Keywords
Cholangiopancreatography, Endoscopic Retrograde; Contrast Media; Microscopy, Electron; Microscopy, Polarization; Pancreatitis
Abbreviations
EM: electron micrographs; WBC: white blood cell
INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) induced pancreatitis affects approximately 1-7% of patients with occasional significant morbidity and rarely mortality [1]. Currently the etiology of ERCP related pancreatitis is felt to be multifactorial including both factors related to the procedure and to the patient. Speculation centers around several procedure related factors including rate and volume of injected contrast material, pressure of injection, and edema resulting from multiple attempts at cannulation of the sphincter of Oddi. Lack of a suitable animal model has further hindered the evaluation of the relative contribution of the various factors that may lead to post ERCP pancreatitis.
The type of contrast agent used has been hypothesized to affect the chance of pancreatitis associated with ERCP with earlier studies suggesting decreased risks of pancreatitis with low osmolar non-ionic contrast agents [2, 3, 4]. This has been challenged by other clinical studies that have not found a significant difference in post ERCP pancreatitis rate based upon the type of contrast agent used [5, 6, 7].
Due to the continued controversy and the lack of any histologic evidence of ionic higher osmolarity contrast agents causing more pancreatitis and pancreatic injury we examined the effect of both an ionic high osmolarity and a non-ionic low osmolarity contrast agent in a canine model with subsequent light and electron microscopy examinations of the pancreas.
MATERIAL AND METHODS
Six mongrel dogs were the subjects of the study. The dogs were anesthetized with intravenous surital (10 mg/kg), intubated, and maintained on inhaled halothane gas. After shaving and prepping the abdomen with betadine, a midline incision was performed and the duodenum exposed. The second portion of the duodenum was opened, and the ampulla of Vater cannulated under direct visualization with the catheter uniformly 1.5 cm into the papilla. The cannula was sutured in place 1.0 cm from the papilla and the duodenum and abdominal wall were closed prior to injection of the contrast agent.
Contrast material was injected under fluoroscopic control with stable gentle pressure until full acinarization (defined as opacification of acini in the pancreatic parenchyma by contrast) became apparent. Overhead films were taken to document correct placement of the catheter and then complete acinarization. Three dogs received diatrizoate meglumine 60%, an ionic contrast agent with osmolarity of 1,415 mosM (Hypaques, Sanofi-Winthrop Pharmaceuticals, New York, NY, USA). Three dogs received iopamidol, a non-ionic agent with osmolarity of 672 mosM (Omnipaque 300, Sanofi-Winthrop Pharmaceuticals, New York, NY, USA). Because of slight differences in the size of the dogs and also in the size and shape of each individual canine pancreas it was felt that visualization of acinarization by fluoroscopy would serve as the best control rather than amount of or pressure of injection of the contrast agents. The volume of contrast needed to achieve acinarization was recorded for each dog. Pancreatograms were interpreted by a staff radiologist unaware of the type of contrast used to ensure that the pancreatic ducts in each dog were fully and completely acinarized.
After waking from anesthesia the dogs were transferred to animal care centers. All dogs were allowed to have food and water ad lib over the next 48 hours.
Serum amylase and white blood cell (WBC) count determinations were obtained from each dog at zero, six, twelve, twenty-four, and forty-eight hours after the procedure.
At forty-eight hours post procedure the animals were sacrificed and the mongrel pancreases were removed and immediately fixed in 10% buffered formalin with cuts being made through the proximal and distal pancreas. Specimens were then prepared by fixation in paraffin, microtoming, and staining with hematoxylin and eosin (H&E).
The H&E and electron micrographs (EM) of the pancreatic specimens were each read by a single staff pathologist who was blinded to the type of contrast used. On H&E micrographs the specimen was examined for evidence of interstitial edema and focal areas of fat necrosis as seen in mild interstitial pancreatitis and destruction of pancreatic parenchyma and necrosis of acinar and ductal tissues as seen in more severe pancreatitis. [8]. EMs of both the proximal and distal duct of each animal were obtained and examined for cellular injury. EM criteria for cellular injury was based upon the presence of myelin figures, presence of mitochondrial swelling, and loss of christae within the mitochondria of the pancreatic cells. Severity of cellular injury on electron microscopy was classified as mild (less than 25% of mitochondria affected), moderate (between 25-50% of mitochondria affected), and severe (greater than 50% of mitochondria affected). Comparisons were made between the dogs injected with ionic high osmolar contrast and the dogs injected with non-ionic low osmolar contrast for the presence of pancreatitis on light microscopy and for the presence of cellular damage on electron microscopy.
