Adam J Horn, Subodh M Lele
Department of Pathology and Microbiology, University of Nebraska Medical Center. Omaha, NE, USA
- *Corresponding Author:
- Adam J Horn
Department of Pathology and Microbiology; University of
Nebraska Medical Center; 983135 Nebraska Medical Center
4350 Dewey Ave; Omaha, NE 68198-3135; USA
Phone: +1-402.559.4186
Fax: +1-402.559.6018
E-mail: ahor1@unmc.edu
Received March 11th, 2011 - Accepted April 4th, 2011
Keywords
Epidermal Cyst; Pancreas; Spleen
INTRODUCTION
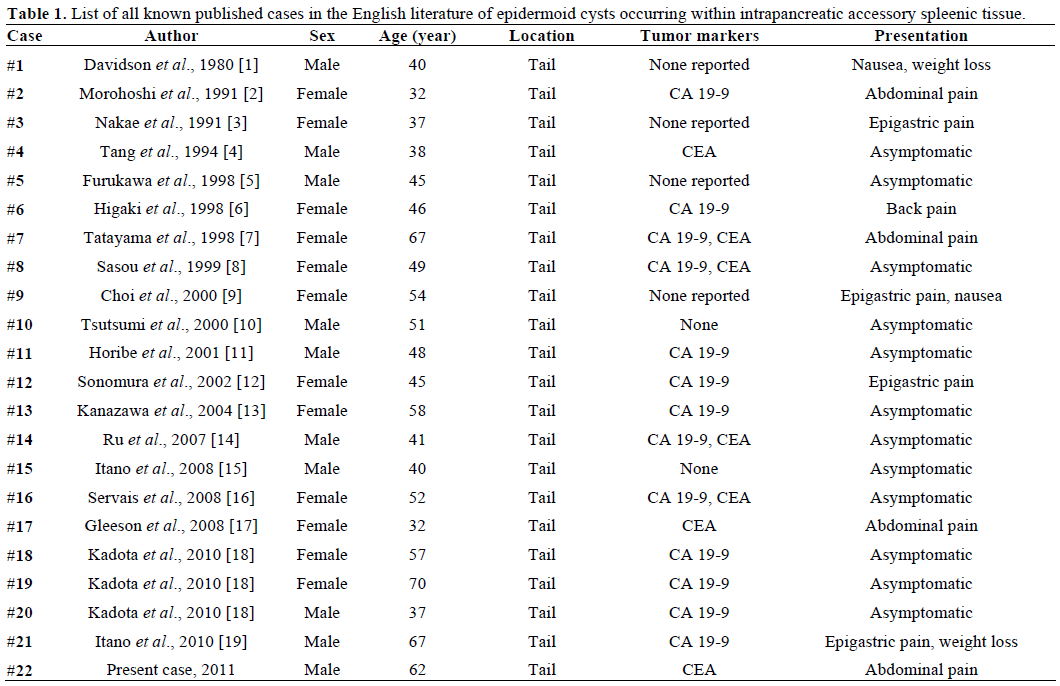
An epidermoid cyst occurring within an intrapancreatic accessory spleen is an extremely rare occurrence, with only 21 cases being described in the English literature since being first described in 1980 [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19]. As these lesions are often detected incidentally on imaging and are occasionally associated with increased serum CA 19-9 and CEA levels, their discovery can raise concern of a cystic pancreatic neoplasm [6, 7, 8, 11, 12, 13, 18, 20, 21]. In this report we describe an epidermoid cyst arising within an intrapancreatic accessory spleen in a symptomatic individual which prompted surgical exploration.
CASE REPORT
The patient is a 62-year-old male who presented to a rural clinic with complains of vague left-sided abdominal pain. A Computed tomography (CT) scan was obtained which showed a left-sided retroperitoneal mass with a possible cystic component (Figure 1). Resection of the mass was advised and the patient was transferred to our tertiary academic medical center. Abdominal surgical exploration revealed a large mass containing a cystic cavity (4.8x3.7x1.9 cm in aggregate) consisting of hemorrhagic fatty soft tissue and purulent appearing debris originating from the tail of the pancreas. The cyst was removed and sent for pathologic examination. Microscopy revealed multiple epidermoid cysts within accessory splenic tissue (Figure 2). The cysts were lined by stratified squamous epithelium, some of which was keratinizing, and were variable in size. Several cysts appeared to have ruptured and had surrounding fat necrosis and foreign body giant cells. The lining of the cysts was positive for CEA on immunohistochemistry. The findings are consistent with a benign epidermoid cyst arising within accessory splenic tissue in the tail of the pancreas. The patient recovered without complication.
