Keywords
Pancreatic Ducts; Dilatation; Kidney Transplantation; Pancreas Transplantation
Abbreviations
EMG: electromyography; i.v.: intravenous; MMF: mycophenolate mofetil; PDC: pancreaticoduodenocystostomy; SPK: simultaneous pancreas-kidney; TAC: tacrolimus; US: ultrasound; VCUG: voiding cystourethrogram
INTRODUCTION
Simultaneous pancreas-kidney (SPK) transplantation has become a successful procedure for the management of patients with type I (insulin-dependent) diabetes mellitus that have associated end stage renal disease [1]. The whole pancreas transplantation is performed most commonly with pancreatic exocrine bladder drainage via a pancreaticoduodenocystostomy (PDC) [2]. Radiologic imaging plays a major role in the evaluation of the transplanted pancreas in the postoperative period and especially in the early detection of possible complications. A variety of imaging modalities are used, including computed tomography scan [3, 4, 5], ultrasound (US) [5, 6], scintigraphy [5], and magnetic resonance [7, 8]. The principal contributions of US Doppler are in the assessment of pancreatic circulation, evaluation of peripancreatic fluid collections, and possible rejection. Dilatation of the allograft pancreatic duct following bladderdrained SPK transplant is not well described in the transplant literature. We correlate this finding with clinical significance.
PATIENTS AND METHODS
From February 1993 to December 1999, 145 SPK transplants were performed (74 males, 71 females). All recipients were adults (median age of 38 years, range 23 to 56) with type I insulin dependent diabetes and endstage renal disease. All patients underwent pre-transplant voiding cystourethrogram (VCUG). Five patients were noted to have a dilated pancreatic duct on US examination of the graft one to eighteen months posttransplant. The sonograms and medical records of these five patients were retrospectively reviewed.
No sign of reflux, trabeculation or post-void residual urine were seen in these 5 patients in the preoperative VCUG. The standard donor operation was performed and generally included procurement of the liver, both kidneys and whole pancreas and duodenum. The recovery and preparation of the pancreaticoduodenal block has been modified as described before [9].
Immunosuppression Protocol
From February 1993 to June 1994, induction immunosuppression consisted of 14 days of murine monoclonal antibody OKT3 (5 mg/day), cyclosporine A, methylprednisolone, and azathioprine. In July 1994, tacrolimus (TAC) was introduced and started in the operating room by continuous intravenous (i.v.) infusion at doses of 0.02 to 0.03 mg/kg/day, and continued for several days until the patient could tolerate oral medication. TAC i.v. was switched to the oral formula at 0.1 mg/kg every 12 hours with several days of overlap. TAC was titrated based on whole blood concentrations monitored daily [10]. Recently mycophenolate mofetil (MMF) has been used to replace azathioprine. From May 1997 to December 1997, the protocol was adjusted to eliminate OKT3 antibody therapy [11]. Starting in January of 1998, SPK were performed with a new quadruple immunosuppression protocol that was introduced as part of a multicenter trial. This consisted of anti-IL2-rmAb, 1 mg/kg i.v. perioperatively and every 14 days for a total of five doses. TAC i.v. was started during surgery at 1 mg/over 24 hours. The i.v. dose was adjusted with oral dose of TAC to maintain trough level of 10-15 ng/ml. Methylprednisolone was given 1gm on the day of surgery and tapered to 0.1 mg/kg/day over 3 months, and MMF 1 gm twice a day orally. All 5 patients with dilatation of the allograft pancreatic duct were induced with OKT3, TAC, MMF and steroids.
Ultrasound Study
Postoperatively US examinations were performed using real time equipment (Acuson, Mountain View, CA, with a 3.5 or 5 MHz transducer, or Diasonics DZ Gateway, Milpitas, CA, with a 3.5 or 5 MHz transducer). Baseline sonograms are routinely performed postoperatively and whenever the patient's clinical condition warrants it.
The size, contour and echogenicity of the graft were observed. The pancreatic duct was visualized and its diameter measured. Normal pancreatic ductal dimensions were assumed to be 2 mm or less. Normal pancreatic ductal dimensions have not been established in the allograft pancreas. However in our experience the normal pancreatic duct is either not visualized or is less than 2 mm, similar to measurements in the native pancreas. The pancreatic dust was differentiated from the remnant of the common bile duct, which can be seen within the head of the pancreas and may measure up to 7 mm normally. Color duplex of the allograft was performed with imaging and sampling of the arterial anastomosis, the superior mesenteric, the splenic artery, the intrapancreatic arterial branches, the superior mesenteric, splenic vein and the portal vein. Color Doppler was used to identify blood flow within the parenchyma and major vessels.