STATISTICS
Data are reported as mean and standard deviation (SD) values. At each time point of the experiment the differences in the mean WBC count and amylase levels were compared in the two groups utilizing the ANOVA test. Ninety-five percent confidence intervals (95% CI) and levels of significance were reported for the differences in the means of WBC count and amylase levels in the two groups. All statistical analysis was carried-out using SAS software v 8.2.
ETHICS
All procedures were preapproved by the University of Wisconsin Institutional Review Board (IRB) and Research Animal Resource Center (RARC) animal care committee and met federal guidelines for the humane use and treatment of animals.
RESULTS
Pancreatic duct injection and visualization was present in all of the animals. Complete acinarization was present in all cases as documented by the endoscopist/surgeon at the time of the procedure and the radiologist in reviewing the films afterwards blinded to the type of contrast used. Acinarization as graded by the radiologist was felt to be of moderate to marked in all of the dogs (Figure 1). No difference between the degree of opacification of the pancreatic duct or acinarization was detected based upon the type of contrast injected. The mean (±SD) amount of contrast needed to result in complete acinarization for the group of dogs receiving ionic contrast was 6.0±2.0 mL and the mean amount of contrast the non-ionic group received was 7.8±4.1 mL of contrast. There was no significant difference in the amount of contrast the two groups received to achieve complete acinarization of the pancreas (P=0.523) with a mean difference of 1.8 mL (95% CI: -5.4 to +9.1 mL).
Figure 1. Fluoroscopic image of canine pancreas after
contrast injection showing marked acinarization of the
pancreatic duct.
The procedure was technically difficult in one animal (D), in which there was difficulty in performing adequate cannulation of the pancreatic duct sufficient to ensure stability of the cannula. This led to repeated attempts at deep cannulation before the cannula was adequately situated 1.5 cm into the duct.
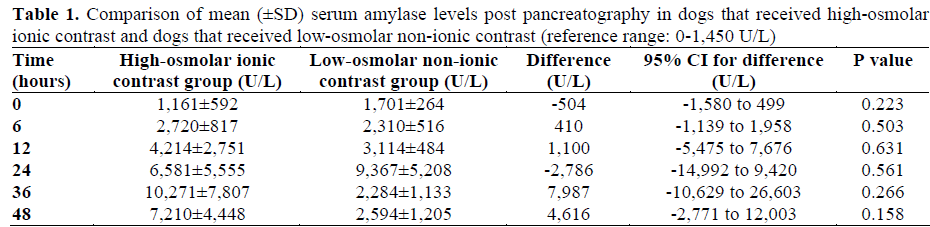
All of the animals developed a significant degree of hyperamylasemia that was approximately 6 to 7 fold higher than the normal amylase level. The amylase level tended to peak 24-36 hours post procedure (Table 1). There was no significant differences between the mean peak amylase levels of the ionic and non-ionic contrast group of dogs (10,271 U/L vs. 9,367 U/L; difference in means: 904 U/L, 95% CI: - 14,140 to 15,948 U/L; P=0.876).
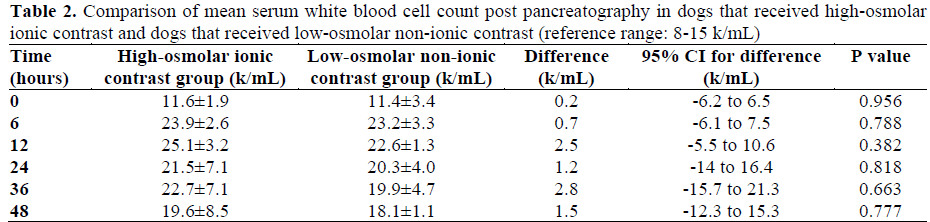
The WBC count level also increased in all animals after the pancreatic injection (Table 2). The WBC count tended to peak at 6-12 hours post procedure. There was no significant differences between the mean peak WBC count levels of the ionic and non-ionic contrast group of dogs (25.8 k/mL vs. 24.1 k/mL; difference in means: 1.7 k/mL, 95% CI: -6.4 to 9.9 k/mL; P=0.586).
