Keywords
Abdominal Injuries; Drainage; Firearms; Pancreatitis, Acute Necrotizing; Wounds and Injuries
INTRODUCTION
Shotgun injuries, although rare in the European Union, are the cause of increasing surgical problems related to the proliferation of firearms, civilian crime and terrorism in peace time [1, 2], and may lead to severe trauma disease and even to death, usually due to hemorrhagic shock. Prognosis is significantly worse in the presence of multiorgan injuries [3]. Gunshot pancreaticoduodenal injuries are relatively unusual, but not rare in urban trauma units. Their management remains complex because of the absence of standardized, universal guidelines for treatment [4], and the high incidence of associated lesions of major vessels and of other gastrointestinal structures [5]. Therefore, surgical treatment is still controversial, ranging from primary sutures to pancreaticoduodenectomy [6].
The possibilities offered by safe and effective mini-invasive techniques seem to open new, articulated perspectives for the treatment of pancreaticoduodenal injury complications, such as fluid collection and pancreatitis [7, 8]. We present the case of a patient with multiple penetrating gunshot trauma evolving into acute necrotizing pancreatitis, treated by combining a surgical with a mini-invasive approach.
CASE REPORT
A 27-year-old man was evaluated in the emergency room for multiple penetrating abdominal, thoracic and cranio-facial gunshot injuries. At admission, he presented a Glasgow Coma Score of 4 due to severe hemorrhagic shock. A total-body CT scan revealed maxillo-ethmoidal fractures with a detained projectile, bilateral massive hemothorax and large pulmonary contusions, with a bullet in the spinal canal at level of T3, and multiple costal and scapular fractures. A diffuse hemoperitoneum, a large intrahepatic hematoma of the right lobe with liver laceration and an active bleeding lesion of the pancreatic-duodenal artery were evident (Figure 1). Moreover, two bullets were observed in the posterior abdominal wall (Figure 2) and in the pelvic floor, respectively.
Figure 1. CT scan: active hemorrhage by lesion of
pancreatic-duodenal artery (white arrows), liver
laceration (black arrow) and hemoperitoneum (*).
Figure 2. CT scan shows retained firearm bullet (arrow
head) which caused: hemorrhage by lesion of
pancreatic-duodenal artery (white arrows), liver
laceration (black arrow) and hemoperitoneum (*).
The emergency laparotomy confirmed the massive hemoperitoneum and revealed diffused bile spillage, a large intracapsular hematoma of the right lobe of the liver, a hematoma of the pancreatic head, a jejunal perforation 2 cm from the Treitz ligament, and further small bowel (Figure 3) and mesenterial perforations. Moreover, the superior flexure of the duodenum was perforated, and a laceration of the duodenal inferior flexure was evident (Figure 4). Liver mobilization with inspection of the intracapsular hematoma and a wide Kocher maneuver with a primary two-layer closure of the duodenal laceration were performed. Hemostatic suture of the superior branches of the pancreaticoduodenal artery was necessary in order to stop the bleeding causing the hemoperitoneum. A Billroth II procedure with a gastroenteroanastomosis constructed with a jejunal loop of 60 cm from the Treitz ligament and a distal Braun enteroenteroanastomosis were performed. A jejunal resection was also required, and a mechanical jejunojejunal terminolateral anastomosis was constructed 2 cm below the Treitz ligament with an EEA 25 stapler (Ethicon, Cincinnati, OH, U.S.A.). Two abdominal drains in proximity of the duodenal stump and the Treitz ligament, and one pelvic drain were positioned. Double thoracic drainage and removal of the bullet from the ethmoidal cells were also carried out.
Figure 3. Emergency laparotomy: two small bowel
perforations (black arrows) are shown.
Figure 4. Emergency laparotomy: a wide laceration of
the inferior flexure of the duodenum is shown.
In the immediate postoperative period, a CT scan and neurosurgical re-evaluation showed a severe nervous lesion at the level of the T3 causing paraplegia, secondary to the bullet retained in the spinal canal. Owing to prolonged ventilation, a tracheostomy had to be performed on the 6th postoperative day. Perioperative intravenous fluids and colloids, antibiotics including cefalosporin, metronidazole and aminoglycoside, total parenteral nutrition and inhibitor of the pancreatic secretion were administered.
On the 12th postoperative day, bilioenteric fluid was observed from the right drainage tube; a CT scan showed perihepatic and perisplenic fluid collection extending into the pancreatic space; laboratory investigation revealed leucocytosis and increased serum levels of amylases, lipases and bilirubin. The same high values were demonstrated in the fluid collected from the drainage tube.