Video-Urodynamic Studies
Video-urodynamic study is a series of tests and x-rays that give a detailed look at the function of the bladder, urethra and sphincters. The urodynamic study involves cystometry, which is the major portion of the urodynamic workup and requires the placement of a 7F urodynamic catheter. This allows measurement of bladder pressures during the filling and the voiding phase of the study. The bladder is filled with dilute contrast at room temperature through this catheter. Standard filling rates of 35 cc per minute are used. A second pressure catheter is placed in the lower portion of the rectum or in the posterior vaginal vault. This measures intra-abdominal pressure. Sphincter electromyography (EMG) is obtained by surface electrodes, wire electrodes, or needle electrodes placed in the perianal area. Perineal EMG is recorded during filling and voiding phase of the study. Uroflow studies are obtained as free flow rates and post-void residuals are examined after each evaluation. All urodynamic studies are performed in duplicate and the findings are averaged to give the final parameters. Fluoroscopy control is performed during the filling and voiding phase of the study.
ETHICS
This is a retrospective study and data were collected in the usual clinical practice.
STATISTICS
Simple descriptive statistics were reported: median, minimum and maximum values of data distributions.
RESULTS
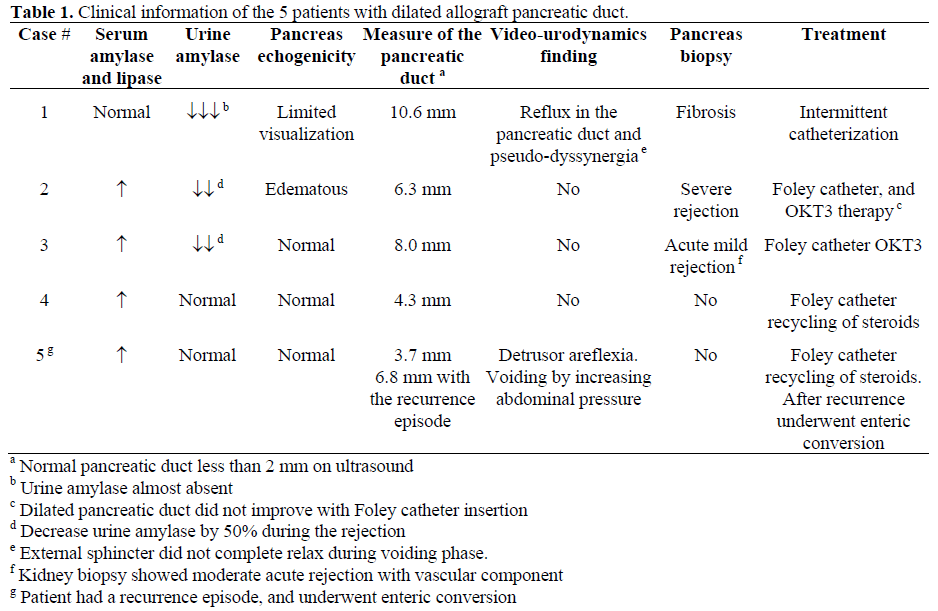
One hundred forty five patients underwent SPK transplants. Of these, 5 (3.4%) patients were identified with an US finding of dilated pancreatic duct postoperatively. There were 3 males and 2 females. One patient presented with normal serum amylase and lipase, and decreased urinary amylase and hyperglycemia. In this patient, pancreatic duct size improved with Foley catheter drainage but it remained 4 mm. However, a pancreas biopsy showed fibrosis. In the other four patients, the pancreatic duct size was improved to some degree by Foley catheter bladder decompression. These patients presented with elevation of serum amylase and lipase, which improved initially, but then required antirejection treatment (2 pancreas biopsy-proven, 2 empirically). This US finding was not seen in the other patients with rejection (our rejection rate is approximately 30%) or with reflux pancreatitis (1 out of 145 patients). The clinical course of the five patients is described in Table 1.
Case 1. A 38-year-old female underwent SPK. She lost kidney function due to an ischemic event (cortical necrosis by biopsy) and received a second kidney transplant (2 Dr match) 3 months later. Induction immunosuppression for the kidney included steroid bolus and recycling, and FK506 i.v. without antibody induction. She remained normoglycemic with normal serum and urine amylase. Six months later, after two kidney biopsy-proven acute rejection episodes, her creatinine was 1.4 mg/dl, but she was readmitted due to decreased urinary amylase (almost absent) and hyperglycemia for which she required insulin. US on admission demonstrated a dilated allograft pancreatic duct 10.3 mm (Figure 1). This improved with Foley catheter insertion. Video-urodynamics showed reflux into the pancreatic duct (Figure 2) and voiding in a not "relaxed manner" with evidence of pseudodyssynergia (Figure 3). Pancreas biopsy showed fibrosis without rejection. This patient requires insulin.
