Vishal Gupta, Sunil Kumar, Pankaj Kumar, Abhijit Chandra*
Department of Surgical Gastroenterology, Chhatrapati Shahuji Maharaj Medical University. Chowk, Lucknow, Uttar Pradesh. India
- *Corresponding Author:
- Abhijit Chandra
Department of Surgical Gastroenterology
Chhatrapati Shahuji Maharaj Medical University
Erstwhile King George Medical University
Lucknow, Uttar Pradesh; India
Phone: +91-522.225.8660/+91-522.274.0068
Mobile: +91-933.592.0302
Fax: +91-522.225.6116
E-mail: abhijitchandra@hotmail.com
Received December 15th, 2010 Accepted February 1st, 2011
Keywords
Pancreatitis, Chronic; Splenectomy; Aneurysm, False
INTRODUCTION
Visceral artery aneurysms are uncommon and pseudoaneurysms are rare entities. The splenic artery is the most commonly affected artery [1]. Goldberg et al. [2] found only 160 cases of splenic artery pseudoaneurysm in the literature which were reported in the last 43 years. The Mayo clinic experience revealed only 10 cases over a period of 18 years [1]. Giant pseudoaneurysms, defined as pseudoaneurysms equal to, or greater than, 5 cm in size, are rare. Only 19 cases have been reported until now. We herein describe the case of a giant pseudoaneurysm of the splenic artery in a patient who presented with abdominal pain without bleeding.
CASE REPORT
A 47-year-old male patient presented to our out-patient department with a 1-month history of non-radiating epigastric abdominal pain, moderate to severe in intensity occasionally requiring injectable analgesics. There was a history of occasional vomiting. He had been an alcoholic for the past 15 years. Diabetes had been detected 6 months previously and was controlled with an oral hypoglycemic. There was no history of hematemesis, melena, fever, jaundice, altered bowel habits, anorexia or weight loss. He had undergone an open cholecystectomy 3 years previously for symptomatic gallstones. Physical examination was non-contributory. The patient was initially evaluated elsewhere with abdominal ultrasound which revealed a multilayered lesion with a peripheral anechoic area contiguous with the splenic artery and another cystic lesion (5.5x4 cm) close to the anterior abdominal wall. The patient was admitted to our center and underwent further evaluation.
A hematological work-up, including hemoglobin and liver function tests, was normal. A contrast enhanced computed tomography scan (Figures 1 and 2) revealed features of chronic pancreatitis with multiple foci of calcifications in the pancreatic duct and parenchyma involving the body and tail. The pancreatic duct was not significantly dilated. There was a large pseudoaneurysm measuring 7x4 cm in size in the splenic artery. In addition, there was a pseudocyst measuring 6x4 cm in size in the omentum, separate from the pancreas.
Figure 1. CT scan showing calcification in the body and tail of the
pancreas, pseudoaneurysm and pseudocyst separate from the
pancreas.
Figure 2. CT scan coronal reconstruction showing a giant
pseudoaneurysm of the splenic artery with the artery passing through
the pseudoaneurysm.
The patient underwent an exploratory laparotomy. The pancreas was firm and there was a large pulsating pseudocyst in the body of the pancreas having a thin wall at places where an intraluminal clot could be seen (Figure 3). It was densely adherent to the stomach and the retroperitoneum. Another pseudocyst was also located in the greater omentum separate from the pancreas. The lesser sac was entered by dividing the gastrocolic omentum and the short gastric vessels. The stomach was separated from the pseudoaneurysm and the pancreas by careful dissection. Proximal vascular control of the splenic artery was achieved near its origin. A distal pancreatectomy and splenectomy were then performed in an antegrade manner (Figure 4). The omental pancreatic pseudocyst was also resected. The postoperative period was uneventful and the patient was discharged on the 7th postoperative day.
Figure 3. Intraoperative photograph showing the pseudoaneurysm
with a thin wall. The pancreas has been looped near the neck region.
Figure 4. Resected specimen of a distal pancreatectomy and
splenectomy showing clots inside the pseudoaneurysm.
DISCUSSION
Visceral artery pseudoaneurysms are uncommon. The splenic artery is the most commonly affected visceral artery [1]. They usually develop secondary to pancreatic diseases. They develop more commonly in chronic pancreatitis (46%) than in acute pancreatitis (6%) [1]. Our patient developed a splenic artery pseudoaneurysm secondary to chronic pancreatitis. The mechanisms of the formation of pseudoaneurysms in pancreatitis include inflammation with enzymatic digestion of the pancreatic or peripancreatic artery, visceral artery erosion by pseudocysts and pseudocyst erosion into the bowel wall and intramural artery [3]. Abdominal trauma is the second most common cause. Damage to the intima and elastic lamina due to rapid deceleration may lead to the formation of such a pseudoaneurysm [4]. Other causes described are peptic ulcer disease and iatrogenic causes (e.g. prior abdominal surgery or endovascular interventions) [1, 2].
