2575-7733.9.5.41
Abstract
This look at opinions a case of a 7-12 months-old female admitted with bloody diarrhea and stomach ache, who turned into sooner or later diagnosed with Budd-Chiari Syndrome (BCS) in the context of Ulcerative Colitis (UC). Medical exam revealed hepatomegaly and ascites, and laboratory assessments confirmed severe anemia and slight leukocytosis. Endoscopy confirmed pancolitis. Initial treatment with heparin and methylprednisolone became powerful, but a relapse befell during steroid weaning, necessitating anti-TNF remedy. That is one of the youngest said instances of BCS related to UC, highlighting the significance of early and multidisciplinary management in such complicated instances.
Keywords
Gut microbiome; Immune system; Gastrointestinal disorders; Gastroesophageal reflux disease
Introduction
Ulcerative colitis is a continual Inflammatory Bowel Ailment (IBD) characterised by mucosal inflammation of the colon and rectum. Budd-Chiari syndrome is a sickness resulting from hepatic venous outflow obstruction. despite the fact that rare, it is a clinically massive complication, mainly in sufferers with underlying inflammatory bowel disorder including ulcerative colitis [1].
This pursuit to research a case study of a 7-12 months-old affected person providing with a unique mixture of BCS and UC, emphasizing the diagnostic demanding situations, management strategies, and underlying pathophysiology.
Pediatric Ulcerative Colitis (UC) is a persistent Inflammatory Bowel Sickness (IBD) characterised through irritation and ulceration of the colon, mainly affecting kids and youth. At the same time as UC generally presents with signs inclusive of abdominal ache, diarrhea, and rectal bleeding, its extraintestinal manifestations can complicate analysis and control. One such uncommon however serious hardship is Budd-Chiari Syndrome (BCS), a condition characterized by means of the obstruction of hepatic venous outflow, main to liver disorder, ascites, and hepatomegaly.
The coexistence of UC and BCS in a pediatric affected person is distinctly rare, making the medical diagnosis and treatment mainly tough. while each UC and BCS were studied for my part, the simultaneous presence of these conditions in an unmarried patient is scarcely documented, and the underlying pathophysiological mechanisms stay poorly understood. This example looks at targets to discover the diagnostic adventure, scientific presentation, and control techniques for a pediatric affected person diagnosed with each UC and concurrent BCS. Moreover, it highlights the importance of thinking about uncommon greater-intestinal headaches in pediatric IBD, as early popularity and spark off intervention are crucial for improving affected person outcomes.
Through this case report, we seek to contribute to the growing body of literature on complex and rare presentations of pediatric diseases, emphasizing the need for heightened clinical vigilance and a multidisciplinary approach in treatment.
Case Presentation
The patient, a 7-year-old girl, presented with a 2-day history of bloody diarrhea and abdominal pain, alongside a 1-week history of intermittent diarrhea with a Pediatric Ulcerative Colitis Activity Index (PUCAI) score of 70, indicating severe disease. Clinical examination revealed hepatomegaly and ascites (Figure 1). Laboratory investigations showed the following results (Table 1). Endoscopy showed pancolitis with a Mayo score of 3. Patient was on heparin therapy and IV methylprednisolone, with a good response within days (PUCAI score 15). However, during steroid weaning and maintenance with 5-ASA, the patient relapsed and required the initiation of anti-TNF therapy. Her abdominal distension decreased over days, but the liver size remained unchanged [2-5].
| Parameter |
Result |
Normal range |
Interpretation |
| Hemoglobin |
5.5 g/dL |
11.5-15.5 g/dL |
Severe anemia |
| White blood cell count |
9.1 × 109/L |
4.0-10.5 × 109/L |
Mild leukocytosis |
| Platelet count |
362 × 109/L |
150-400 × 109/L |
Normal |
| Erythrocyte Sedimentation Rate (ESR) |
95 mm/h |
0-20 mm/h |
Markedly elevated |
| Alanine Aminotransferase (ALT) |
11 U/L |
7-56 U/L |
Normal |
| Aspartate Aminotransferase (AST) |
22 U/L |
10-40 U/L |
Normal |
| Albumin |
32 g/L (slightly low) |
35-50 g/L |
Slightly low |
| Total bilirubin |
12 µmol/L |
1.2-20.8 µmol/L |
Normal |
| Thrombophilia workup |
| INR |
Normal |
0.8-1.2 |
No evidence of thrombophilia |
| PT |
Normal |
11-14 seconds |
|
| aPTT |
Normal |
25-35 seconds |
|
| Protein C and S |
Normal |
|
|
| Antiphospholipid antibodies |
Negative |
|
|
Table 1: Laboratory investigations.