The dogs showed no obvious evidence of clinical disease except for dog D which refused food and water for the 48 hours post pancreatic injection and appeared withdrawn, unwilling to come out of its cage for either feedings or activity.
On hematoxylin and eosin staining none of the animals in either contrast group showed histologic evidence of pancreatitis including no evidence of an acute inflammatory reaction, edema, fat necrosis, nor necrosis of pancreatic tissue (Figure 2).
Figure 2. Light microscopy image of canine pancreatic
duct 48 hours after injection of contrast revealing
normal ductal system without evidence of
inflammation or injury.
On electron microscopy two dogs showed evidence of reversible cellular injury, manifested primarily by mitochondrial swelling and the presence of myelin figures (Figure 3). In both of these animals injury was seen in both the proximal and the distal pancreatic duct. In both of the dogs showing cellular injury, the injury was classified as minor involving less than 25% of the mitochondria observed. Both dogs that showed evidence of injury on electron microscopy post-procedure were from the group that received the non-ionic low osmolar contrast medium.
Figure 3. Electron microscopy , 2000 magnification, of
Dog D pancreas showing pancreatic cellular injury as
demonstrated by the presence of myelin figures
(arrows) and swollen mitochondria with loss of christae
(arrowheads).
DISCUSSION
ERCP induced pancreatitis is a unique entity because it is a potentially preventable form of pancreatitis. While occurring in a minority of patients, it is a purely iatrogenic complication that can add significant morbidity to the procedure. Thus, any preventive measure which can aid in decreasing the incidence and severity of this complication would be of clinical benefit.
Controversy in the literature is present in regard to the potential benefits of non-ionic, low osmolar contrast media. Several nongastrointestinal studies have shown that nonionic contrast agents are less likely to cause tissue necrosis than ionic agents when injected subcutaneously and are potentially less toxic in the subarachnoid space and cardiovascular system [9, 10]. Further, high osmolar ionic contrast media has been found to be more cytoxic with increased chromosomal damage and inhibited cell growth as compared to low osmolar non-ionic contrast media in dog gallbladder epithelial cells [11].
These studies and others have led to clinical trials directly examining whether using low osmolar non-ionic contrast medium in the pancreatic duct at the time of the ERCP lessens the clinical chance of pancreatitis. Early studies in the 1980s and 1990s suggested a potential clinical benefit with decreased complications when non-ionic contrast agents were used for pancreatography during ERCP. O’Connor et al. randomized 85 patients to receive either diatrizoate meglumine, an ionic contrast medium or iopamidate, a non-ionic contrast group. The group of patients receiving the non-ionic contrast agent was found to have significantly lower and less frequent elevations of amylase and lipase [4]. Barkin et al. also found that patients who received a non-ionic low osmolar contrast agent at ERCP to have significantly lower amylase and lipase levels post ERCP. In addition it was found that fewer patients developed clinical pancreatitis as compared to the patients who received an ionic contrast agent [2].
These and other studies suggesting the use of non-ionic contrast medium to prevent post ERCP pancreatitis were criticized for drawing results with few patients studied and poor methods that did not differentiate between the type of patients undergoing ERCP nor the difficulty of the procedure. Subsequently, a large multi-center study was performed which compared non-ionic versus ionic contrast agents in greater than 1,600 patients with the study divided into subgroups based on patient characteristics and ERCP procedure complexity [6]. No difference was found in post procedure pancreatitis between the groups based upon what type of contrast agent was used.
However, all of the studies above compared the use of different contrast agents in clinical settings with clinical pancreatitis or elevation of pancreatic enzymes as the endpoints. More recent studies [12, 13, 14] all have suggested that clinical pancreatitis post ERCP is a result of multiple factors. The existing clinical studies comparing ionic and non-ionic contrast agents no matter how well designed did not and could not control for all factors other than the type of contrast agent used.
