Vikas Gupta1, Vikash Moond1, Santhosh Irrinki1, Ashwini Sood2, Ajay Gulati3, Amanjit Bal4, KimVaiphei4, Saroj K Sinha5, Rakesh Kochhar5
Department of General Surgery1, Nuclear Medicine2, Radiodiagnosis3, Pathology4 and Gastroenterology5, Postgraduate Institute of Medical Education and Research, Chandigarh 160012, India
- *Corresponding Author:
- Vikas Gupta
Postgarduate Iinstitute of Medical Education and Research
General surgery, Sector 12
Chandigarh, 160012, India
Tel + 9872041120
E-mail vikaspgi@gmail.com
Received March 04th, 2018 - Accepted June 25th, 2018
Keywords
Pancreatic Neoplasms; Paraganglioma
INTRODUCTION
Multicentric pancreatic neoplasm though rare can be
encountered in patients with neuroendocrine tumors,
cystic neoplasms, synchronous pancreatic adenocarcinoma
or metastatic lesion from other organs [1]. These lesions
offer a unique challenge to the surgeon with respect to the
surgical procedure to be performed. The balance between
radical resection and post-operative quality of life has to
be considered. Conventionally total Pancreatectomy was
the surgical option for multi focal pancreatic neoplasm,
however it is associated with impaired functional outcome
in terms of long term exocrine and endocrine insufficiency
[2]. Parenchyma preserving pancreatic resection for
multiple and low grade lesion has been described to
circumvate the functional consequences associated with
total pancreatectomy. These may vary from enucleation
to segmental resection to preservation of small pancreatic
segment. Middle preserving pancreatectomy is an attractive option in such patients [3]. Ever since its first description
in 1999, only 26 cases has been reported in the English
literature so far. Middle Preserving Pancreatectomy is
a rare surgical procedure mainly due to lack of suitable
cases. We hereby report our experience with two cases
of middle preserving pancreatectomy performed over a
period of seven years.
METHODOLGY AND RESULTS
The present study describes two patients who
underwent Middle preserving Pancreatectomy for multi
centric pancreatic neoplasm. From January 2011 to
December 2017 two patients undergoing middle preserving
pancreatectomy were reviewed retrospectively.
Demographic, biochemical, radiological, operative and
follow up data were retrieved. During the study period a
