Ali Samba1*, Kareem Mumuni1 and Amala Chukwu Okpala2
1Department of OBGYN, University of Ghana School of Medicine and Dentistry, Ghana
2Department of OBGYN, Korle-Bu Teaching Hospital, Ghana
*Corresponding Author:
Ali Samba,
Department of OBGYN
University of Ghana School of Medicine and Dentistry
Korle-Bu. Accra, Ghana
Tel: +0023326747367
E-mail: abmasa@yahoo.com
Received date: July 19, 2016; Accepted date: January 10, 2017; Published date: January 12, 2017
Citation: Samba A, Mumuni K, Okpala AC. A Case Report of Pregnancy in Rudimentary Horn, Gynecol Obstet Case Rep. 2017, 3:1. doi:10.21767/2471-8165.1000039
Introduction
Retention of surgical sponges intra-abdominally is an uncommon surgical error and a rare but preventable occurrence [1,2]. The true incidence may never be known as the embarrassment, humiliation, job loss and law suit that could attend this situation often leads to shelving of many cases especially in the developing world [3].
The real incidence of retention of surgical sponges intraabdominally is yet to be well described. Reports have shown it to be in the range of 1 in 100 to 3000 for all surgical interventions and 1 in 1000 to 1500 for intra-abdominal operations [4].
A case of a woman in whom a surgical sponge was inadvertently left in her pelvis post abdominal hysterectomy which migrated via a vaginal vault fistula into the bladder with partial extrusion through the urethral orifice is reported here.
Case Report
A 45 year old multiparous woman presented with an eight week history of dysuria, fever, chills, frequency, nocturia, straining, feeling of incomplete emptying, urge incontinence and lower abdominal pain associated with a three day history of protrusion of a whitish substance from the urethral orifice (Figure 1).
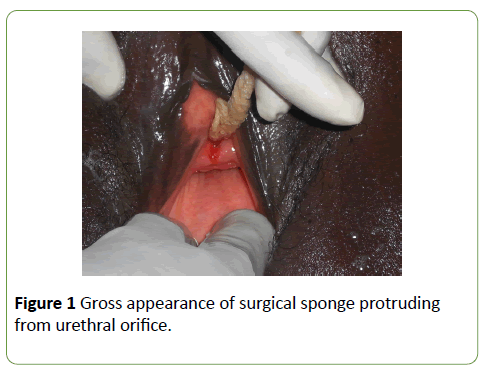
Figure 1:Gross appearance of surgical sponge protruding from urethral orifice.
A year ago she had undergone a total abdominal hysterectomy for bleeding uterine fibroids at a private clinic; and had no symptoms until eight weeks before reporting to the clinic. Previous treatments for recurrent urinary tract infections were of no avail.
A cystogram done revealed a structure which resembled a surgical sponge situated between the bladder and vagina and an urethro-vaginal fistula was suspected as contrast outlined both the vagina and gauze during initial phase of contrast administration (Figure 2).
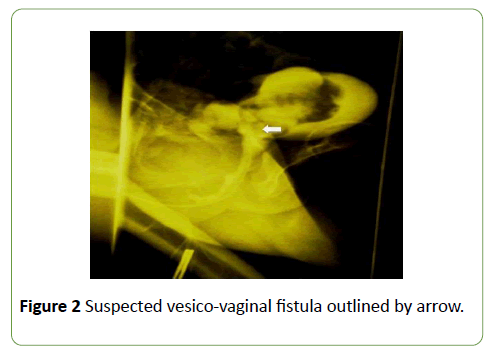
Figure 2:Suspected vesico-vaginal fistula outlined by arrow.
An exploratory laparotomy done revealed adhesions between the bladder and the small bowel, and also an abdominal sponge that had invaded into the urinary bladder. On cystostomy the sponge was noticed to have extruded partially through the external urethra meatus (Figures 3-5).