Figure 1. Ultrasound evaluation showed the pancreas
transplanted in the right iliac fossa. A tubular structure
was identified within the transplanted pancreas, which
likely represented a dilated pancreatic duct. This
structure measured 10.3 mm in transverse dimension.
Figure 2. During the video-urodynamics, the patient
was on supine position and monitored fluoroscopically.
The bladder was filled with dilute contrast.
Fluoroscopic control revealed a smooth walled bladder
during the filling phase with a closed bladder neck. The
patient experienced some reflux of urine into the
duodenum segment and into the pancreatic duct during
the height of the filling phase and especially during the
voiding phase.
Figure 3. Bladder compliance was normal during the
filling phase with detrusor pressures (Pdet) of less than
25 cm of H2O reached out of capacity of approximately
300 ml. Total intravesical pressure capacity was
approximately 40 cm of H2O. The patient had delayed
onset of sensation of fullness but very quickly had a
strong urge to void. During the voiding effort, a
detrusor contraction of 58 cm H2O was achieved and
sustained accompanied by a large amount of abdominal
straining and incomplete relaxation of the external
sphincter (EMG), possible evidence of pseudodyssynergia.
This patient did not void in a relaxed
manner. However, she did have adequate strength of
her detrusor contraction.
Case 2. A 39-year-old female underwent SPK and donor bone marrow infusion [12]. Eighteen months after the transplant, she was admitted with elevation of serum amylase and lipase and a decrease urine amylase (by 50%). US showed an edematous pancreas and dilated pancreatic duct (6.3 mm) which did not improve with Foley catheterization. Five days later, after no improvement in serum amylase and lipase, a pancreas biopsy was performed showing moderate to severe rejection with a vascular component. After finishing a 14 day course of OKT3 there was improvement of the serum and urine amylase and lipase and the pancreatic duct (without Foley catheter) measured 3 mm. She continues to be euglycemic off insulin.
Case 3. A 37-year-old male was admitted 6 weeks after SPK transplant with elevation of serum amylase/lipase and decrease in urine amylase (by 50%). The US showed a dilated pancreatic duct (8 mm). Twenty-four hours after insertion of Foley catheter, repeated US demonstrated a normal duct. However, after 5 days the serum amylase/lipase remained elevated and a pancreas biopsy was performed which showed acute rejection. By the end of a 14-day course of OKT3, the serum amylase/lipase and urine amylase normalized. This patient remains euglycemic, off insulin.
Case 4. One month after SPK transplant, a 40-year old male was admitted with elevation of serum amylase/lipase and normal urine amylase. The US demonstrated a dilated pancreatic duct (4.3 mm). A Foley catheter was inserted, and at the same time he was treated empirically for rejection with a 4-day course of methylprednisolone. Repeat US showed normal size pancreatic duct. The Foley catheter was left in place for about 7 days. Repeat US after removal of the catheter still showed normal size pancreatic duct. The patient remains euglycemic, off insulin.
Case 5. This case (a 41-year old male) is similar to case 4 with the only difference that the pancreatic duct measured 3.7 mm before the insertion of a Foley catheter. He was empirically treated for rejection (elevation of serum amylase/lipase and normal urine amylase) with improvement of the duct size (repeat US) after anti-rejection treatment. Six months after this event, he developed a recurrence. This time the US showed a duct size of 6.8 mm. A videourodynamic study showed detrusor areflexia, he attempted to void by increasing abdominal pressure but no detrusor activity was noted with the voiding effort. The video phase of this study showed reflux into the duodenum at very low bladder pressures (<5 cm H2O). Although he was offered intermittent catheterization, he preferred and underwent conversion from bladder to enteric drainage successfully. This patient remains euglycemic, off insulin. Patients (4/5) have been followed for a median of 46.5 months (range 45 to 63) without further recurrence.
DISCUSSION
Complications after pancreatic transplantation with pancreatic exocrine bladder drainage via a PDC include primary nonfunction due to preservation injury, rejection, anastomotic leak, arterial and/or venous thrombosis, and infection [9, 13, 14, 15]. Radiologic imaging plays an important role in the evaluation of pancreas transplantation.
The US demonstration of allograft pancreatic duct dilatation has not been well described or defined previously. Mjörnstedt et al. [16] reported pronounced dilatation of the pancreatic duct secondary to distal obstruction in a patient who received a segmental pancreatic graft. Dilatation of the duct has also been reported in a few cases of pancreatic rejection [17].