Figure 1. Computed tomography (CT) scan demonstrating a large,
left-sided cystic mass near the tail of the pancreas.
Figure 2. a. Microscopic image of multiple cysts with stratified
squamous epithelium within splenic parenchyma. b. Immunoperoxidase
positivity for CEA in the epithelium of the cyst.
DISCUSSION
Epidermoid cysts of the spleen are a relatively infrequent cause of true non-parasitic splenic cysts. Accessory splenic tissue is a not uncommon finding at autopsy, with approximately 20% of accessory spleens occurring in the region of the tail of the pancreas [22]. However, epidermoid cysts occurring within an intrapancreatic accessory spleen are exceedingly rare, with only 21 previously reported cases (Table 1).
An epidermoid cyst histologically is comprised of a cystic space lined by keratinizing and non-keratinizing, non-hear bearing stratified squamous or cuboidal epithelium. All known cases arising in accessory splenic tissue have occurred within the tail of the pancreas, with sizes ranging from 1.5 to 11.5 cm, and have been reported to be both unilocular and multilocular [18]. It has been hypothesized that the cysts may arise due to a mesothelial inclusion that undergoes squamous metaplasia [23], as a byproduct of a teratoma [24], or as a communication between the pancreatic duct system with the intrapancreatic accessory spleen [7]. A recent report citing possible pancreatic duct material within an epidermoid cyst is supportive of the third theory [18]. Epidermoid cysts within an intrapancreatic accessory spleen have been associated with increases in serum CA 19-9 and CEA. Our case demonstrated immunoperoxidase positivity for CEA; no preoperative serum CEA or CA 19-9 levels were performed. D2-40 (a marker of epithelial origin) immunoperoxidase positivity has also recently been described [18].
The differential diagnosis includes pseudocysts, intraductal papillary mucinous neoplasms (IPMN), serous and mucinous cystadenomas, and lymphoepithelial cysts. A fine needle aspiration (FNA) of an epidermoid cyst within an intrapancreatic accessory spleen can yield pancreatic tissue, inflammatory debris, and fluid with increased CEA and CA 19-9 levels. These findings can be suggestive of malignancy; however, the presence of mature squamous epithelium and the lack of cytologically malignant appearing cells can be helpful in narrowing the differential diagnosis. There are no characteristic features to define the lesion on radiology, which when discovered can cause concern for a cystic pancreatic neoplasm as the radiographic findings can be quite similar [20]. There has been suggestion that the spleen and an intrapancreatic accessory spleen should demonstrate similar enhancement with contrast-enhanced CT imaging or MRI after superparamagnetic iron oxide administration [12, 21]. Because it is impossible to entirely rule out cystic pancreatic malignancies, surgical resection and histopathological examination is required for definitive diagnosis. Laparoscopic resection of an epidermoid cyst within an intrapancreatic accessory spleen has recently been described and offers the benefits of diminished pain and recovery time versus an open procedure in cases where the differential diagnosis favors a benign process but malignancy can not be ruled out [19].
In summary, an epidermoid cyst arising in intrapancreatic accessory spleen is a rare entity that can mimic malignant conditions. Because there is no reliable preoperative method to identify this entity, it remains a rare but important component in the differential diagnosis of cystic lesions in the tail of the pancreas.
Conflict of interest
The author has no potential conflicts of interest
References
- Davidson ED, Campbell WG, Hersh T. Epidermoid splenic cystoccurring in an intrapancreatic accessory spleen. Dig Dis Sci 1980;25:964-7. [PMID 7449592]
- Morohoshi T, Hamamoto T, Kunimura T, Yoshida E, Kanda M,Funo K, et al. Epidermoid cyst derived from an accessory spleen inthe pancreas. A case report with literature survey. ActaPathol.Jpn1991; 41:916-21. [PMID 1785350]