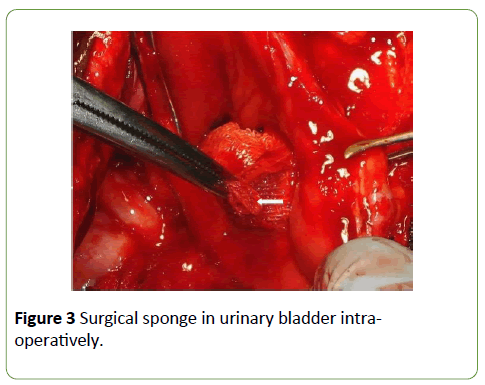
Figure 3:Surgical sponge in urinary bladder intraoperatively.
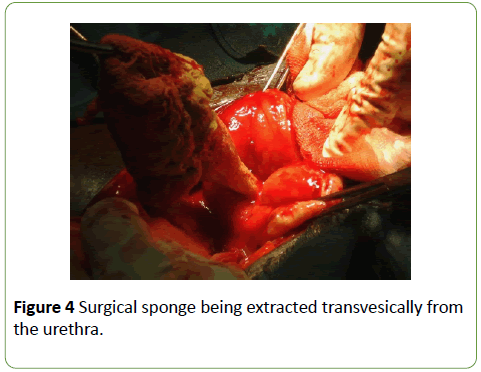
Figure 4:Surgical sponge being extracted transvesically from the urethra.

Figure 5:The surgical sponge.
The sponge was removed, and the bladder repaired with vicryl 2/0. The post-operative management included oral antibiotics and the urethral catheter retained for 21 days. She was discharged home well and continent. She was reviewed at 2 and 6 weeks and was in satisfactory condition without any voiding difficulties.
Discussion
The term “gossypiboma” denotes a cotton foreign body that is retained inside the patient during surgery [5]. The word is derived from two sources: the Latin word gossypum which means “cotton”; and boma which means “concealed place” derived from Kiswahili [3].
Retained surgical sponges have been reported to occur after a diversity of surgical procedures such as abdominal, thoracic, cardiovascular, orthopaedic, and even neurosurgical operations [2,6]. Following retention, they have revealed themselves as intra-abdominal masses, in intestinal fistulae, by intestinal obstruction after transmural migration into the intestinal lumen, by protrusion into the gastric antrum from the first part of the duodenum, and into the rectum.3 Most cases present as a mass or with subacute intestinal obstruction, although rarely do they result in fistulas, free perforation or even extrusion [7].
A review of 64 cases of transmural migration of retained surgical sponges, mainly after intra-abdominal surgery, showed that 75% of the cases involved intestinal migration, whereas only 7 cases described migration into the bladder [6]. Spontaneous transurethral protrusion is rare, and the present authors have the knowledge of the report of only one case [8].
In the case presented, there was spontaneous protrusion through the urethra.
Clinical presentations are usually acute or delayed, where acute follows a septic course with abscess/granuloma formation, and delayed occurs months to years later with adhesion formation and encapsulation [2]. The acute type occurs if the material is contaminated or causes mechanical bowel obstruction. The abscess formed ultimately ruptures into a hollow viscus and discharges pus followed by bleeding and extrusion of the foreign body. If the foreign body cannot be extruded it remains in the abscess cavity and creates multiple fistulae, leading to complaints of chronic ill health and vague abdominal symptoms post-surgery [3].
The delayed type is usually due to a sterile foreign body granuloma with no contamination. Gradually, the foreign material invades a hollow viscus and the thick walled cavity gradually collapses over the foreign material as it migrates into the lumen of the organ [3].
It is likely that the present case, perhaps, falls into the latter type, since the total abdominal hysterectomy was done a year before. As described by Lin et al, a possible explanation for the present case could be that a gossypiboma formed as a result of chronic inflammation around the retained surgical sponge, which eroded through the posterior wall of the urinary bladder and manifested with urinary symptoms including repeated episodes of urinary tract infections [8]. It is proposed that repeated contractions of the bladder muscle in an attempt to expel the foreign body caused the gossypiboma to extrude through the only exit, the internal urethral meatus and then finally protrude from the external urethral meatus.
