Takatomo Mine*
Department of Orthopaedic Surgery, National Hospital Organization Kanmon Medical Center, Japan
Masaya Kajino
Department of Rehabilitation, National Hospital Organization Kanmon Medical Center, Yamaguchi, Japan
Jun Sato
Department of Rehabilitation, National Hospital Organization Kanmon Medical Center, Yamaguchi, Japan
Yasunari Ikedo
Department of Rehabilitation, National Hospital Organization Kanmon Medical Center, Yamaguchi, Japan
Koichiro Ihara
Department of Orthopaedic Surgery, National Hospital Organization Kanmon Medical Center, Japan
Hiroyuki Kawamura
Department of Orthopaedic Surgery, National Hospital Organization Kanmon Medical Center, Japan
Ryutaro Kuriyama
Department of Orthopaedic Surgery, National Hospital Organization Kanmon Medical Center, Japan
Ryo Date
Department of Orthopaedic Surgery, National Hospital Organization Kanmon Medical Center, Japan
Corresponding Author:
Takatomo Mine
Department of Orthopaedic Surgery
National Hospital Organization Kanmon Medicine Center
1-1 ChoufuUsiroda Simonoseki , Yamaguchi 752-8510, Japan
Tel: +81-83-2411199
Fax: +81-83-2411301
E-mail: minet@ kanmon-mc2.hosp.go.jp
Submitted date: August 28, 2017; Accepted date: September 14, 2017; Published date: September 21, 2017
Keywords
Gait analysis; Total knee arthroplasty; Osteoarthritis of the knee
Abbreviations
TKA: Total Knee Arthroplasty; OA: Osteoarthritis; HSS: Hospital for Special Surgery
Introduction
There are many reports that successful clinical outcomes have been achieved for patients with knee osteoarthritis (OA) after total knee arthroplasty (TKA). Gait presents good improvement after TKA. However, it has been reported that some kinematic and kinetic abnormalities persist even after a long period [1-5]. Benedetti reported that knee kinematic and kinetic abnormalities during load acceptance after total knee replacement are associated with co-contractions in muscular activation pattern [6,7]. Andriacchi reported a gait pattern, which tended to extend the knee throughout the stance phase thus avoiding the quadriceps demand [8]. Banks reported many knees showed significantly different kinematics between the gait and stair activities, as well as differences from knee having other implant designs [9]. We reported in vivo kinematics during stair stepping motion as well as standing and sitting motion from a chair after TKA. The knee motion kinematic patterns observed in this study were not similar with normal knee kinematics and were derived from the unique design of the implant [10,11]. In some patients, their gait is stable on the ground, but the feeling of instability when stair stepping remains. It is inferred that the feeling of instability when stair stepping does not completely disappear with only improvement of knee function. Improvement of gait oscillation, including the trunk, is necessary. Among daily activities, gait and stair stepping are very important. The goal of this analysis was to assess gait oscillation during gait and stair stepping in patients after TKA.
Materials and Methods
Fifteen patients who underwent TKA with the Bi-surface KU5 knee prosthesis (Kyocera Medical Corporation, Japan) were assessed in this study. All of the patients were followed-up for more than one year before being assessed. There were 12 female and 3 male patients, all of whom had been diagnosed with osteoarthritis. Their average age was 76 (range: 63-87) years (Table 1). One surgeon performed all of the TKA procedures and the parapatellar approach was used in all patients. The patella was not resurfaced. All of the implants were fixed with cement.
| Mean age |
76.1 ± 7.1 |
| Gender (male/female) |
3/12 |
| Mean body mass index |
24 ± 6.0 |
| Diagnosis (OA) |
15 |
| HSS score |
94.1 ± 3.3 |
| Mean follow-up (months) |
40.7 ± 9.5 |
Table 1: Patient characteristics.
The postoperative gait analyses were performed at 40.7 (range: 27-63) months after the surgery. Clinical evaluations were made according to the knee-rating scale of the Hospital for Special Surgery (HSS) before and after arthroplasties. Statistical analysis was performed using R2.8.1. Postoperative gait analysis results between Bi-surface KU5 knee prosthesis were compared with the one factor repeated measures analysis of variance. The multiple comparison procedure used the Shaffer method.
Using a 2-point gait oscillometer MVP-WS2-S (Microstone Corp. Japan), we assessed gait oscillation during gait (10 m) and stair stepping. Two compact wireless sensors were attached to the dorsal vertebral region and the sacral region with the specified harness and belt (Figure 1).