total of 308 pancreatic resection were performed which
included 276 pancreatico-duodenectomies, 27 distal
pancreatectomies and 3 middle pancreatectomies. The
incidence of Middle Preserving Pancreatectomy was
0.6%
Both patients had almost identical presentation.
Both were young females with clinical presentation of
intermittent paroxysmal hypertension along with elevated
urine and serum catecholamine level. One of them was a
diabetic (Table 1).
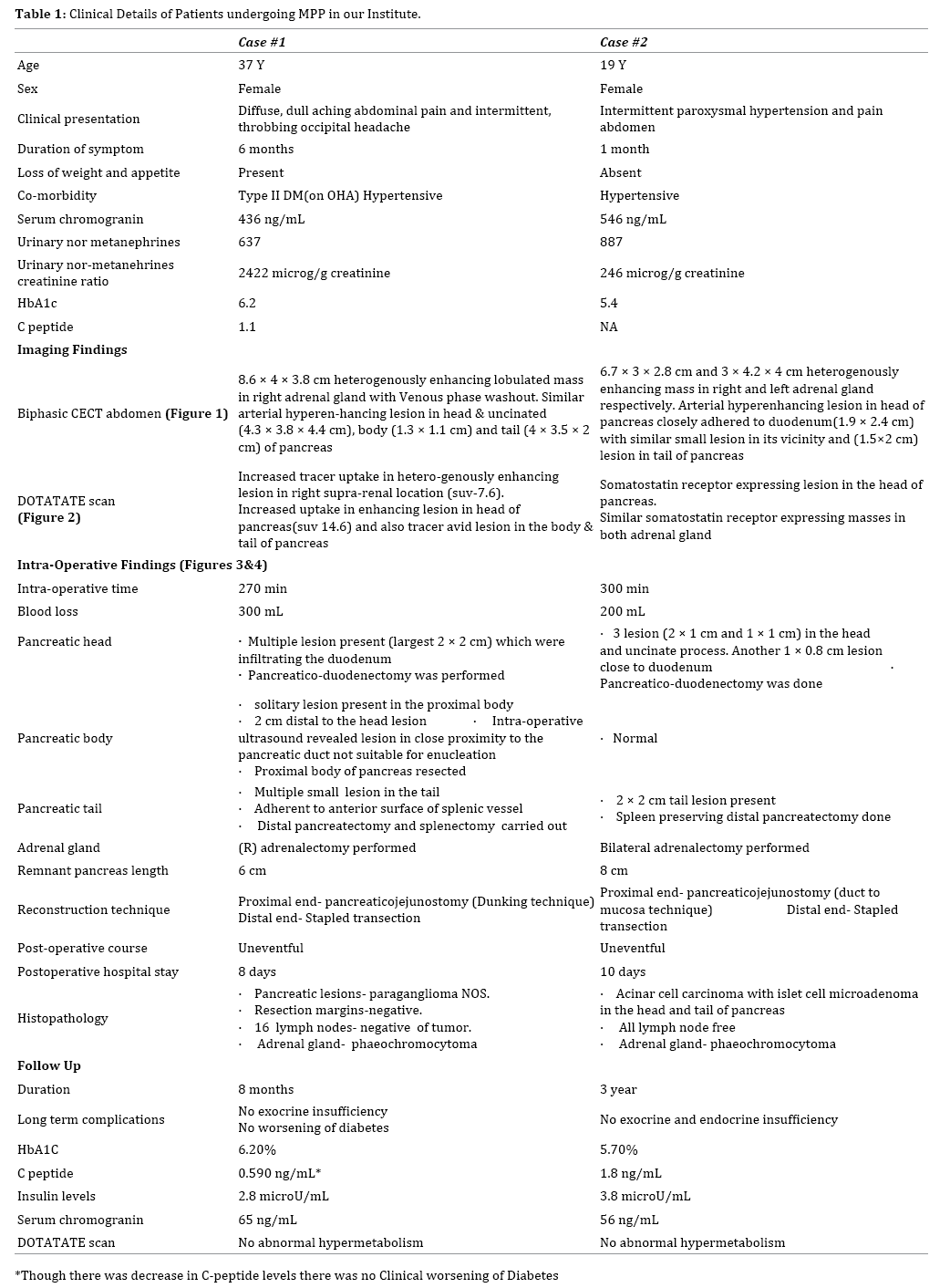
On imaging both had hyper-vascular lesion in the head
and uncinate process of pancreas and similar lesion in
the tail. One of them had similar nodule in the pancreatic
body as well. Both had adrenal lesions suggestive of
pheochromocytoma; one of the patients had bilateral
disease. Both the patients underwent Middle Preserving
Pancreatectomy and Adrenalectomy and both had an
uneventful recovery (Figures 1 and 2).
Figure 1: CECT with hyperenhancing lesion in the head and right adrenal gland (case #1)
Figure 2: DOTA scan with tracer avid lesion in the head of pancreas (case #1)
Technique of Middle Preserving Pancreatectomy
After a rooftop incision, the peritoneal cavity was
carefully explored and the pancreas was exposed. A
standard Antrum preserving pylorus ring excisionpancreaticoduodenectomy
was performed towards
the head lesion. For the distal lesion, care was taken to
preserve the dorsal pancreatic artery. A spleen-preserving
distal pancreatectomy with careful dissection of the
splenic vessels was done in one patients, while the other
one with a large lesion impinging upon the splenic hilum,
concomitant splenectomy was performed. In the patient
where splenectomy was performed, the splenic vessels
were ligated at the level of distal pancreatic transection.
Both proximal and distal resection margins were confirmed
free of malignancy on frozen section. The distal pancreatic
stump was closed using a linear stapler. Care should be
taken in leaving at least 5 cm of pancreatic remnant which
was 6 and 8cm in the two index cases. The proximal end of the pancreatic stump was anastomosed end-to-side to a
Roux en-Y jejunal loop. An end-to-side hepaticojejunostomy
and gastrojejunostomy were performed in same order
over a single jejunal loop. Figures 3 and 4 shows the end
result of the surgical procedure.
