Keywords
Pancreatitis; Neurilemmoma
INTRODUCTION
Schwannomas (also called neurilemmomas) are encapsulated tumors made entirely of benign neoplastic Schwann cells [1-2]. They are the most common peripheral nerve tumors. They grow from peripheral nerves or nerve roots in an eccentric fashion with the nerve itself usually incorporated into the capsule [3]. Schwannomas usually grow, in descending order of frequency, in the lower extremity, upper extremity, trunk, head and neck, retroperitoneum, mediastinum, and pelvis [4].
Pancreatic schwannomas are very rare neoplasms. Based on a recent study in 2012, less than 50 cases of pancreatic schwannoma have been described in the English literature over the past thirty years [5]. This tumor is believed to arise from either autonomic sympathetic or parasympathetic branches of the Vagus nerve [6-7]. These tumors vary considerably in size and approximately two thirds are reported to undergo degenerative changes including cyst formation, calcification, hemorrhage, hyalinization and xanthomatous infiltration [8-9]. Preoperative diagnosis of pancreatic schwannoma can be challenging as the radiographic findings are similar to other more common pancreatic tumors such as pancreatic adenocarcinoma, neuroendocrine tumors or cystic neoplasms. Herein, we present a case of an enlarging pancreatic head schwannoma in a 72 year old woman who presented with a long standing history of dyspepsia and intermittent epigastric pain.
CASE REPORT
The patient is 72 year old Caucasian female with a past medical history of hypertension, hyperlipidemia, cervical stenosis and depression. She originally presented with worsening dyspepsia and intermittent epigastric pain for 2 years for which she sought medical attention. During the initial evaluation, a solid, enhancing mass in the anterolateral surface of the head of the pancreas was found on abdominal CT scan. There was no associated dilatation of the main pancreatic or common bile duct. Upper endoscopy revealed no lesions in the stomach or duodenum. During the following two years, the patient had multiple endoscopic ultrasound guided fine needle aspiration biopsies of the mass which were either nondiagnostic or resulted in benign appearing pancreatic tissue. She then underwent an open pancreatic biopsy with removal of a peri-pancreatic lymph node. These all revealed benign pancreatic tissue with fibrosis and no obvious evidence of malignancy. Her CEA and CA19- 9 levels were within normal limits. She was followed closely for 3 years with serial imaging and endoscopic ultrasounds, until an abdominal CT scan showed a substantial increase in the size of the pancreatic mass from 1.9 x 2.2 cm to 3.1 x 2.7cm (Figure 1). The pancreatic mass was described as a well-encapsulated tumor, without any cystic component. There were no other intra-abdominal lesions or pathologic lymphadenopathy noted. Magnetic resonance cholangiopancreatography showed normal caliber of the biliary tree and pancreatic duct. Endosc opic ultrasound confirmed a heterogeneous solid pancreatic head mass without pancreatic duct dilation (Figure 2). Her serum CEA and CA19-9 levels remained within normal limits throughout. Physical examination did not reveal any concerning findings, although the patient reported ongoing intermittent epigastric discomfort. Given the patient’s ongoing epigastric pain, and the enlarging size of the mass, a decision was made to proceed with surgery due to the concern that this may represent either a welldifferentiated pancreatic neuroendocrine tumor or a low grade pancreatic neoplasm (e.g. solid pseudopapillary neoplasm).
Figure 1. Contrast enhanced computed tomography (CT) scan of the
abdomen showing a pancreatic head mass (arrow), with heterogeneous
enhancement.
Figure 2. Endoscopic ultrasound reveals a solid heterogeneous mass
(24 mm by 23 mm maximal cross-sectional diameter), with a spiculated
appearance.
Figure 3. The tumor also showed alternating areas of hypercellularity
with edematous, myxoid, hypocellular foci, Antoni A (a.) and B (b.) areas.
No mitoses or necrosis are present. Associated hyalinized vessels (V) are
prominent.
The patient underwent an uneventful non-pylorus preserving pancreaticoduodenectomy. A wellencapsulated 3.5 cm mass was found arising from the superior aspect of the pancreatic head. Intraoperative ultrasound confirmed a solitary solid mass, with no evidence of lesions in the liver or remainder of the pancreas. She had an unremarkable post-operative course and was sent home on post-operative day 6.