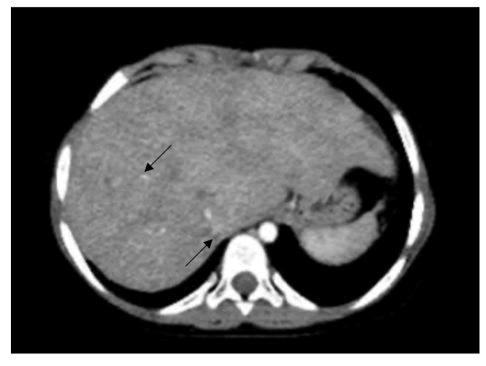
Figure 1: CT scan showing liver with highlighted areas (arrows), possibly indicating lesions or abnormalities for further medical evaluation.
CT angiography displaying a fairly enlarged liver (14.8 cm) with marked caudate lobe expansion, inhomogeneous evaluation enhancement, attenuated intrahepatic inferior vena cava, and non-visualized hepatic veins.
Results and Discussion
Outcome and Observe Up
The patient accompanied for 18 months. She is on remission (clinical and biochemical proof with the aid of bad CRP and normalized fCal <50) and maintained on infliximab. Enoxaparin became discontinued after 6 months without a recurrence of thrombosis and no worsening of mounted hepatic veins.
The pathophysiology underlying the confluence of BCS and UC involves a complicated interplay among inflammatory approaches, hypercoagulability, and vascular disorder.
Inflammatory mediators feature of UC make a contribution to endothelial injury and activation, predisposing to thrombosis inside hepatic vasculature. Dysregulation of coagulation pathways similarly exacerbates the prothrombotic country in UC, leading to hepatic venous outflow obstruction.
Diagnostic demanding situations in UC-related BCS necessitate an excessive index of suspicion and multimodal imaging strategies. Contrast-stronger imaging strategies play a pivotal function in delineating hepatic vascular anatomy and figuring out thrombotic occlusions feature of BCS [6].
Management of UC-associated BCS requires a multidisciplinary method that specialize in each underlying IBD and hepatic venous outflow obstruction. Healing interventions purpose to mitigate thrombotic threat, alleviate hepatic congestion, and optimize UC manipulate. Anticoagulation stays a cornerstone, frequently supplemented via immunosuppressive sellers and biologic retailers concentrated on inflammatory pathways. Surgical interventions can be indicated in refractory cases or advanced liver ailment.
As we navigate the elaborate labyrinth of UC-associated BCS, it turns into evident that a complete information of the underlying pathophysiology is paramount in guiding healing interventions and optimizing medical consequences. The case study serves as a poignant reminder of the tricky tapestry of irritation and coagulation that defines the medical panorama of UC-related BCS, underscoring the want for a multidisciplinary technique in unraveling the mysteries that lie on the intersection of inflammatory bowel illnesses and hepatic issues.
At some point of evaluation, we be aware all instances pronounced for person patients BCS came after prognosis of UC. even as instances pronounced in pediatric age has comparable concurrence of BCS and UC at identical time of diagnosis.
The convergence of Budd-Chiari Syndrome (BCS) and ulcerative colitis (UC) affords a fascinating intersection of pathophysiological complexities. In the case of the 7-yearantique patient, who presented with a 2-day history of bloody diarrhea and belly ache alongside a 1-week records of intermittent diarrhea, her medical presentation aligns with the pronounced literature, emphasizing the importance of spotting the extraintestinal manifestations of UC, specifically whilst complicated through thrombotic activities including BCS. The diagnostic journey in UC-associated BCS is fraught with demanding situations, necessitating a multidisciplinary method and an excessive index of suspicion. Comparisonimproved imaging strategies play a pivotal position in confirming hepatic venous outflow obstruction, as verified in this case [7].