Re-laparotomy showed a considerable amount
of peritoneal exudate in the peripancreatic
region; the head and body of the pancreas
were involved in a massive inflammatory
process producing wide areas of necrosis
(Figure 5). Inflammatory disease consistent
with pancreatitis involved the duodenal
stump, with a discontinuance measuring 1 cm
in diameter and located 2 cm forward of the
stapler suture. All the anastomoses were
undamaged and well healed. A clearing of the
pancreatic space was performed; a Foley
catheter (n. 14), secured by a tobacco bag
suture, was inserted through the duodenal
perforation (Figure 6) and three drainage
tubes were positioned.
Figure 5. Emergency re-laparotomy: the pancreatic
head (indicated by the tips of a dissection forceps) and
body (depressed by the finger of the surgeon) are
involved in a massive inflammatory process producing
wide areas of necrosis.
Figure 6. Emergency re-laparotomy: a Foley catheter
is inserted through the duodenal perforation.
On the 6th postoperative day, the patient was extubated from mechanical ventilation; two days later, following the accidental removal of two peripancreatic drains, fever, leucocytosis and abdominal distension appeared. A CT scan showed a considerable and moderately homogeneous fluid collection (15-25 Hounsfield units) in the epiploic retrocavity (Figure 7); consequently, percutaneous CT-guided drainage was performed by inserting an 8.5 Fr pigtail catheter with one-shot technique (Figure 8). Pseudomonas aeruginosa and Staphilococcus haemoliticus bacteria infected the pancreatic juice collected by the percutaneous drainage, confirming the diagnosis of infected necrotizing acute pancreatitis.
Figure 7. CT scan: peripancreatic fluid collections (*)
reaching the anterior abdominal wall (arrow).
Figure 8. CT guidance percutaneous 10 French pigtail
drainage was positioned into the fluid collection (*).
Two days later the patient with tracheostomy was moved from the intensive care unit to our surgical unit. As the postoperative period continued, the acute necrotizing pancreatitis evolved into a pancreatic fistula with an initial mean output of 350 mL/day which was treated by conservative management (Figure 9). Thirty-nine days after re-surgery, the tracheostomy was closed and, six days later, the patient started a light diet; the Foley in the duodenum was removed 58 days after its insertion, and the patient was discharged 80 days after the gunshot trauma. Two months after the complete resolution of the pancreatic fistula, the pigtail catheter was removed (Figure 10). Eighteen months later the patient is well despite paraplegia.
Figure 9. After 15 days with the catheter in place, the
fluid collection (*) has diminished in size.
Figure 10. A final CT scan with post-processing multiplanar
reconstruction was helpful in confirming
complete resolution of the fluid collection after catheter
removal.
DISCUSSION
An incidence of penetrating injuries in the pancreas, ranging from 1 to 12%, has been reported in the literature; combined pancreaticoduodenal lesions are rare and account for less than 10% of pancreatic injuries [9, 10]. Gunshot wounds of the duodenum and pancreas cause most pancreaticoduodenal injuries [5].
Duodenal and pancreatic traumas are associated with a variety of other serious lesions in 45-85% of cases [11, 12] and overall morbidity and mortality ranging from 30 to 100% and 9 to 50%, respectively, have been reported in various series [5, 9]. The optimal management of penetrating duodenopancreatic lesions continues to be a matter of debate and controversy. Although discordant opinions were reported in the literature regarding pyloric exclusion [13, 14], this procedure and drainage of the pancreas are the mainstays of surgical treatment [15, 16].
The site of the duodenal injury is crucial for determining the surgical approach, aiming not only at reconstructing duodenal continuity but also at avoiding suture line dehiscence [4]. Laceration of the duodenal bulb or superior flexure of the duodenum can be safely treated with gastric resection and by closure of the duodenal stump. When the injury is just below the ampulla of Vater, however, resection of the damage may be difficult. Mucosal or serosal patches and a pedicled graft with a free vascular pedicle created from stomach, jejunum or ileum tissue have been previously proposed without proven efficacy [5, 17, 18, 19]. Duodenal drainage with a decompression tube, gastrojejunostomy, feeding jejunostomy, gastric resection with external duodenal drainage with Foley or Petzer tubes have also been recommended with conflicting reports of efficacy [20, 21, 22, 23].