Figure 3: Intraoperative photograph of the pancreatic remnant (case #1). (a). Proximal end of pancreatic stump prepared for intestinal anastomosis. (b). Distal stapled end of pancreatic stump
Figure 4: Photograph of resected specimen (case #1)
Literature Search Strategy
A PubMed search was made using the key words
Middle preserving pancreatectomy, Center preserving
Pancreatectomy, Multicentric pancreatic lesions,
Parenchyma preserving Pancreatectomy and the resultant
articles dating between 1999 to December 2017 were
scrutinized and 16 full text articles were systematically
reviewed in the present analysis. Out of the 16 articles
reviewed, four were case series and remaining 12 were
single case reports.
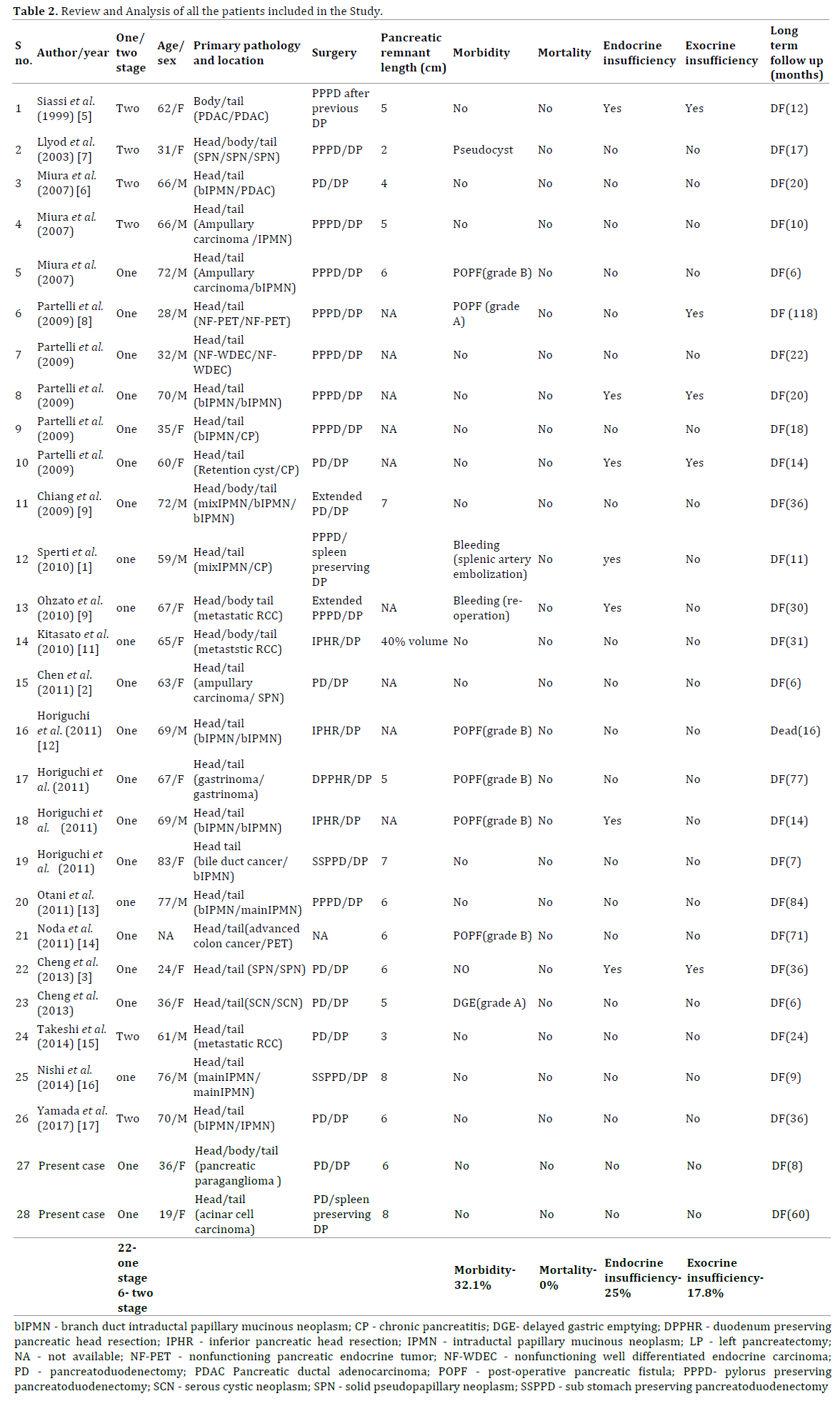
Literature Analysis
In the present study a total of 28 patients data were
retrieved and analysed (including two from present
study). For patients operated after 2007, the complications
such as pancreatic fistula, delayed gastric emptying and
post pancreatectomy haemorrhage were classified in
accordance with the ISGPS definitions [4]. The mean age
of the study group was 56.85 years (19-83 years), female
to male ratio was 1:1.07. In the present review the most
common indication for Middle Preserving Pancreatectomy was Intraductal Papillary Mucinous Neoplasm (10) and
other indications were Pancreatic Endocrine tumors (4),
Solid Pseudopaillary neoplasms (3), Metastatic Renal
Cell carcinoma (3), chronic pancreatitis (3), pancreatic
ductal adenocarcinoma (2), serous cystic neoplasm (1). 22 patients underwent one stage Middle Preserving
Pancreatectomy while the remaining six patients
underwent the surgery in two stages. The mean length of
pancreatic remnant to be 5.5 cm (2-8 cm). In the present
analysis we found the overall morbidity to be 32.1%
(9/28), Pancreatic fistula rate was 21.4% (6/28) of which
7.14% (2/28) were grade A and 14.2% (4/28) was grade
B. One patient had grade A delayed gastric emptying, while
2 patients had postoperative haemorrhage which was
managed by coil embolization of the splenic artery in one
and surgical reexploration in another. There have been
no reports of peri-operative mortality or necrosis of the
remnant pancreas till now. We found the rate of endocrine
and exocrine insufficiency to be 25% (7/28) and 17.8%
(5/28) respectively (Table 2).