On microscopic examination, sections of the 3.5 cm mass revealed a cellular spindle cell neoplasm with mild atypia and focal cystic degenerative changes (<img class="equation" src="https://www.primescholars.com/articles-images/). The lesion was relatively well defined and nerve tissue was noted at the periphery. On immunohistochemistry, the spindle cells were strongly positive for S-100 protein (Figure 4) and negative for pancytokeratin, CD-34, CD- 117, smooth muscle actin and Melan A. These findings were consistent with the diagnosis of a pancreatic schwannoma. At 12 months follow up, the patient is doing well without recurrent disease and resolution of her epigastric pain and dyspepsia.
Figure 4. Immunohistochemical examination of the pancreatic head
tumor shows diffuse and strong positivity to S100 protein (brown
staining), and negative for pancytokeratin, CD34, CD117, smooth muscle
actin and Melan-A.
DISCUSSION
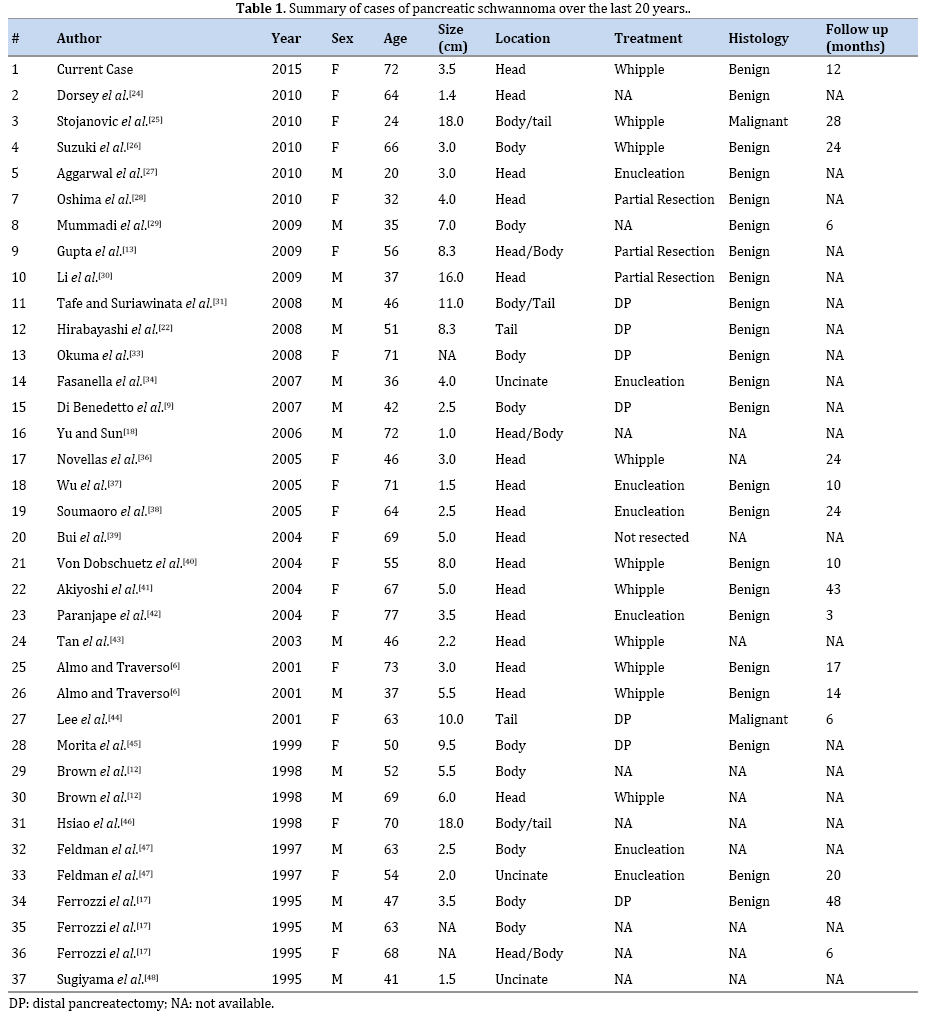
Pancreatic schwannomas are extremely uncommon neoplasms. The majority of these tumors are benign, with only 5 cases of malignant pancreatic schwannomas reported in the English literature [9-10] (Table 1). These tumors commonly affect adults (range: 20-87 years) without gender or race preference [5, 11, 12]. Pancreatic schwannomas vary in size (1-20 cm) and location. In a previous study, an association between tumor size and malignant potential has been suggested with larger tumors having more malignant potential [11]. They generally grow slowly but the incidence of degenerative changes including cyst formation, calcification, hemorrhage and lipid infiltrates is directly proportional to the size of the tumor.