In the presence of a duodenal lesion ranging from 50 to 70% of the circumference, Rouxen- Y duodenojejunostomy and duodenopancreatectomy procedures have also been proposed [23, 24], but with increased risk of dehiscence in cases of sepsis and peritonitis. However, duodenal resection should be carried out when duodenal continuity or vascularization is interrupted; two procedures are currently being used. Resection of the duodenum with a primary end-to-end anastomosis should be performed in case of injury to the first, third and fourth segments. On the other hand, a pancreaticoduodenectomy should be reserved for selected cases of ampullary or proximal pancreatic duct injuries, massive peripancreatic hemorrhage and severe lesions of the duodenum and head of the pancreas [5, 25].
Therefore, when the pancreas is simultaneously involved in the gunshot damage, management is even more complex. Surgical management depends on the degree and location of the parenchymal lesion as well as on the presumed or evident integrity of the pancreatic duct [9]. Indeed, Bradley et al. [26] showed a significant association between injury to the main pancreatic duct and pancreas-related morbidity; furthermore, the overall morbidity is increased by delayed diagnosis and intervention [26, 27].
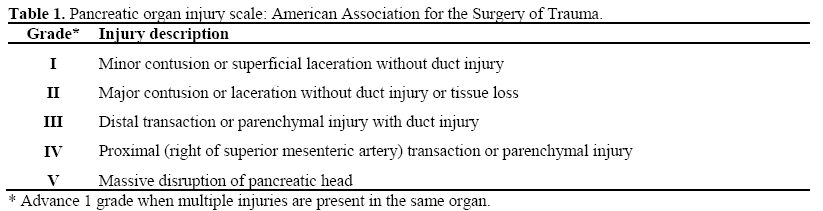
Surgical procedures, such as duodenopancreatectomy, segmental or total pancreatectomy, show high morbidity and mortality, especially in emergency setting and in the presence of multiple traumas [28]. Moreover, radical procedures may be contraindicated for the hemodynamic and metabolic conditions of these patients, often suffering from physiological pathologies such as dilutional coagulopathy, hypothermia and acidosis, the so called “killer triad” [29, 30].The current opinion is that the appropriate treatment of the pancreatic trauma should be performed according to the type of injury (Table 1). Grade I and grade II injuries should be managed by hemostasis, debridement of devitalised tissue and adequate external drainage [9, 31]. The temptation to repair capsular laceration should be avoided because this may result in pseudocyst formation [9]. Grade III injuries require a distal pancreatectomy with closed suction drainage [9]. Grade IV and V injuries are frequently associated with multiple life-threatening traumas and generally require a damagecontrol approach with packing and wide external drainage [9].
Grade II pancreatic injury management associated with a Billroth II procedure and a jejunal resection was performed in the first operation in the case reported, but the appearance of a duodenal perforation due to severe posttraumatic necrotizing pancreatitis required an emergency re-laparotomy. Indeed, in pancreaticoduodenal trauma, the need for re-laparotomy due to postoperative complications is frequently reported in the literature, accounting for an average of 2-5 operations for the patients [5, 11, 32].
The main postoperative complications requiring re-operation are duodenal and pancreatic related. The major duodenumrelated complications are duodenal fistula and duodenal obstruction, ranging from 0 to 17% and from 1 to 1.8%, respectively [5, 33]. The pancreatic-related complications consist of pancreatic fistula (20-26%), intra-abdominal abscess (9-17%) and pseudocyst formation (5- 15%) [34, 35, 36, 37], but pancreatitis is the prevailing postoperative complication, occurring in 30-72% of cases and representing the main reason for mortality in pancreatic trauma [12, 38, 39].
Acute necrotizing pancreatitis is an objective diagnosis following contrast-enhanced CT which determines the extent of the necrosis and fluid collection, serially monitoring the progress; the diagnosis of the evolution of pancreatic necrosis into infection follows a positive culture or a CT scan showing gas pockets in and around the lesion.
Open pancreatic necrosectomy remains an important treatment for managing necrotizing pancreatitis, but mortality after debridement continues to be inordinately high [40, 41]. Mortality rates ranging from 20 to 70% have actually been reported in the literature, with sepsis and multiorgan failure as the most frequent causes [42, 43, 44, 45]. Moreover, a higher mortality rate was observed in patients with an increased APACHE II score, early persistent SIRS and unresolved multiorgan dysfunction [41].
In this report, the management complexity increased due to the accidental peripancreatic drain removal which forced further intervention.