DISCUSSION
Siassi et al. in 1999 first described a two staged middle
preserving pancreatectomy in a patient with metachronous
pancreatic adenocarcinoma who previously underwent
distal pancreatectomy [5]. In 2007 Miura et al. reported
first single stage Middle Preserving Pancreatectomy with
successful outcome [6]. Ever since only 26 cases have been
reported [7, 8, 9, 10, 11, 12, 13, 14, 15].
Middle preserving pancreatectomy is a rare surgical
procedure, mainly due to lack of suitable cases. Middle
preserving pancreatectomy should be avoided in patient
with pancreatic ductal adenocarcinoma due to inability
to perform proper lymphadenectomy and compromise of
resection margins [16]. Middle preserving pancreatectomy
has been considered preferable in patients with benign,
borderline or low grade malignancies with multicentricity.
MPP should be converted to an oncologically appropriate
operation if inadequate tumor resections are encountered
intraoperatively (Figure 5).
Figure 5: Medium power photomicrograph of the tumour showing cells with monomorphic nuclei with finely stipple chromatin. The cells are dominantly arranged in trabeculae and cords, occasionally with acinar pattern separated by fine fibrovascular stroma. (H&E, x400) (case #1)
Middle preserving pancreatectomy has two potential
sources of pancreatic fistula - pancreato-intestinal
anastomotic site and stapled distal end of pancreatic
remnant. So, theoretically can be considered to be at
a higher risk of pancreatic fistula and perioperative
morbidity. Perioperative morbidity and mortality
associated with pancreatoduodenectomy and distal
pancreatectomy are 38-44%, 1-4% and 13-54%, 0-4%
mrespectively [17, 18, 19, 20, 21] which is comparable
to Middle Preserving Pancreatectomy. In a recent metaanalysis,
total pancreatectomy was associated with an
overall morbidity and mortality of 31.1-57.1% and 1.6-
9.2% respectively with inevitable exocrine and endocrine
insufficiency [22].
Dorsal pancreatic artery is the major supply to the
pancreatic remnant and care should be exercised to
preserve it [16]. This can be achieved by performing careful
lymphadenectomy at the level of celiac and splenic artery.
Both the patients in the present study had an uneventful
recovery; this was probably due to the better preservation
of blood supply of pancreatic remnant.