The pancreatic head is the most common location representing 40% all of tumors, followed by the body (20%), and tail (15%). The uncinate process is the least common location (15%) [13-14]. There is a direct association with tumor location and symptoms. Tumors located in the head of the pancreas tend to be more symptomatic when compared with tumors in the periphery of the gland. In recent studies, up to 70% of the patients are symptomatic at the time of diagnosis [5-11], but most of the symptoms are vague and no specific including: dyspepsia, epigastric or back pain, and nausea. Jaundice is rare as the biliary tree is seldom occluded [15-16]. About 30% of the patients are asymptomatic and the lesions are found incidentally on abdominal imaging. Laboratory tests in the diagnosis of pancreatic schwannoma are not usually helpful; most of the patients have normal values and negative tumor markers.
Pre-operative diagnosis of pancreatic schwannomas is difficult even with multiple imaging modalities. Computed tomography (CT) scan can be helpful in distinguishing solid from cystic lesions and help in determining pancreatic duct dilation, the precise location of the mass, and its relation to mesenteric vessels. Certain pancreatic schwannoma characteristics on CT scan include; Antoni A and B components of the tumor that can be seen as low density and/or cystic degenerative areas [17, 18]. The more vascular Antoni A areas are usually enhancing lesions whereas Antoni B areas are frequently nonenhancing lesions [17, 18]. Magnetic resonance imaging (MRI) usually shows hypointensity on T1-weighted images and hyperintensity on T2-weighted images but like the CT features, these findings are non-specific.
The use of ultrasound-guided fine needle aspiration (FNA) in diagnosing pancreatic schwannomas remains controversial due to its high false negative rate. Based on previous literature reports only 1 out of 8 pancreatic schwannomas were diagnosed with ultrasound-guided FNA [19]. As was seen in our patient, multiple FNAs and even an open core biopsy did not confirm the diagnosis. The real challenge in the diagnosis of pancreatic schwannomas is the presence of cystic formation within the tumor. Lesions can often be misdiagnosed as benign pancreatic cysts. The definitive diagnosis can often only be made with histologic examination of a resected specimen and immunohistochemical staining.
Macroscopically, pancreatic schwannomas commonly appear cystic but they can also have a complete solid structure or a mixed pattern of solid and cystic formations throughout the tumor. Usually, they are well-demarcated, well-encapsulated, homogenous nodules that can have degenerative changes including hemorrhagic areas and xanthomous infiltrations that could give the tumor a yellow-tan coloration.
Microscopically, a typical pancreatic schwannoma is composed of hypercellular and hypocellular areas. Hypercellular or the Antoni A area consists of monomorphic spindle shaped Schwann cells full of poorly defined eosinophilic cytoplasm and pointed basophilic nuclei, in a variably collagenous stroma. These cells in the Antoni A areas show nuclear palisading, and parallel arrays of such palisades with intervening cell processes called Verocay bodies. Antoni B areas or hypocellular areas are also composed of Schwann cells with inconspicuous cytoplasm and nuclei appearing to be suspended in a copious myxoid, often microcystic matrix. The degenerative changes are usually recognized in the Antoni B areas. Normally, less than five mitotic figures per 10 high power fields can be seen in a benign schwannoma. Very rarely, pancreatic schwannomas can undergo malignant transformation, with only 5 cases described in the English literature. Malignant schwannomas are characterized by rapid growth, infiltration of adjacent structures, and multiple necrotic and hemorrhagic changes within the tumor [20, 21].
Immunohistochemically, pancreatic schwannomas are positive for S 100, Vimentin and CD 56. Conversely, spindle cells in pancreatic schwannomas stain negative for cytokeratin, CD117, desmin, CD34, AE1/AE3, alpha smooth muscle actin, and smooth muscle myosin. Cytogenetic analysis studies show that most schwannomas show either monosomy 22 or loss of 22q material [22, 32, 35].