Although recently minimally invasive necrosectomy techniques have been tried with satisfying results [46, 47, 48], they frequently necessitate multiple sessions for a definitive toilette [43] and have not been feasible in previous abdominal surgery for traumas. However, in the last decade, percutaneous CT-guided catheter drainage has been included in the management of necrotizing pancreatitis, even if the existing literature is limited [7, 42, 49].
Ultrasound or CT-guided drainage placement is reportedly effective in up to 90% of cases for drainage of acute fluid collections, pseudocysts or abscesses with a purely liquid content [42, 50]. Nevertheless, success rates for the drainage of contained fluid collection in necrotizing pancreatitis ranges from 26 to 50% because the infected collections are often not completely liquid and the possibility of removing the solid debris therein contained is equivocal [42, 49, 51]. The use of large bore catheters and the placement of several drainages has not yet been demonstrated definitively, and a prospective study seems to be necessary in order to evaluate the impact of drainage characteristics [42, 52].
However, percutaneous drainage allows a significant temporizing effect, especially in critically ill patients, postponing surgical intervention and leading to full recovery in several cases [49, 53, 54].
In conclusion, the treatment is successful when it is tailored to the clinical needs of the patient, especially if there are severe concomitant injuries or a prolonged course of treatment. As in the case reported, percutaneous drainage with targeted antibiotic therapy, based on bacterial cultures from FNA, should also be considered in all critically ill patients with post-traumatic necrotizing pancreatitis in order to avoid further hazardous surgical revision burdened by a high morbidity and mortality rates [42, 43, 44, 45]. Efforts to reduce mortality among patients with multiple pancreaticoduodenal penetrating gunshot traumas should focus on multidisciplinary surgical and minimally invasive treatment to optimize organ recovery.
Conflict of interest
The authors have no potential conflicts of interest
References
- Figl M, Weninger P, Hertz H. Gunshot Injuries - Incidence and Treatment. ZentralblChir 2007; 132:365-71. [PMID 17724642]
- Witkowski Z, Lasek J, Kopiszka K, Stasiak M. Shotgun injuries--epidemiological and clinical aspects. WiadLek 2006; 59:341-5. [PMID 17017479]
- Vasquez JC, Coimbra R, Hoyt DB, Fortlage D. Management of penetrating pancreatic trauma: an 11- year experience of a level-1 trauma center. Injury 2001; 32:753-9. [PMID 11754881]
- Testini M, Piccinni G, Lissidini G, Di Venere B, Gurrado A, Poli E, et al. Management of Descending Duodenal Injuries Secondary to Laparoscopic Cholecystectomy. Dig Surg 2008; 25:12-15. [PMID 18235191]
- Talving P, Nicol AJ, Navsaria PH. Civilian duodenal gunshot wounds: surgical management made simpler. World J Surg 2006; 30:488-94. [PMID 16547621]
- Asensio JA, Stewart BM, Demetriades D. Duodenum. In: Ivatury RR, Cayten CG (editors). The Textbook of Penetrating trauma. Baltimore, Williams & Wilkins, 1996, p. 160.
- Segal D, Mortele KJ, Banks PA, Silverman SG. Acute necrotizing pancreatitis: role of CT-guided percutaneous catheter drainage. Abdom Imaging 2007; 32:351-61. [PMID 17502982]
- Lee JK, Kwak KK, Park JK, Yoon WJ, Lee SH, Ryu JK, et al. The efficacy of nonsurgical tratment of infected pancreatic necrosis. Pancreas 2007; 34:399- 404. [PMID 17446837]
- Al-Ahmadi K, Ahmed N. Outcomes after pancreatic trauma: experience at a single institution. Can J Surg 2008; 51:118-24. [PMID 18377752]
- Kao LS, Bulger EM, Parks DL, Byrd GF, Jurkovich GJ. Predictors of morbidity after traumatic pancreatic injury. J Trauma 2003; 55:898-905. [PMID 14608163]