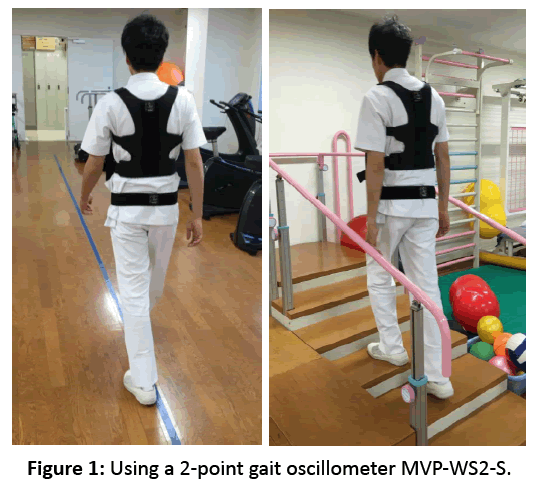
Figure 1: Using a 2-point gait oscillometer MVP-WS2-S.
The gait oscillation analyses were performed by examining acceleration (anterior, TKA side and contralateral side) and gait barycentric factors (single-support phase and ratio of the center of gravity maximum values) between gait and stair stepping. We performed the analysis postoperatively at more than one year after TKA.
For the ratio of the center of gravity maximum values, the barycentric transfer while gait was indicated on the plotted area of the figure eight in the graph. In the graph of this figure, the ratio of the center of gravity maximum values was defined as the maximum of the vertical axis/the maximum of the cross axis, and the index of the barycentric transfer at while gait (Figure 2).
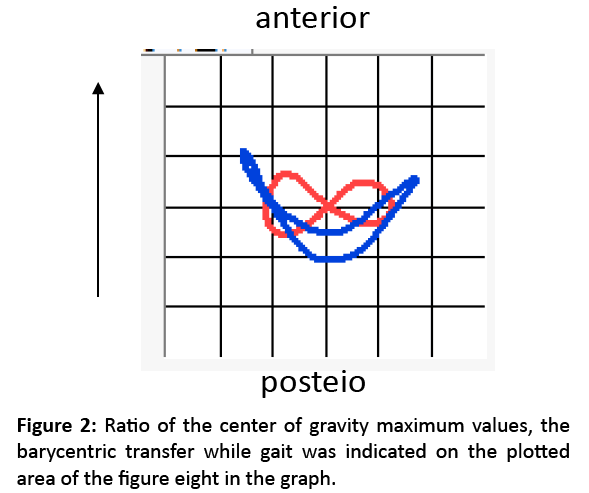
Figure 2: Ratio of the center of gravity maximum values, the barycentric transfer while gait was indicated on the plotted area of the figure eight in the graph.
Results
The mean preoperative clinical score (HSS) was 54.5, whereas the mean postoperative score improved to 94.1 after surgery.
Acceleration
To the anterior direction: Mean postoperative values were 6.45 ± 2.9 at gait, 8.32 ± 2.94 at stair-up and 5.94 ± 2.92 at stair-down in the sacral region. There was a significant difference between gait and stair-up and between stair-up and down. Mean postoperative values were 6.13 ± 1.1 at gait, 7.23 ± 1.93 at stair-up and 6.0 ± 2.44 at stair-down in the dorsal vertebral region. There was a significant difference between gait and stair-up, and between stair-up and down.
To the TKA side direction: Mean postoperative values were 4.85 ± 1.52 at gait, 3.98 ± 1.47 at stair-up and 5.86 ± 2.78 at stair-down in the sacral region. There was no significant difference between gait and stair-up or down. Mean postoperative values were 3.74 ± 1.37 at gait, 2.66 ± 0.77 at stair-up and 4.62 ± 1.99 at stair-down in the dorsal vertebral region. There was a significant difference between gait and stair-up, and between stair-up and down.
To the contralateral side direction: Mean postoperative values were 4.92 ± 1.98 at gait, 3.96 ± 1.59 at stair-up and 6.14 ± 2.09 at stair-down in the sacral region. There was a significant difference between stair-up and down. Mean postoperative values were 3.55 ± 0.89 at gait, 2.95 ± 0.76 at stair-up and 3.95 ± 1.23 at stair-down in the dorsal vertebral region. There was a significant difference between gait and stair-up, and between stair-up and down.
In the sacral region and the dorsal vertebral region, there was no significant difference between acceleration to the TKA side direction or to the contralateral direction at gait and stair-up or down.
Single-support phase
The postoperative mean value was 1.02 ± 0.15 at gait, 0.99 ± 0.07 at stair-up and 1.04 ± 0.12 at stair-down. There was a significant difference between the gait and stair-stepping values.