- Nakae Y, Hayakawa T, Kondo T, Shibata T, Kitagawa M, SakaiY, et al. Epidermoid cyst occurring in a pancreatic accessory spleen.J ClinGastroenterol 1991; 13:362-4. [PMID 2066557]
- Tang X, Tanaka Y, Tsutsumi Y. Epithelial inclusion cysts in anintrapancreatic accessory spleen. PatholInt 1994; 44:652-4. [PMID7952152]
- Furukawa H, Kosuge T, Kanai Y, Mukai K. Epidermoid cyst inan intrapancreatic accessory spleen: CT and pathologic findings. AJRAm J Roentgenol 1998; 171:271. [PMID 9648813]
- Higaki K, Jimi A, Watanabe J, Kusaba A, Kojiro M. Epidermoidcyst of the spleen with CA 19-9 or carcinoembryonic antigenproductions: report of three cases. Am J SurgPathol 1998; 22:704-8. [PMID 9630177]
- Tateyama H, Tada T, Murase T, Fujitake S, Eimoto T.Lymphoepithelial cyst and epidermoid cyst of the accessory spleen inthe pancreas. Mod Pathol 1998; 11:1171-7. [PMID 9872647]
- Sasou S, Nakamura S, Inomata M. Epithelial splenic cysts in anintrapancreatic accessory spleen and spleen. PatholInt 1999;49:1078-83. [PMID 10632928]
- Choi SK, Ahn SI, Hong KC, Kim SJ, Kim TS, Woo ZH, ShinSH. A case of epidermoid cyst of the intrapancreatic accessoryspleen. J Korean Med Sci 2000; 15:589-92. [PMID 11068999]
- Tsutsumi S, Kojima T, Fukai Y, Kanoh K, Shimura T, MochikiE, et al. Epidermoid cyst of an intrapancreatic accessory spleen. Acase report. Hepatogastroenterology 2000; 47:1462-4. [PMID11100377]
- Horibe Y, Murakami M, Yamao K, Imaeda Y, Tashiro K,Kasahara M. Epithelial inclusion cyst (epidermoid cyst) formationwith epithelioid cell granuloma in an intrapancreatic accessoryspleen. PatholInt 2001; 51:50-4. [PMID 11148465]
- Sonomura T, Kataoka S, Chikugo T, Hirooka T, Makimoto S,Nakamoto T, Sato M. Epidermoid cyst originating from anintrapancreatic accessory spleen. Abdom.Imaging 2002; 27:560-2. [PMID 12172998]
- Kanazawa H, Kamiya J, Nagino M, Uesaka K, Yuasa N, Oda K,et al. Epidermoid cyst in an intrapancreatic accessory spleen: a casereport. J.Hepatobiliary. J HepatobiliaryPancreatSurg 2004; 11:61-3. [PMID 15754048]
- Ru K, Kalra A, Ucci A. Epidermoid cyst of intrapancreaticaccessory spleen. Dig Dis Sci 2007; 52:1229-32. [PMID 17385039]
- Itano O, Shiraga N, Kouta E, Iri H, Tanaka K, Hattori H, et al.Epidermoid cyst originating from an intrapancreatic accessoryspleen. J HepatobiliaryPancreatSurg 2008; 15:436-9. [PMID18670847]
- Servais EL, Sarkaria IS, Solomon GJ, Gumpeni P, LiebermanMD. Giant epidermoid cyst within an intrapancreatic accessoryspleen mimicking a cystic neoplasm of the pancreas: case report andreview of the literature. Pancreas 2008; 36:98-100. [PMID18192891]
- Gleeson FC, Kendrick ML, Chari ST, Zhang L, Levy MJ.Epidermoid accessory splenic cyst masquerading as a pancreaticmucinous cystic neoplasm. Endoscopy 2008; 40(Suppl. 2):E141-2. [PMID 18633876]
- Kadota K, Kushida Y, Miyai Y, Katsuki N, Hayashi T, Bando K,et al. Epidermoid cyst in an intrapancreatic accessory spleen: threecase reports and review of the literatures. PatholOncol Res 2010;16:435-42. [PMID 19949910]
- Itano O, Chiba N, Wada T, Yuasa Y, Sato T, Ishikawa H, et al.Laparoscopic resection of an epidermoid cyst originating from anintrapancreatic accessory spleen: report of a case. Surg Today 2010;40:72-5. [PMID 20037845]
- Park MS, Kim KW, Lim JS, Lee JH, Kim JH, Kim SY, et al.Unusual cystic neoplasms in the pancreas: radiologic-pathologiccorrelation. J Comput Assist Tomogr 2005; 29:610-6. [PMID16163029]
- Motosugi U, Yamaguchi H, Ichikawa T, Sano K, Araki T,Takayama Y, et al. Epidermoid cyst in intrapancreatic accessoryspleen: radiological findings including superparamagnetic iron oxideenhancedmagnetic resonance imaging. J Comput Assist Tomogr2010; 34:217-22. [PMID 20351508]
- Halpert B, Alden ZA. Accessory spleens in or at the tail of thepancreas. A survey of 2,700 additional necropsies. Arch Pathol 1964;77:652-4. [PMID 14130052]
- Ough YD, Nash HR, Wood DA. Mesothelial cysts of the spleenwith squamous metaplasia. Am J ClinPathol 1981; 76:666-9. [PMID7293981]
- Lifschitz-Mercer B, Open M, Kushnir I, Czernobilsky B.Epidermoid cyst of the spleen: a cytokeratin profile with comparisonto other squamous epithelia. Virchows Arch 1994; 424:213-6. [PMID7514079]