The management of pancreatic schwannoma is strictly guided by the histologic results. With most of the tumors having a benign histology, tumor enucleation is the most common surgical procedure performed [23]. In cases where the tumor is showing malignant behavior (infiltration of tissue or close proximity to important vessels) or the frozen section is inconclusive, an oncologic, margin negative resection is recommended.
Although malignant peripheral nerve sheath tumors can be treated with Doxirubicin based chemotherapy, there are no data on the use of chemotherapy for pancreatic schwannomas. Other therapeutic options like radiation therapy, have not been studied for panncreatic schwannomas. Nonetheless, neurogenic schwannomas have been managed with radiation therapy for decades suggesting that radiation could be used in the future for the treatment of pancreatic schwannoma in patients that are not suitable for surgical resection [11].
In conclusion, we present a case of a 3.5 cm pancreatic schwannoma, which presented as intermittent epigastric pain and persistent dyspepsia and was followed by serial abdominal imagining for approximately two years, until a marked increase in the size of the lesion was observed. Due to its proximity to the portal vessels the consensus was to proceed with surgery, with histology revealing a benign pancreatic schwannoma. Although pancreatic schwannoma is a rare benign disease, it should be included in the list of differential diagnosis of all pancreatic masses with or without cystic changes. The lack pf specific symptoms, radiological characteristics and tumor markers from other pancreatic lesions, makes the preoperative diagnosis challenging with most of the cases diagnosed after surgical excision. Whenever possible the surgical treatment should aim to enucleation of the tumor. When this is not possible due to anatomic location or unclear diagnosis like in our case, more extended resection is justified. Close radiological follow-up is recommended after surgical excision but results from longer follow-up studies are needed in pancreatic schwannoma as there is not clear evidence of the behavior of these tumors after resection.
Conflicting Interest
The authors had no conflicts of interest
References
- Pilavaki M, Chourmouzi D, Kiziridou A, et al. Imaging of peripheral nerve sheath tumors with pathologic correlation: pictorial review. Eur J Radiol 2004; 52:229. [PMID: 15544900]
- Skovronsky DM, Oberholtzer JC. Pathologic classification of peripheral nerve tumors. Neurosurgery Clin N Am 2004; 15:157. [PMID: 15177315]
- Bhattacharyya AK, Perrin R, Guha A. Peripheral nerve tumors: management strategies and molecular insights. J Neurooncol 2004; 69:335. [PMID: 15527099]
- Abu-Zaid, Ahmed, et al. "Pancreatic tail schwannoma in a 44-year-old male: a case report and literature review." Case reports in oncological medicine 2013 (2013).
- T. Moriya, W. Kimura, I. Hirai et al., "Pancreatic schwannoma: case report and an updated 30-year review of the literature yielding 47 cases," World Journal of Gastroenterology, vol. 18, no. 13, pp. 1538-1544, 2012.
- Almo KM, Traveso LW. Pancreatic schwannoma: an uncommon but important entity. J Gastrointestinal Surg. 2001; 5:359-63. [PMID: 22509087]
- David S, Barkin JS. Pancreatic schwannoma. Pancreas 1993; 8:274-76. [PMID: 8460103]
- Paraiyapa C, Johnson SR, Khwaja K, Goldman H, Kruskal JB, Hanto DW. Clinical characteristics, treatment and outcome of pancreatic schwannomas. J GasterointestSurg 2004; 8:706-12. [PMID: 15358332]
- Di Benedetto F, Spaggiari M, de Ruvo M, et al., "Pancreatic schwannoma of the body involving the splenic vein: case report and review of the literature," European Journal of Surgical Oncology, vol. 33, no. 7, pp. 926-928, 2007. [PMID: 17049200]
- Coombs RS. "Case of the season: malignant neurogenic tumor of duodenum and pancreas," Seminars in Roentgenology, vol. 25, pp. 127-129, 1990. [PMID: 2112269]
- Móller Pedersen V, Hede A, Graem N. "A solitary malignant schwannoma mimicking a pancreatic pseudocyst: a case report," ActaChirurgicaScandinavica 1982; 148:697-8. [PMID: 7170905]
- Brown SZ, Owen DA, O'Connell JX, Scudamore CH. "Schwannoma of the pancreas: a report of two cases and a review of the literature." Modern Pathology 1998; 1178-1182.