There are no consensuses regarding the optimal length
of pancreatic remnant to prevent pancreatic insufficiency.
Clinically significant pancreatic insufficiency results
from80-90% loss of pancreatic parenchyma [23]. To
prevent pancreatic insufficiency Miura et al. proposed
preservation of at least 25% pancreatic parenchyma [6].
Yasuda et al. analyzed the volume of middle portion of
pancreas to be 25% of the gland based on CT pancreatic
volumetric [24]. Theoretically middle preserving
pancreatectomy should preserve enough pancreas
to preclude development of exocrine and endocrine
insufficiency. The length of pancreatic remnant predicted
to prevent exocrine and endocrine insufficiency has
been estimated to be at least 5-6 cm, as this length
approximates to about 35-40% of the gland. Moreover
middle preserving pancreatectomy preserves glucagon
secreting alpha cells located mainly in the body of
pancreas and reduce risk of brittle diabetes [1]. In our
analysis we found even the patient with small remnant
pancreas (2 cm) did not develop pancreatic insufficiency
at 17 months follow up.
Pancreatic pathology involving the head and tail
definitely has the potential of involving the pancreatic
body. There is a risk of residual or recurrent disease in
the remnant pancreas. In order to avoid the recurrence in the remnant pancreas after MPP, appropriate candidates
should be selected through careful preoperative evaluation
of malignant potential, and intraoperative frozen section
analysis of the two resection margins. Furthermore,
intraoperative ultrasound would be helpful to identify all
of the lesions and to confirm that the remnant was disease
free. There have been no reports of disease recurrence
in the remnant pancreas after middle preserving
pancreatectomy. However the patient should be kept on
regular follow up to detect early recurrence.
CONCLUSION
Concluding, middle preserving pancreatectomy is a
feasible, safe and effective alternative in carefully selected
patients with benign or low grade multicentric pancreatic
neoplasms. The procedure can be performed with
acceptable morbidity and no mortality with a good long
term functional outcome.
Conflicts of Interest
There are no conflicts of interest.
References
- Sperti C, Polizzi ML, Moro M, Beltrame V, Pedrazzoli S. Middle-preserving pancreatectomy: an interesting procedure for pancreas-sparing resection. JOP 2010; 11:258-61. [PMID: 20442523]
- Chen HW, Wang FJ, Lai EC, Lau WY. Middle-preserving pancreatectomy for synchronous ampullary carcinoma and solid-pseudopapillary tumor of distal pancreas. Int J Surg Case Rep 2011; 2:267-8. [PMID: 22096749]
- Cheng K, Shen BY, Peng CH, Na LM, Cheng DF. Middle-preserving pancreatectomy: report of two cases and review of the literature. World J Surg Oncol 2013; 11:106. [PMID: 23702284]
- Pratt WB, Maithel SK, Vanounou T, Huang ZS, Callery MP, Vollmer Jr CM. Clinical and economic validation of the International Study Group of Pancreatic Fistula (ISGPF) classification scheme. Ann Surg 2007; 245:443. [PMID: 17435552]
- Siassi M, Klein P, Hohenberger W. Organ-preserving surgery for multicentric carcinoma of the pancreas. Eur J Surg Oncol 1999; 25:548–550. [PMID: 10527608]
- Miura F, Takada T, Asano T, Kenmochi T, Ochiai T, Amano H, et al. Hemodynamic changes of splenogastric circulation after spleen-preserving pancreatectomy with excision of splenic artery and vein. Surgery 2005; 138:518-22. [PMID: 16213907]
- Lloyd FP Jr, Kang J. Multifocal papillary-cystic neoplasm of the pancreas. J Natl Med Assoc 2003; 95:1204– 1207. [PMID: 14717478]
- Partelli S, Boninsegna L, Salvia R, Bassi C, Pederzoli P, Falconi M. Middle-preserving pancreatectomy for multicentric body-sparing lesions of the pancreas. Am J Surg 2009; 198:e49-53. [PMID: 19716880]