Ratio of the center of gravity maximum values
Postoperative values were 0.8 ± 0.44 at gait, 0.85 ± 0.46 at stair-up and 0.79 ± 0.31 at stair-down in the sacral region. Postoperative values were 0.66 ± 0.5 at gait, 0.67 ± 0.25 at stairup and 0.56 ± 0.29 at stair-down in the dorsal vertebral region. There was a significant difference between the sacral region and the dorsal vertebral region at gait and stair-up and down. There was no significant difference between the gait and stair-stepping values (Table 2).
| |
gait |
Step-up |
Step-down |
|
| Acceleration |
|
|
|
|
| To the anterior |
|
|
|
|
| Sacral region |
6.451 ± 2.90 |
8.321 ± 2.94 |
5.943 ± 2.92 |
Gaitdown** |
| Dorsal vertebral region |
6.129 ± 1.10 |
7.225 ± 1.93 |
6.007 ± 2.44 |
Gaitdown** |
| To the TKA direction |
|
|
|
|
| Sacral region |
4.849 ± 1.52 |
3.983 ± 1.47 |
5.859 ± 2.78 |
|
| Dorsal vertebral region |
3.743 ± 1.37 |
2.663 ± 0.77 |
4.628 ± 1.99 |
Gait>up ** up |
| To the contralateral direction |
|
|
|
|
| Sacral region |
4.916 ± 1.98 |
3.963 ± 1.59 |
6.141 ± 2.09 |
up |
| Dorsal vertebral region |
3.547 ± 0.89 |
2.953 ± 0.76 |
3.952 ± 1.23 |
Gait>up* up |
| Single-support phase |
|
|
|
|
| TKA side |
0.538 ± 0.07 |
0.659 ± 0.11 |
0.747 ± 0.17 |
Gait |
| Contralateral side |
0.534 ± 0.08 |
0.665 ± 0.10 |
0.716 ± 0.14 |
Gait |
| Ratio of the center of gravity maximum values |
|
|
|
|
| Sacral region |
0.806 ± 0.44 |
0.85 ± 0.46 |
0.791 ± 0.31 |
|
| Dorsal vertebral region |
0.658 ± 0.50 |
0.669 ± 0.25 |
0.56 ± 0.29 |
|
* p<0.05 ** p<0.01
Table 2: Ratio of the center of gravity maximum values.
Discussion
Gait presents good improvement after TKA. Gait analysis has long been used to assess the postoperative functional capacity following TKA. Some methods of gait analysis have been used. There have been few quantitative studies of gait analysis. Bolanos and Kramers-de Quervain reported that gait condition improves after TKA [12,13]. However, others have reported that gait impairment remains after TKA [6,14]. Berman reported that patients with a nearly balanced quadriceps-tohamstring ratio walked with a more symmetrical gait pattern, and a balanced hamstring to quadriceps mechanism is needed for resumption of normal gait [15]. Benedetti reported that knee kinematic and kinetic abnormalities during load acceptance after total knee replacement are associated with co-contractions in the muscular activation pattern [6,7]. In some patients, gait is stable on the ground, but the feeling of instability during stair-stepping remains. It is inferred that the feeling of instability during stair stepping does not completely disappear with only improvement of knee function. Assessing only knee and lower limb function is not a sufficient assessment of gait. Assessment of gait oscillation, including function of the trunk, is necessary. We used a 2-point gait oscillometer MVP-WS2-S to assess gait oscillation. This device can display visualization of the body movement while walking. The use of two wireless motion sensors allows for simple trace measurements of the motion of the dorsal vertebra and sacral regions while gait, and synchronizes the motion of two points. Among daily activities, gait and stair stepping are very important. In the present study, we examined acceleration (anterior, TKA side and contralateral side), and gait barycentric factors (single-support phase and the ratio of the center of gravity maximum values) during walking (10 m) and stair stepping.
We reviewed cases of OA that received only unilateral TKA, and examined their gait oscillation during gait and stair stepping after the unilateral TKA. Generally, acceleration to the anterior direction in the sacral region and the dorsal vertebral region increased more at stair-up than at gait or stair-down. There was no significant difference between acceleration to the TKA side direction and to the contralateral direction at gait or stair-up or down. However, acceleration to lateral side direction in the dorsal vertebral region increased to the TKA side more at stair-down than at gait or stair-up. On the other hand, acceleration to the lateral side direction in the sacral region increased to the contralateral side more at stair-down than at gait or stair-up. We considered that gait oscillation in the sacral region could be modified by the dorsal vertebral region. The single-support phase was close to 1. In comparison with the contralateral side, the load is equal on the TKA side during walking and stair stepping. This is more obvious during stair stepping than walking. The ratio of the center of gravity maximum values increased more at the sacral region than at the dorsal vertebral region. We considered gait oscillation to be less at the dorsal vertebral region than at the sacral region.