A mechanical obstruction (e.g. pancreatic stone, inadvertent suture) or reflux pancreatitis may cause dilatation of the transplant pancreatic duct. Reflux pancreatitis is typically characterized by: 1) sudden onset of lower abdominal pain located over the pancreatic graft; 2) elevation of serum amylase in the absence of leak; 3) edema of the pancreas, without abscess or fluid collection on computed tomography scan; and 4) resolution of the symptoms within 24 hours after placement of a Foley catheter [18]. Pancreatitis is thought to be chemically induced by reflux of urine through the sphincter of Oddi into the pancreatic duct during the voiding phase of the bladder with high detrusor pressure [15]. Others have hypothesized that this could be caused by an incompetent sphincter of Oddi [19] or by pressure exerted on the pancreatic duct due to a large volume bladder, or micturition narrowing the duodenocystostomy and obstructing it [20]. Asymptomatic reflux pancreatitis with high or normal detrusor pressure, incompetent sphincter of Oddi or external sphincterdetrusor- dyssynergia could have caused the dilatation of the pancreatic duct in Case 1.
Could pancreatic duct dilatation be associated with pancreas rejection? Four patients presented with elevation of serum amylase and without abdominal pain. Edema of the pancreas was seen in only one patient (Case 2), 3 patients had normal echogenic pancreas (Case 3-5), and in one the visualization was limited. Two patients had biopsy-proven allograft pancreas rejection, and the other two patients (empirically treated) in the absence of other abnormal findings rejection might have been possible. After anti-rejection treatment, there was US improvement in the size of the pancreatic duct (Foley catheter was already removed), with the exception of Case 3 who had improvement of the duct size 24 hr after Foley insertion. All four patients with rejection had a normal voiding pattern and normal VCUG (no suspicion of neurogenic bladder). Urodynamic studies were not obtained (except case 5 who developed recurrence). One could speculate that pancreas rejection could be associated with a certain degree of pancreatic duct dilatation in the absence of other pathology causing duct dilatation.
Duodenal biopsy was not performed in any of the cases. However, duodenal rejection (with or without pancreas rejection) associated with inflammation and swelling of the ampulla may have caused: 1) obstruction that resulted in dilatation of the pancreatic duct, or 2) relaxation of sphincter, allowing free reflux in the pancreatic duct.
Only case 5 had recurrence of this phenomenon six months after the Foley catheter had been removed. A videourodynamic study was obtained during the second event, which demonstrated detrusor areflexia. He was voiding by increasing abdominal pressure but without detrusor activity. This abnormal voiding pattern was creating high intravesical pressures resulting in an incompetent sphincter of Oddi and dilatation of the pancreatic duct. He underwent enteric conversion [21]. The other treatment option for this type of neurogenic bladder is intermittent catheterization. The patient with pseudodyssynergia lost the pancreas allograft function (pancreas biopsy-proven fibrosis without rejection). The clinical presentation was different from those patients with rejection. There was no elevation of serum amylase, but rather decreased urinary amylase and insulin requirement. The loss of the allograft function in this patient was probably induced by chronic reflux of urine through the sphincter of Oddi into the pancreatic duct during voiding phase. The pancreas US and video-urodynamics showed dilated duct and reflux into the duct respectively. Interestingly, the patient was asymptomatic and did not experience pain related to reflux. Intermittent catheterization without voiding and bladder training as suggested by videourodynamic study or early conversion to enteric drainage may have prevented graft loss.
In conclusion, allograft pancreatic duct dilatation is uncommon in SPK transplant with PDC. Management of the duct dilatation with Foley catheter drainage, repeat serum and urinary amylase, US, pancreas biopsy, and selective urodynamic study can help to determine the possible etiology of this US finding. Following this approach, pancreas loss can be minimized. Although this finding is likely secondary to outlet obstruction, Foley decompression alone may not be sufficient treatment (enteric conversion may ultimately be necessary) and rejection of the pancreas allograft should also be considered.