- Gupta A, Subhas G, Mittal VK, Jacobs MJ. "Pancreatic schwannoma: literature review," Journal of Surgical Education 2009; 168-173. [PMID: 19712917]
- Tofigh AM, Hashemi M, Honar BN, Solhjoo F. "Rare presentation of pancreatic schwannoma: a case report."J Med Case Rep 2008; 2:268.
- Eggermont, V. Vuzevski, M. Huisman, K. De Jong, and J. Jeekel, "Solitary malignant schwannoma of the pancreas: report of a case and ultrastructural examination." J Surg Oncol 1987; 36:21-5. [PMID: 3626558]
- Walsh MM1, Brandspigel K. "Gastrointestinal bleeding due to pancreatic schwannoma complicating von Recklinghausen"s disease,? Gastroenterology 1989; 1550-1551. [PMID: 2511055]
- Ferrozzi F, Bova D, Garlaschi G. "Pancreatic schwannoma: report of three cases." ClinRadiol 1995; 50:492-5. [PMID: 7614798]
- Yu RS, Sun JZ. "Pancreatic schwannoma: CT findings," Abdominal Imaging, Abdom Imaging 2006; 31:103-5. [PMID: 16132429]
- Yu GH, Sack MJ, Baloch Z, Gupta P., "Difficulties in the fine needle aspiration (FNA) diagnosis of schwannoma." Cytopathology 1999; 10:186-94.
- Enzinger FM, Weiss SW. Benign Tumors of the peripheral nerves in Soft Tissue, F.M.Enzinger, Ed., pp 821-828, Elseiver Saunders, St.Louis, Mo, USA, 3rd Edition,1995.
- Weiss SW, Langloss JM, Enzinger FM. "Value of S-100 protein in the diagnosis of soft tissue tumors with particular reference to benign and malignant Schwann cell tumors." Lab Invest 1983; 49:299-308.
- Hirabayashi K, Yasuda M, Umemura S, Itoli H, Itoli J, Yazawa N, et al. Cytological features of the cystic fluid of pancreatic schwannoma with cystic degeneration. A case report JOP. 2008; 9:203-8. [PMID: 18326930]
- Prasad D1, Jalali R, Shet T. Shet, "Intracranial subfrontalschwannoma treated with surgery and 3D conformal radiotherapy." Neurol India 2004; 52:248-50. [PMID: 15269484]
- Dorsey F, Taggart MW, Fisher WE. Image of the month. Pancreatic schwannoma. Arch Surg2010; 145: 913-914. [PMID: 20855766]
- Stojanovic MP, Radojkovic M, Jeremic LM, Zlatic AV, Stanojevic GZ, Jovanovic MA, et al. Malignant schwannoma of the pancreas involving transversal colon treated with en-bloc resection. World J Gastroenterol 2010; 16: 119-122. [PMID: 20039458]
- Suzuki S, Kaji S, Koike N, Harada N, Hayashi T, Suzuki M, Hanyu F, Ban S. Pancreatic schwannoma: a case report and literature review with special reference to imaging features. JOP 2010; 11: 31-35. [PMID: 20065549]
- Aggarwal G, Satsangi B, Shukla S, Lahoti BK, Mathur RK, Maheshwari A. Rare asymptomatic presentations of schwannomas in early adolescence: three cases with review of literature. Int J Surg 2010; 8: 203-206. [PMID: 20167297]
- Oshima M, Yachida S, Suzuki Y. Pancreatic schwannoma in a 32-year-old woman mimicking a solid-pseudopapillary neoplasm. Clin Gastroenterol Hepatol 2010; 8: e1-e2. [PMID: 19501191]
- Mummadi RR, Nealon WH, Artifon EL, Fleming JB, Bhutani MS. Pancreatic Schwannoma presenting as a cystic lesion. Gastrointest Endosc 2009; 69: 341; discussio 341. [PMID: 19185694]