There were some limitations in our study. The small number of patients weakens the statistical power of the results. Further investigation with a larger sample size is needed to obtain more clinical data. In addition, no control group and standard error of measurement may have decreased the generalization power of this study. Despite all these limitations, the present study contributes significantly to the improvement of knee prosthesis design.
Conclusion
Increasing gait oscillation in the sacral region may be modified by the dorsal vertebral region. In comparison with the contralateral side, the load is equal on the TKA side during walking and stair stepping. This is more obvious during stair stepping than walking. Gait oscillation was less at the dorsal vertebral region than at the sacral region. Improvement of gait oscillation, including the trunk, is necessary.
Ethics Approval and Consent to Participate
This study was approved by Ethical Review Boards of Kanmon Medical Center (Shimonoseki, Japan). Informed consent to participate in our study was obtained from participants.
Funding
This research was supported by the commissioned research expenses to Kanmon Medical Center (Shimonoseki, Japan) from Kyocera Medical Japan.
Availability of Data and Materials
The authors are unable to share raw data because ethical approval was not obtained for data sharing. In addition, informed consent for data sharing was not obtained from the individuals. Please find all summarized datasets reported in the results section and the tables.
Consent for Publication
We have obtained consent to publish from the participants.
Author’s Contributions
TM designed the study, analyzed the data, and wrote the manuscript. MK, JS, YI, KI, HK, RK and RD collected the data and participated in the design of the study. MK, JS and YI analyzed the data and helped write. All authors have read and approved the final manuscript.
References
- Stiehl JB, Dennis DA, Komistek RD. In vivo determination of condylar lift-off and screw-home in a mobile bearing total knee arthroplasty. J Arthroplasty 1999; 14: 293-299.
- Uvehammer J, Karrholm J, Brandsson S. In vivo kinematics of total knee arthroplasty: Flat compared with concave tibial joint surface. J Orthop Res 2000; 18: 856-864.
- Banks SA, Markovich GD, Hodge WA. In vivo kinematics of cruciate-retaining and substituting knee arthroplasties. J Arthroplasty 1997; 12: 297-304.
- Karrholm J, Jonsson H, Nilsson KG. Kinematics of successful knee prostheses during weight-bearing: Three-dimensional movements and positions of screw axes in the Tricon-M and Miller-Ga lante designs. Knee Surg Sports Traumatol Arthrosc 1994; 2: 50-59.
- Banks SA, Hodge WA. Implant design affects knee arthroplasty kinematic during stair-stepping. Clin Orthop Relat Res 2004; 426: 187-193.
- Benedetti MG, Bonato P. Myoelectric activation pattern during gait in total knee replacement; Relationship with kinematics, kinetics and clinical outcome. IEEE Trans Rehabil Eng1999; 7: 140-149.
- Benedetti MG, Catani F, Bilotta TW, Marcacci M, Mariani E, et al. Myoelectric activation pattern and gait biomechanics after total knee replacement. Clin Biomech 2003; 18: 871-876.
- Andriacchi TP. Functional analysis of pre and post knee surgery, total knee arthroplasty and ACL reconstruction. J. Biomech 1993; 115: 575-581.
- Banks SA, Hodge A. Design and activity dependence of kinematics in flexed and mobile-bearing knee arthroplasties. J Arthroplasty 2004; 19: 809-816.
- Mine T, Hoshi K, Gamada K, Ihara K, Kawamura K, et al. Kinematic analysis of posterior-stabilized total knee arthroplasty during standing up from and sitting down on a chair. J Orthopaedic Surgery and Research 2016; 11: 142.
- Mine T, Hoshi K, Gamada K, Ihara K, Kawamura K, et al. In vivo kinematics of a unique posterior-stabilized knee implant during a stepping exercise. J Orthopaedic Surgery and Research 2016; 11: 18.
- Bolanos AA. A comparison of isokinetic strength testing and gait analysis in patients with posterior cruciate-retaining and substituting knee arthroplasties. J Arthroplasty 1998; 13: 906-915.
- Kramers-de Quervain IA. Quantitative gait analysis after bilateral total knee arthroplasty with two different systems within each subject. J Arthroplasty 1997; 12: 168-179.
- Hilding MB. Gait affects tibial component fixation. J Arthroplasty 1999; 14: 589-593.
- Berman AT, Bosacco SJ. Evaluation of total knee arthroplasty using isokinetic testing. Clin Orthop 1991; 271: 106-113.