Thus, determining if the instillation of different contrast agents into the pancreatic duct causes varying amounts of damage to the pancreas and pancreatic cells may be better determined by histologic confirmation. Lacking the ability to safely obtain tissue samples in humans from the pancreas, animal models may represent a better opportunity to define the effect of non-ionic versus ionic contrast in the pancreas. To date, only two animal studies have used histologic evidence to compare the infusion of differing contrast agents into the pancreas and the two studies have arrived at conflicting results.
Bub et al. examined the effect of injecting varying contrast agents into the pancreatic ducts of cats and found the least amount of damage with low osmolar non-ionic contrast mediums by examining the pancreas with electron microscopy [10]. Conversely, Saari et al. using only hematoxylin-eosin stains and light microscopy found that an ionic contrast agent resulted in the least amount of damage in a pig model [15]. Thus, only two animal histologic studies examining various contrast media have been performed and these two studies have found differing results with regard to the damage caused by ionic vs. nonionic contrast.
Our study attempted to further define what effect the type of contrast agent used in the pancreatic duct has on the pancreas with particular attention paid to determining if a non-ionic low osmolar contrast agent decreases the amount of pancreatic inflammation and cellular damage. We chose to compare the dog pancreas after injecting the pancreatic duct with either high osmolar ionic or low osmolar non-ionic contrast using the serum markers of amylase and WBC, and more importantly using both light microscopy and electron microscopy to assess for histologic pancreatic injury.
Previous clinical studies have used amylase as a marker to show that non-ionic contrast agents resulted in less pancreatic damage. While amylase released into the serum can be a surrogate marker for pancreatic inflammation no proof exists that there is a direct relationship between amylase peak post ERCP and pancreatic cellular damage. However, the fact that amylase levels peaked to well greater than 5 times normal in the dogs in both groups and the WBC count rose within 24 hours suggests at a minimum the injection and acinarization resulted in at least the biochemical presence of pancreatitis in both contrast groups. Even noting that serum amylase post pancreatography and serum WBC count are poor markers for definitively identifying pancreatitis and pancreatic cell injury, the finding that the dogs who received the non-ionic contrast did not have lower serum amylase levels and white blood cell counts may indirectly support that non-ionic contrast does not lessen post pancreatography pancreatitis.
None of the dog pancreases showed evidence of pancreatitis on H&E staining. Given that there was no evidence of tissue damage on light microscopy our study demonstrates that if the histology of pancreatic injury is to be best studied electron microscopy is important and light microscopy may not be sensitive enough to detect subtle differences in cellular injury.
Finally and notably, none of the dogs that received the ionic, high osmolar contrast showed any evidence of pancreatic cellular injury on electron microscopy. Counter to the hypothesis that non-ionic, low osmolar agents would result in less cellular injury in the pancreas was the finding in our study that the only two dogs that showed evidence of cellular injury on electron microscopy were found in the groups that received omnipaque, the non-ionic, low osmolar contrast agent. This suggests first, consistent with recent clinical studies, it is likely that low osmolar non-ionic contrast agents do not result in less pancreatic damage or pancreatitis. Further, more closely examining the dogs that did show evidence of reversible cellular damage on EM suggests even more so that contrast medium is not as important as other factors post ERCP in causing pancreatic cellular injury. Dog D, the dog that showed the most mitochondrial swelling required the most contrast to achieve acinarization and required by far the most manipulation at the papilla and duct to achieve acinarization. Thus factors that have been shown to be a risk for post ERCP pancreatitis such as difficult cannulation, papillary trauma, and increased number of pancreatic injections are likely to be more important risk factors for pancreatic cellular damage, reversible or otherwise and pancreatitis than the type of contrast used [16].
While our study because of the small number of dogs examined does not definitively disprove that non-ionic low osmolar contrast agents cause less pancreatitis and pancreatic cellular injury it adds further histologic evidence to the growing clinical evidence that the type and osmolarity of contrast medium used likely does not increase or decrease toxicity to the pancreas at the time of ERCP. Given present findings and the collection of previous clinical studies in the literature it is likely that non-ionic low osmolar contrast agents used during ERCP do not significantly prevent post-ERCP pancreatitis and pancreatic cell injury.