- Lopez PP, Benjamin R, Cockburn M, Amortegui JD, Schulman CI, Soffer D, et al. Recent trends in themanagement of combined pancreatoduodenal injuries. Am Surg 2005; 71:847-52. [PMID 16468533]
- Ivanov PA, Grishin AV, Korneev DA, Ziniakov SA. Injuries of Pancreaticoduodenal organs. Khirurgiia (Mosk) 2003; 12:39-43. [PMID 14671603]
- Velmahos GC, Constantinou C, Kasotakis G. Safety of repair for severe duodenal injuries. World J Surg 2008; 32:7-12. [PMID 17952703]
- Seamon MJ, Pieri PG, Fisher CA, Gaughan J, Santora TA, Pathak AS, et al. A ten-year retrospective review: does pyloric exclusion improve clinical outcome after penetrating duodenal and combined pancreaticoduodenal injuries? J Trauma 2007; 62:829- 33. [PMID 17426536]
- Mansour MA, Moore JB, Moore EE, Moore FA. Conservative management of combined pancreaticoduodenal injuries. Am J Surg 1989; 158:531-5. [PMID 2589583]
- Hwang SY, Choi YC. Prognostic determinants in patients with traumatic pancreatic injuries. J Korean Med Sci 2008; 23:126-30. [PMID 18303212]
- De Shazo CV, Snyder WH, Daugherty CG, Crenshaw CA. Mucosal pedicle graft or jejunum for large gastrointestinal defects. Am J Surg 1972; 124:671-672. [PMID 5079805]
- Papachristou DN, Fortner JG. Reconstruction of duodenal wall defects with the use of a gastric "island" flap. Arch Surg 1977; 112:199-200. [PMID 851478]
- Walley BD, Goco I. Duodenal patch grafting. Am J Surg 1980; 140:706-708. [PMID 7435834]
- Jones SA, Gazzaniga AB, Keller TB. The serosal patch: a surgical parachute. Am J Surg 1973; 126:186- 196. [PMID 4721542]
- Snyder WH 3rd, Weigelt JA, Watkins WL, Bietz DS. The surgical management of duodenal trauma. Precepts based on a review of 247 cases. Arch Surg 1980; 115:422-9. [PMID 7362449]
- Ivatury RR, Gaudino J, Ascher E, Nallathambi M, Ramirez-Schon G, Stahl WM. Treatment of penetrating duodenal injuries: primary repair vs. repair with decompressiveenterostomy/serosal patch. J Trauma 1985; 25:337-341. [PMID 4046085]
- Carrillo EH, Richardson DJ, Miller FB. Evolution in the management of duodenal injuries. J Trauma 1996; 40:1037-45. [PMID 8656463]
- Cogbill TH, Moore EE, Feliciano DV, Hoyt DB, Jurkovich GJ, Morris JA, et al. Conservative management of duodenal trauma: a multicenter perspective. J Trauma 1990; 30:1469-75. [PMID 2258957]
- Ivatury RR. Duodenal injuries: small but lethal lesions. Cir Gen 2003; 25:59-64.
- Bradley EL III, Young PR Jr, Chang MC, Allen JE, Baker CC, Meredith W, et al. Diagnosis and initial management of blunt pancreatic trauma:guidelines from a multiinstitutional review. Ann Sur 1998; 227:861-9. [PMID 9637549]
- Oniscu GC, Parks RW, Garden OJ. Classification of liver and pancreatic trauma. HPB (Oxford) 2006; 8:4-9. [PMID 18333232]
- Aldemir M, Taçyildiz I, Girgin S. Predicting factors for mortality in the penetrating abdominal trauma. Acta ChirBelg 2004; 104:429-434. [PMID 15469156]
- Rotondo MF, Schwab CW, McGonigal MD, Phillips GR 3rd, Fruchterman TM, Kauder DR, et al. 'Damage control': an approach for improved survival in exsanguinating penetrating abdominal injury. J Trauma 1993; 35:375-82. [PMID 8371295]
- Stawicki SP, Brooks A, Bilski T, Scaff D, Gupta R, Schwab CW, Gracias VH. The concept of damage control: Extending the paradigm to emergency general surgery. Injury 2008; 39:93-101. [PMID 17888435]
- Boffard KD, Brooks AJ. Pancreatic trauma: injury to the pancreas and pancreatic duct. Eur J Surg 2000; 166:4-12. [PMID 10688209]
- Rickard MJ, Brohi K, Bautz PC. Pancreatic and duodenal injuries: keep it simple. Anz J Surg 2005; 75:581-6. [PMID 15972052]
- Asensio JA, Feliciano DV, Britt LD, Kerstein MD. Management of duodenal injuries. CurrProblSurg 1993; 11:1023-93. [PMID 8222749]
- Mayer JM, Tomczak R, Rau B, Gebhard F, Beger HG. Pancreatic injury in severe trauma: early diagnosis and therapy improve the outcome. Dig Surg 2002; 19:291-7. [PMID 12207073]