Comparing the case of the 7-yr-vintage girl with the referred cases, we observe a commonality in the clinical presentation and diagnostic challenges encountered throughout extraordinary age organizations. In spite of variations in age and disease severity, the underlying pathophysiological mechanisms linking UC and BCS remain regular, emphasizing the significance of a comprehensive understanding of the disorder spectrum. The interaction between infection and coagulation in UC-related BCS transcends character instances, underscoring the want for tailor-made healing interventions focused on each inflammatory pathways and thrombotic threat elements [8].
The supplied case of the 7-year-vintage lady serves as a poignant instance of the complicated interaction among UC and BCS, highlighting the diagnostic demanding situations, pathophysiological mechanisms, and healing issues inherent on this complicated scientific entity. By way of evaluating her case with the referred cases, we gain a broader attitude at the sickness spectrum and the underlying pathophysiology, paving the manner for optimized scientific control strategies [9].
Conclusion
This example has a look at highlights the complex dating among UC and BCS, emphasizing the want for early reputation and accurate diagnosis. The evaluation of the patient's presentation and underlying pathophysiology underscores the importance of a multidisciplinary approach in handling UC-associated BCS. We emphasize the crucial importance of prompt initiation of appropriate management techniques to optimize medical effects in this specific affected person populace.
Affected Person Consent
Knowledgeable consent changed into received from the patient's guardians for the publication of this situation file. identifying facts has been anonymized to defend the patient's privacy.
References
- Socha P, Ryzko J, Janczyk W, Dzik E, Iwanczak B, et al. (2007) Hepatic vein thrombosis as a complication of ulcerative colitis in a 12-year-old patient. Dig Dis Sci. 52(5):1293-1298.
[Crossref] [Google Scholar] [PubMed]
- Yılmaz B, Köklü S, Bayraktar Y (2013) Ulcerative colitis presenting with Budd-Chiari syndrome. J Crohns Colitis. 7(2).
[Crossref] [Google Scholar] [PubMed]
- Hendrickson BA, Gokhale R, Cho JH (2002) Clinical aspects and pathophysiology of inflammatory bowel disease. Clin Microbiol Rev. 15(1):79-94.
[Crossref] [Google Scholar] [PubMed]
- Horsthuis K, Stokkers PC, Stoker J (2008) Detection of inflammatory bowel disease: diagnostic performance of cross-sectional imaging modalities. Abdom Imaging. 33(4):407-416.
[Crossref] [Google Scholar] [PubMed]
- Bohra GK, Chhabra V, Midha N, Sureka B (2018) Budd-Chiari syndrome in a patient with ulcerative colitis. BMJ Case Rep.
[Crossref] [Google Scholar] [PubMed]
- Menon KV, Shah V, Kamath PS (2004) The Budd-Chiari syndrome. N Engl J Med. 350(6):578-585.
[Crossref] [Google Scholar] [PubMed]
- Schoepfer AM, Tran VDC, Rossel JB, Sokollik C, Spalinger J, et al. (2021) Impact of diagnostic delay on disease course in pediatric-versus adult-onset patients with ulcerative colitis: Data from the Swiss IBD Cohort. Inflamm Intest Dis. 7(2):87-96.
[Crossref] [Google Scholar] [PubMed]
- Marchetti F, Mainetti M, Giovannini M, Morelli C (2017) Budd-Chiari syndrome and ulcerative colitis in an adolescent. Recenti Prog Med. 108(5):242-245.
[Crossref] [Google Scholar]
- Jaqua NT, Stratton A, Yaccobe L, Tahir U, Kenny P, et al. (2013) A review of the literature on three extraintestinal complications of ulcerative colitis: an ulcerative colitis flare complicated by Budd-Chiari syndrome, cerebral venous thrombosis and idiopathic thrombocytopenia. Acta Gastroenterol Belg. 76(3):311-316.
[Google Scholar] [PubMed]
Citation: Alwahbi G (2025) Pediatric Ulcerative Colitis with Concurrent Budd-Chiari Syndrome: A Rare Case Study. J Clin
Gastroenterol Hepatol. 9:41.
Copyright: © 2025 Alwahbi G. This is an open-access article distributed under the terms of the Creative Commons Attribution
License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source
are credited.