References
- Mallery JS, Baron TH, Dominitz JA, Goldstein JL, Hirota WK, Jacobson BC, et al. Complications of ERCP. Gastrointest Endosc 2003; 57:633-8. [PMID 12709688]
- Barkin JS, Casal GL, Reiner DK, Goldberg RI, Phillips RS, Kaplan S. A comparative study of contrast agents for endoscopic retrograde pancreatography. Am J Gasterenterol 1991; 86:1437-41. [PMID 1928034]
- Banerjee AK, Grainger SL, Thompson RP. Trial of low versus high osmolar contrast media in endoscopic retrograde cholangiopancreatography. Br J ClinPract 1990; 44:445-7. [PMID 2282293]
- O'Connor HJ, Ellis WR, Manning AP, Lintott DJ, McMahon MJ, Axon AT. Iopamidol as contrast agent in endoscopic retrograde pancreatography: a prospective randomized comparison with diatrizoate. Endoscopy 1988; 20:244-7. [PMID 3168937]
- Goebel C, Hardt P, Doppl W, Temme H, Hackstein N, Klor HU. Frequency of pancreatitis after endoscopic retrograde cholangiopancreatography with iopromid or iotrolan: a randomized trial. EurRadiol 2000; 10:677-80. [PMID 10795554]
- Johnson GK, Geenen JE, Bedford RA, Johanson J, Cass O, Sherman S, et al. A comparison of nonionic versus ionic contrast media: results of a prospective multicenter study. Midwest Pancreatobiliary study group. Gastrointest Endosc 1995; 42:312-6. [PMID 8536898]
- Sherman S, Hawes RH, Rathgaber SW, Uzer MF, Smith MT, Khusro OE, et al. Post-ERCP pancreatitis: randomized, prospective study comparing a low- and high-osmolarity contrast agent. Gastrointest Endosc 1994; 40:422-7. [PMID 7926531]
- Vinay K, Nelso F, Abul A. Robbins and Cotran Pathologic Basis of Disease. 7th ed. Philadelphia, PA, USA: WB Saunders/Elsevier, 2005. [ISBN 721601871]
- Almen T, Aspelin P. Cardiovascular effects of ionic monomeric, ionic dimeric and non-ionic contrast media. Effects in animals on myocardial contractile force, pulmonary and aortic blood pressure and aortic endothelium. Invest Radiol 1975; 10:557-63. [PMID 1201937]
- Bub H, Burner W, Riemann JF, Stolte M. Morphology of the pancreatic ductal epithelium after traumatization of the papilla of Vater or endoscopic retrograde pancreatography with various contrast media in cats. Scand J Gastroenterol 1983; 18:581-92. [PMID 6675180]
- Ju YM, Kim MH, Lee SK, Seo DW, Min YI, Kim JY. Comparative cytotoxicity of low-osmolar nonionic and high-osmolar ionic contrast media to dog gallbladder epithelial cells. Gastrointest Endosc 2002; 55:382-6. [PMID 11868013]
- Freeman ML, DiSario JA, Nelson DB, Fennerty MB, Lee JG, Bjorkman DJ, et al. Risk factors for post- ERCP pancreatitis : a prospective, multicenter study. Gastrointest Endosc 2001; 54:425-34. [PMID 11577302]
- Masci E, Toti G, Mariani A, Curioni S, Lomazzi A, Dinelli M, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol 2001; 96:417-23. [PMID 11232684]
- Loperfido S, Angelini G, Benedetti G, Chilovi F, Costan F DeBerardinis F, et al. Major early complications from diagnostic and therapeutic ERCO: a prospective multicenter study. Gastrointest Endosc 1998; 48:1-10. [PMID 9684657]
- Saari A, Kivisaari C, Standertskjold-Nordenstam C, Brackett K, Schroder T. Experimental pancreatography: a comparison of three contrast media. Scand J Gastroenterol 1988; 23:53-58. [PMID 3344398]
- Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: A comprehensive review. Gastrointest Endosc 2004; 59:845-64. [PMID 15173799]