References
- Sutherland D, Gruessner A, Moudry-Munns K. International pancreas transplant registry report. Transplant Proc 1994; 26:407-11. [AN 94225380]
- Sollinger HW, Knechtle SJ, Reed A, D'Alessandro AM, Kalayoglu M, Belzer FO, Pirsch J. Experience with 100 consecutive simultaneous kidney-pancreas transplant with bladder drainage. Ann Surg 1991; 214:703-11. [AN 92074851]
- Maile CW, Crass JR, Frick, MP, Feinberg SB, Goldberg ME, Sutherland DE. CT of pancreas transplantation. Invest Radiol 1985; 20:609-12. [AN 86058493]
- Letourneau JG, Maile CW, Sutherland DE, Feinberg SB. Ultrasound and computed tomography in the evaluation of pancreatic transplantation. RadiolClin North Am 1987; 25:345-355. [AN 87147911]
- Patel B, Markivee CR, Mahanta B, Vas W, George E, Garvin P. Pancreatic transplantation: Scintigraphy, US, and CT. Radiology 1988; 167:685-7. [AN 88204150]
- Milner LN, Ramos IM, Marks WH, Taylor KJ. Ultrasound imaging of pancreatico-duodenal transplants. J ClinGastroenterol 1991; 13:570-574. [AN 92078598]
- Krebs T, Daly B, Wong J, Barlett S. The magnetic resonance-derived pancreas to psoas ratio (PPR): objective and reliable noninvasive diagnosis of pancreatic rejection. Transplant Proc 1995; 27:3034. [AN 96125410]
- Yuh WT, Wiese JA, Abu-Yousef MM, Rezai K, Sato Y, Berbaum KS, et al. Pancreatic transplant imaging. Radiology 1988; 167:679-83. [AN 88204149]
- Ciancio G, Burke GW, Viciana AL, Ruiz P, Ginzburg E, Dowdy L, et al. Destructive allograft fungal arteritis following simultaneous pancreaskidneytransplantation. Transplantation 1996; 61:172-5. [AN 96195474]
- Burke GW, Alejandro R, Ciancio G, Nery J, Roth D, Shapiro R, et al. The use of FK506 in simultaneouspancreas/kidney transplantation: rescue, induction, and maintenance immunosuppression. Transplant Proc1995; 27:3123-4. [AN 96125455]
- Burke GW, Ciancio G, Alejandro R, Roth D, Ricordi C, Tzakis A, Miller J. Use of tacrolimus and mycophenolatemofetil for pancreas-kidney transplantation with or without OKT3 induction. Transplant Proc 1998; 30:1544-5. [AN 98300256]
- Burke GW, Ricordi C, Karatzas T, Carreno M, Markou M, Cirocco R, et al. Donor bone marrow infusion in simultaneous pancreas/kidney transplantation with OKT3 induction: Evidence for augmentation of chimerism. Transplant Proc 1997; 29:1207-8. [AN 97232781]
- Ciancio G, Burke GW, Nery JR, Coker D, Miller J. Urethritis/dysuria after simultaneous pancreas-kidney transplantation. Clin Transplant 1996; 10:67-70. [AN 96252065]
- Ciancio G, Burke GW, Nery J, Siquijor A, Coker D, Roth D, Miller J. Urological complications following simultaneous pancreas-kidney transplantation. Transplant Proc 1995; 27:3125-6. [AN 96125456]
- Ciancio G, Burke GW, Roth D, Luque C, Coker D,Miller J. Reflux pancreatitis after simultaneouspancreas-kidney transplantation treated by alpha1 blocker. Transplantation 1995; 60:760-1. [AN 96029816]
- Mjörnstedt L, Geterud K, Olausson M. Occlusion of the pancreatic duct: A case of impaired pancreas graft function. Transplant Proc 1992; 24:350-1. [AN 92169862]
- Batiuk TD, Carpenter HA, Morton MJ, Brown ML, Engen DE, Velosa JA. Correlation of pancreas allograft biopsy with radionuclide and ultrasound imaging of pancreas allografts. Transplant Proc 1991; 23:1606-7. [AN 91111695]
- Sollinger HW, Messing EM, Eckhoff DE, PirschJD, D'Alessandro AM,Kalayoglu M, et al. Urological complications in 210 consecutive simultaneous pancreas-kidney transplants with bladder drainage. Ann Surg 1993; 218:561-8. [AN 94029228]
- Stephanian E, Gruessner RW, Brayman KL, Gores P, Dunn DL, Najarian JS, Sutherland DE. Conversion of exocrine secretions from the bladder to enteric drainage in recipients of whole pancreaticoduodenaltransplants. Ann Surg 1992; 216:663-72. [AN 93103316]
- Boudreaux JP,Nealon WH, Carson RC, Fish JC. Pancreatitis necessitating urinary undiversion in abladder-drained pancreas transplant. Transplant Proc1990; 22:641-2. [AN 90223745]
- Burke GW, Gruessner R, Dunn DL, Sutherland DE. Conversion of whole pancreaticoduodenaltransplants from the bladder to enteric drainage for metabolic acidosis or dysuria. Transplant Proc 1990; 22:651-2. [AN 90223750]