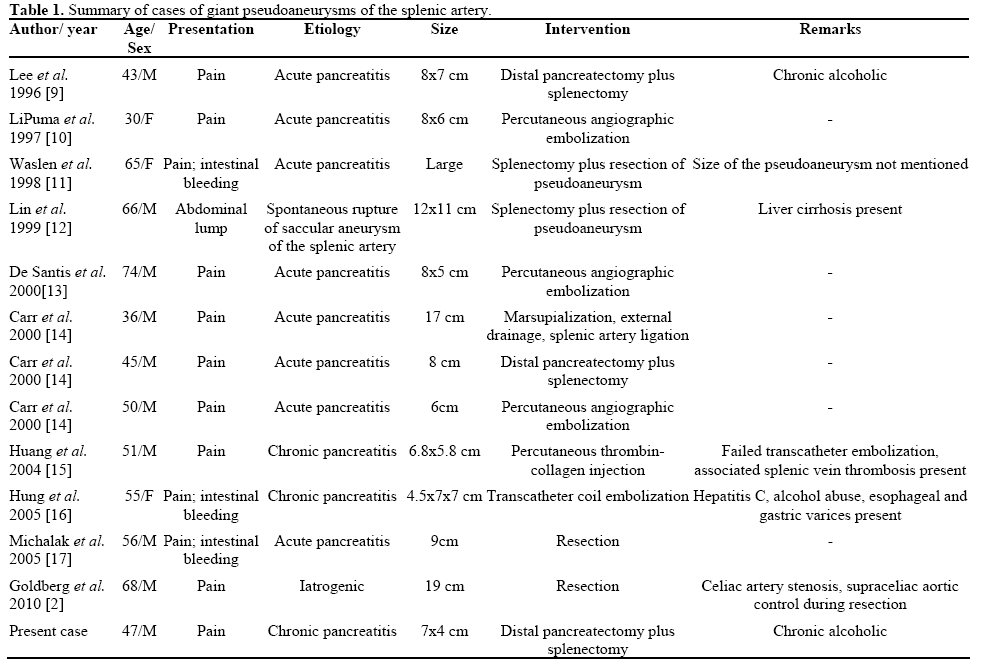
Most of theses pseudoaneurysms are symptomatic at presentation; however, 2.5% of cases have been incidental [1]. They most commonly present with abdominal pain (as in our case) or with bleeding into the gut which may be catastrophic at times. Large or giant pseudoaneurysms may also present with an abdominal lump (Table 1).
Diagnosis is usually made from computed tomography (including CT angiography) or transcatheter angiography. They can also be detected on color Doppler or MR angiography. Transcatheter angiography is considered the gold standard and also has therapeutic potential.
A giant pseudoaneurysm is defined as a pseudoaneurysm equal to, or greater than, 5 cm in size. In the literature, size has ranged from 5-18 cm [1, 2]. Only 19 cases of giant pseudoaneurysms have been reported. Most of these (n=15) have been seen in association with pancreatic diseases [1] (Table 1). Erosion of the splenic artery by an enlarging pseudocyst due to enzymatic digestion and, thus, conversion of the pseudocyst into a pseudoaneurysm can explain the formation of a giant pseudoaneurysm. The remaining 4 cases were secondary to iatrogenic causes: e.g., splenectomy in 2 cases, cystogastrostomy in one and a prior attempt at repairing a splenic artery aneurysm in the last reported case [2].
All splenic artery pseudoaneurysms should be treated when detected as size is not a determinant of future rupture. This is more relevant in patients with chronic pancreatitis as it is an ongoing inflammatory process. A review of the literature suggests that these giant pseudoaneurysms have been managed by both surgical and non-surgical means (Table 1). Different methods of treatment have been trans-angiographic embolization (n=8), distal pancreatectomy/splenectomy (n=7), thrombin injection (n=2), pancreatectomy (n=1) and resection of pseudoaneurysm only (n=1) [2]. However, a pseudoaneurysm associated with a pseudocyst should be treated surgically as the literature indicated that transcatheter embolization has a higher failure rate (20%) as a primary treatment in these patients than in those without pseudocysts (13%) [1]. Hsu et al. [3] have also reported a high (66.7%) rebleeding rate after angiographic embolization. There are recent reports of successful treatment by endovascular stent graft occlusion of these pseudoaneurysms [5]. A pseudoaneurysm related to pseudocyst formation is best treated with surgical excision [1, 6, 7, 8]. Different surgical options exist including splenectomy with or without distal pancreatectomy, ligation of the splenic artery with resection of the pseudoaneurysm and trans-cystic ligation of the bleeding vessel with internal or external drainage of the pseudocyst. Splenectomy, with or without distal pancreatectomy, is a procedure with no reported failure over long periods of time [1]. Distal pancreatectomy and splenectomy should be employed to treat bleeding pseudoaneurysms located in the distal body and tail of the pancreas. Pancreatic resection is the only way to treat these pseudoaneurysms together with the underlying pathologic process in the pancreas which is the primary cause of the pseudoaneurysm. This may be curative in cases where chronic pancreatitis changes are confined to the body and tail of the pancreas, as in our case. However, surgical treatment may not be straightforward especially, in cases of giant pseudoaneurysm.