Common risk factors associated with retained foreign bodies post operatively include unplanned changes of operative procedures, in emergency surgical interventions, when instrument/sponge counts are omitted and when operating on obese patients with excessive amounts of fat [2,3]. The risk increases in patients who may have had a greater number of major surgical procedures at the same time and also when there have been multiple surgical teams [3]. Although surgical textile materials and instruments should be counted once at the start and twice at the end of surgery, counts are not always sufficient, since most reported cases occur in spite of a normal pack count [9]. A case has been reported of a retained laparotomy sponge 11 months post hysterectomy despite the sponge count having been performed twice according to the operative record [10].
Preoperative diagnoses of gossypiboma can be made in many cases utilizing various radiological modalities such as plain radiography when surgical textile materials have been impregnated with a radio-opaque marker, ultrasonography, computerized tomography, magnetic resonance imaging, and gastrointestinal contrast series [2]. In the case of intravesical foreign bodies, radio-opaque ones can usually be detected on Kidney, Ureter and Bladder (KUB) radiography while ultrasonography has been reported for the detection of nonradio- opaque intravesical foreign bodies [11]. Also, urological contrast studies (intravenous urography, retrograde urethrography) may provide additional information and occasionally reveal surprising findings and unexpected radiolucent objects [12]. In the present case, a cystogram was used to confirm the diagnosis.
Once a gossypiboma is diagnosed, it should be removed. Surgery has been the mainstay in the removal of the foreign bodies for many years [2]. Although some non- surgical approaches such as percutaneous radiological retrieval of foreign bodies are reported, they might either be unsuccessful or generate attendant complications [13].
Suggestions put forward to prevent retention of surgical sponges as well as facilitate early postoperative detection include use of sponges with counting of surgical materials once at the beginning and twice at the end of the surgery, methodical wound/body cavity examination and use of sponges with radiopaque markers, and the routine radiographic screening of high-risk patients before they leave the operating room even when counts are documented as correct [2,4,6]. The most important consideration is for the surgeon to keep in mind that despite correct sponge counts gossypibomas do occur and it is responsibility to prevent.
References
- Hung-Shun S, Sung-Lang C, Chia-Cheng K, Shao-Chuan W, Yu-Lin K (2007) Gossypiboma-retained surgical sponge. Journal of Chinese Medical Association 70: 511-513.
- El Fortia M, Bendaoud M, Sethi S (2008) Abdominal Gossypiboma (Textilioma). The Internet Journal of Radiology 9.
- Dakubo J, Clegg-Lamptey JN, Hodasi WM, Obaka HE, Toboh H, et al. (2009) An intra-abdominal gossypiboma. Ghana Med J43: 43-45.
- Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ (2003) Risk factors for retained instruments and sponges after surgery. N Engl J Med 348:229-235.
- Rajagopal A, Martin J (2002) Gossypiboma-"a surgeon's legacy": Report of a case and review of the literature. Dis Colon Rectum 45:119-120.
- Zantvoord Y, van der Weiden RM, van Hooff MH (2008) Transmural migration of retained surgical sponges: a systematic review. Obstet Gynecol Surv 63:465-71.
- Moyle H, Hines OJ, McFadden DW (1996) Gossypiboma of the abdomen. Arch Surg 131: 566-568.
- Lin TY, Chuang CK, Wong YC, Liao HC (1999) Gossypiboma: Migration of retained surgical gauze and spontaneous transurethral protrusion. BJU Int 84: 879-880.
- Zbar AP, Agrawal A, Saeedi IT, Utidjian MRA (1998) Gossypiboma revisited: A case report and review of the literature. J R Coll Surg Edinb43:417-418.
- Dhillon JS, Park A (2002)Transmural migration of a retained laparotomy sponge. Am Surg68:603-605.
- Rafique M (2008) Intravesical foreign bodies; review and current management strategies. Urol J5: 223-231.
- Eckford SD, Persad RA, Brewster SF, Gingell JC (1992)Intravesical foreign bodies: Fiveyear review. Br J Urol 69:41-45.
- Nosher JL, Siegel R (1993) Percutaneous retrieval of nonvascular foreign bodies. Radiology 187:649-651.