- Li S, Ai SZ, Owens C, Kulesza P. Intrapancreaticschwannoma diagnosed by endoscopic ultrasound-guided fine-needle aspiration cytology. DiagnCytopathol 2009; 37: 132-135. [PMID: 19031416]
- Tafe LJ, Suriawinata AA. Cystic pancreatic schwannoma in a 46-year-old man. Ann DiagnPathol 2008; 12: 296-300. [PMID: 18621000]
- Todd KE, Lewis MP, Gloor B, Kusske AM, Ashley SW, Reber HA. Management decisions for unusual periampullary tumors. Am Surg 1997; 63:927-932. [PMID: 9322675]
- Okuma T, Hirota M, Nitta H, Saito S, Yagi T, Ida S, Okamura S, Chikamoto A, Iyama K, et al. Pancreatic schwannoma: report of a case. Surg Today 2008; 38: 266-270. [PMID: 18307004]
- Fasanella KE, Lee KK, Kaushik N. Clinical challenges and images in GI. Benign schwannoma of the pancreatic head. Gastroenterology 2007; 132: 489, 830. [PMID: 17261290]
- Urban BA, Fishman EK, Hruban RH, Cameron JL. CT Findings in cystic schwannoma of the pancreas. J Comput Assist Tomogr 1992; 16:492-493. [PMID: 1592939]
- Novellas S, Chevallier P, Saint Paul MC, Gugenheim J, Bruneton JN. MRI features of a pancreatic schwannoma. Clin Imaging 2005; 29: 434-436. [PMID: 16274899]
- Wu YL, Yan HC, Chen LR, Chen J, Gao SL, Li JT. Pancreatic benign schwannoma treated by simple enucleation: case report and review of literature. Pancreas 2005; 31: 286-288. [PMID: 16163062]
- Soumaoro LT, Teramoto K, Kawamura T, Nakamura N, Sanada T, Sugihara K, Arii S. Benign schwannoma of the pancreas. J Gastrointest Surg 2005; 9: 288-290. [PMID: 15694826]
- Bui TD, Nguyen T, Huerta S, Gu M, Hsiang D. Pancreatic schwannoma. A case report and review of the literature. JOP 2004; 5: 520-526. [PMID: 15536295]
- Von Dobschuetz E, Walch A, Werner M, Hopt UT, Adam U. Giant ancient schwannoma of pancreatic head treated by extended pancreatoduodenectomy. Pancreatology 2004; 4: 505-508. [PMID: 15316226]
- Akiyoshi T, Ueda Y, Yanai K, Yamaguchi H, Kawamoto M, Toyoda K, Hayashi T, Ohuchida J. Melanoticschwannoma of the pancreas: report of a case. Surg Today 2004; 34: 550-553. [PMID: 15170556]
- Paranjape C, Johnson SR, Khwaja K, Goldman H, Kruskal JB, Hanto DW. Clinical characteristics, treatment, and outcome of pancreatic schwannomas. J Gastrointest Surg 2004; 8:706-712. [PMID: 15358332]
- Tan G, Vitellas K, Morrison C, Frankel WL. Cystic schwannoma of the pancreas. Ann DiagnPathol 2003; 7: 285-291. [PMID: 14571430]
- Lee JS, Kim HS, Jung JJ, Han SW, Kim YB. Ancient schwannoma of the pancreas mimicking a cystic tumor. Virchows Arch 2001; 439:697-699. [PMID: 11764392]
- Morita S, Okuda J, Sumiyoshi K, et al. Pancreatic schwannoma: report of a case. Surg Today 1999; 29:1093-1097. [PMID: 10554337]
- Hsiao WC, Lin PW, Chang KC. Benign retroperitoneal schwannoma mimicking a pancreatic cystic tumor: case report and literature review. HepatoGastroenterol 1998; 45:2418-2420. [PMID: 9951935]
- Feldman L, Philpotts LE, Reinhold C, Duguid WP, Rosenberg L. Pancreatic schwannoma: report of two cases and review of the literature. Pancreas. 1997; 15:99-105.
- Sugiyama M, Kimura W, Kuroda A, Muto T. Schwannoma arising from peripancreatic nerve plexus. AJR Am J Roentgenol. 1995; 165:232.