Conflicts of interest
The authors have no potential conflicts of interest
References
- Tessier DJ, Stone WM, Fowl RJ, Abbas MA, Andrews JC, Bower TC, Gloviczki P. Clinical features and management of splenic artery pseudoaneurysm: case series and cumulative review of literature. J Vasc Surg 2003; 38:969-74. [PMID 14603202]
- Goldberg RF, Maley W, Kennedy EP, Yeo CJ, Lavu H. Giant Splenic Artery Pseudoaneurysm. J Gastrointest Surg 2010; Nov 25. [PMID 21108018]
- Hsu JT, Yeh CN, Hung CF, Chen HM, Hwang TL, Jan YY, Chen MF. Management and outcome of bleeding pseudoaneurysm associated with chronic pancreatitis. BMC Gastroenterol 2006; 6:3. [PMID 16405731]
- Norotsky MC, Rogers FB, Shackford SR. Delayed presentation of splenic artery pseudoaneurysms following blunt abdominal trauma: case reports. J Trauma 1995 ;38:444-7. [PMID 7897735]
- Brountzos EN, Vagenas K, Apostolopoulou SC, Panagiotou I, Lymberopoulou D, Kelekis DA. Pancreatitis-associated splenic artery pseudoaneurysm: endovascular treatment with self-expandable stent-grafts. Cardiovasc Intervent Radiol 2003; 26:88-91. [PMID 12491019]
- Bresler L, Boissel P, Grosdidier J. Major hemorrhage from pseudocysts and pseudoaneurysms caused by chronic pancreatitis: surgical therapy. World J Surg 1991; 15:649-52; discussion 652-3. [PMID 1949866]
- de Perrot M, Berney T, Buhler L, Delgadillo X, Mentha G, Morel P. Management of bleeding pseudoaneurysms in patients with pancreatitis. Br J Surg 1999; 86:29-32. [PMID 10027355]
- Reber PU, Patel AG, Baer HU, Triller J, Buchler MW. Acute hemorrhage in chronic pancreatitis: diagnosis and treatment options including superselective\ microcoil embolization. Pancreas 1999; 18:399-402. [PMID 10231846]
- Lee HS, Park JJ, Kim CD, Ryu HS, Hyun JH. Pseudoaneurysm and splenic infarction in chronic pancreatitis--a case report. J Korean Med Sci 1996; 11:183-7. [PMID 8835768]
- LiPuma JP, Sachs PB, Sands MJ, Stuhlmiller S, Herbener TE. Angiography/interventional case of the day. Splenic artery pseudoaneurysm associated with pancreatitis. AJR Am J Roentgenol 1997; 169:259, 262-3. [PMID 9207539]
- Waslen T, Wallace K, Burbridge B, Kwauk S. Pseudoaneurysm secondary to pancreatitis presenting as GI bleeding. Abdom Imaging 1998; 23:318-21. [PMID 9569306]
- Lin CT, Chiang CW, Hsieh HC. Extrasplenic pseudoaneurysm. The role of color flow Doppler ultrasound in diagnosis. Jpn Heart J 1999; 40:365-8. [PMID 10506858]
- De Santis M, Ariosi P, Ferretti A, Casolo A, Manenti A, Romagnoli R. Embolization of giant aneurysm and pseudoaneurysm of the splenic artery. Eur Radiol 2000; 10:1032. [PMID 10879726]
- Carr JA, Cho JS, Shepard AD, Nypaver TJ, Reddy DJ. Visceral pseudoaneurysms due to pancreatic pseudocysts: rare but lethal complications of pancreatitis. J Vasc Surg 2000; 32:722-30. [PMID 11013036]
- Huang IH, Zuckerman DA, Matthews JB. Occlusion of a giant splenic artery pseudoaneurysm with percutaneous thrombin-collagen injection. J Vasc Surg 2004; 40:574-7. [PMID 15337894]
- Hung RK, Loh C, Goldstein L. Selective use of electrolytic detachable and fibered coils to embolize a wide-neck giant splenic artery pseudoaneurysm. J Vasc Surg 2005; 41:889-92. [PMID 15886676]
- Michalak M, Huba M, Kirrga M, Slyk P. Giant splenic artery pseudoaneurysm. Pol J Radiol 2005;70:99-102.