- Chiang KC, Hsu JT, Chen HY, Jwo SC, Hwang TL, Jan YY, et al. Multifocalintraductal papillary mucinous neoplasm of the pancreas – a case report. World J Gastroenterol 2009; 15:628-632. [PMID: 19195068]
- Ohzato H, Yamamoto T, Fukunaga M, Imamura H, Furukawa H. Middlepreserving pancreatectomy for multifocal metastatic renal cell carcinoma located in the head, body and tail of the pancreas. A case report. JOP 2010; 11:633–637. [PMID: 21068502]
- Kitasato A, Tajima Y, Kuroki T, Tsutsumi R, Tsuneoka N, Adachi T, et al. Limited pancreatectomy for metastatic pancreatic tumors from renal cell carcinoma. Hepatogastroenterology 2010; 57:354–357. [PMID: 20583442]
- Horiguchi A, Ishihara S, Ito M, Asano Y, Furusawa K, Yamamoto T, et al. Middle-segment-preserving pancreatectomy for biliary-pancreatic tumors. Hepatogastroenterology 2011; 58:1018–1021. [PMID: 21830434]
- Otani T, Enami Y, Tanaka K, Kusano T, Maeshiro T, Umekita N, et al. Simultaneous pancreaticoduodenectomy and distal pancreatectomy for two IPMNs in the head and the tail. Pancreas 2011; 40:165–167. [PMID: 21160379]
- Noda H, Kato T, Kamiyama H, Toyama N, Konishi F. Middle-preserving pancreatectomy for advanced transverse colon cancer invading the duodenun and non-functioning endocrine tumor in the pancreatic tail. Clin J Gastroenterol 2011; 4:24-7. [PMID: 26190617]
- Takeshi A, Mitsuhiro I, Hiromitsu A, Naoyuki Y, Taiichiro S, Hiroki S, et al. Middle segment-preserving pancreatectomy for recurrent metastasis of renal cell carcinoma after pancreatoduodenectomy: a case report. Case Rep Surg 2014; 2014:648678. [PMID: 25061531]
- Nishi M, Kawasaki H, Fujii M, Nagahashi M, Obatake M, Shirai M, et al. Middle-preserving pancreatectomy for multifocal intraductal papillary mucinous neoplasms of the pancreas: report of a case. Clin J Gastroenterol 2014; 7:251-4. [PMID: 24883129]
- Yamada M, Sugiura T, Okamura Y, Ito T, Yamamoto Y, Ashida R, et al. Middle segment-preserving pancreatectomy for metachronous intraductal papillary mucinous neoplasm after pancreatoduodenectomy: a case report. Surg Case Rep 2017; 3:28. [PMID: 28197897]
- Kawai M, Kondo S, Yamaue H, Wada K, Sano K, Motoi F, et al. Predictive risk factors for clinically relevant pancreatic fistula analyzed in 1,239 patients with pancreaticoduodenectomy: multicenter data collection as a project study of pancreatic surgery by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J Hepatobiliary Pancreat Sci 2011; 18:601-8. [PMID: 21491103]
- Schmidt CM, Powell ES, Yiannoutsos CT, Howard TJ, Wiebke EA, Wiesenauer CA, et al. Pancreaticoduodenectomy: a 20-year experience in 516 patients. Arch Surg 2004; 139:718–25. [PMID: 15249403]
- Knaebel HP, Diener MK, Wente MN, Büchler MW, Seiler CM. Systematic review and meta-analysis of technique for closure of the pancreatic remnant after distal pancreatectomy. Br J Surg 2005; 92:539–46. [PMID: 15852419]
- Crippa S, Bassi C, Warshaw AL, Falconi M, Partelli S, Thayer SP, et al. Middle pancreatectomy: indications, short- and long-term operative outcomes. Ann Surg 2007; 246:69–76. [PMID: 17592293]
- Del Chiaro M, Rangelova E, Segersvärd R, Arnelo U. Are there still indications for total pancreatectomy. Updates Surg 2016; 68:257-63. [PMID: 27605208]
- Slezak LA, Andersen DK. Pancreatic resection: effects on glucose metabolism. World J Surg 2001; 25:452–460. [PMID: 11344398]
- Yasuda H, Takada T, Toyota N, Amano H, Yoshida M, Takada Y, et al. Limited pancreatectomy: significance of postoperative maintenance of pancreatic exocrine function. J Hepatobiliary Pancreat Surg 2000; 7:466–472. [PMID: 11180872]