- el-Boghdadly S, al-Yousef Z, al Bedah K. Pancreatic injury: an audit and a practical approach. Ann R CollSurgEngl 2000; 82:258-62. [PMID 10932660]
- Feliciano DV, Martin TD, Cruse PA, Graham JM, Burch JM, Mattox KL, et al. Management of combined pancreaticoduodenal injuries. Ann Surg 1987; 205:673- 80. [PMID 3592810]
- Cerwenka H, Bacher H, El-Shabrawi A, Kornprat P, Lemmerer M, Portugaller HR, Mischinger HJ. Management of pancreatic trauma and ist consequences-guidelines or individual therapy? Hepatogastroenterology 2007; 54:581-4. [PMID 17523326]
- Eramishantsev AK, Molitvoslovov AB, Filin AV. Traumatic injuries of the pancreas. Khirurgiia (Mosk) 1994; 4:13-7. [PMID 8041063]
- Faroudy M, Mosadik A, Mouelhi S, Ababou A, Lazreq C, Sbihi A. The post-traumatic pancreatitis: about four cases. Ann FrAnesthReanim 2006; 25:652- 6. [PMID 16546346]
- Rodriguez JR, Razo AO, Targarona J, Thayer SP, Rattner DW, Warshaw AL, et al. Debridement and closed packing for sterile or infected necrotizing pancreatitis: insights into indications and outcomes in 167 patients. Ann Surg 2008; 247:294-9. [PMID 18216536]
- Mofidi R, Lee AC, Madhavan KK, Garden OJ, Parks RW. Prognostic factors in patients undergoing surgery for severe necrotizing pancreatitis. World J Surg 2007; 31:2002-7. [PMID 17687599]
- Bruennler T, Langgartner J, Lang S, Wrede CE, Klebl F, Zierhut S, et al. Outcome of patients with acute, necrotizing pancreatitis requiring drainage-does drainage size matter? World J gastroenterol 2008; 14:725-30. [PMID 18205262]
- Connor S, Ghaneh P, Raraty M, Rosso E, Hartley MN, Garvey C, et al. Increasing age and APACHE II score are the main determinants of outcome from pancreatic necrosectomy. Br J Surg 2003; 90:1542-8. [PMID 14648734]
- Beger HG, Rau B, Isenmann R. Natural history of necrotizing pancreatitis. Pancreatology 2003; 3:93-101. [PMID 12774801]
- Banks PA, Freeman ML. Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-400. [PMID 17032204]
- Bucher P, Pugin F, Morel P. Minimally invasive necrosectomy for infected necrotizing pancreatitis. Pancreas 2008; 36:113-9. [PMID 18376300]
- Castellanos G, Piñero A, Serrano A, Llamas C, Fuster M, Fernandez JA, Parrilla P. Translumbar retroperitoneal endoscopy: an alternative in the followup and management of drained infected pancreatic necrosis. Arch Surg 2005; 140:952-5. [PMID 16230544]
- Carter R. Management of infected necrosis secondary to acute pancreatitis: a balancd role for minimal access techniques. Pancreatology 2003; 3:133- 8. PMID 12774803]
- Freeny PC, Hauptmann E, Althaus SJ, Traverso LW, Sinanan M. Percutaneous CT-guided drainage of infected acute necrotizing pancreatitis: techniques and results. AJR Am J Roentgenol 1998; 170:969-75. [PMID 9530046]
- vanSonenberg E, Wittich GR, Goodacre BW, Casola G, D'Agostino HB. Percutaneous abscess drainage: update. World J Surg 2001; 25:362-9. [PMID 11343195]
- Szentkereszty Z, Kerekes L, Hallay J, Czako D, Sápy P. CT-guided percutaneous peripancreatic drainage: a possible therapy in acute necrotizing pancreatitis. Hepatogastroenterology 2002; 49:1696-8. [PMID 12397769]
- Szentkereszty Z, Sapy P. The role of percutaneous external drainage in the treatment of fluid collections associated with severe acute pancreatitis. What, when and how to drain? OrvHetil 2007; 148:1395-9. [PMID 17631476]
- Cheung MT, Ho CN, Siu KW, Kwork PC. Percutaneous drainage and necrosectomy in the management of pancreatic necrosis. Anz J Surg 2005; 75:204-7. [PMID 15839965]
- Echenique AM, Sleeman D, Yrizarry J, Scagnelli T, Guerra JJ Jr, Casillas VJ, et al. Percutaneous catheter-directed débridement of infected pancreatic necrosis: results in 20 patients. J VascIntervRadiol 1998; 9:565-71. [PMID 9684824]











