Keywords
Laparoscopy; Multiple Endocrine Neoplasia Type 1; Pancreatectomy
Abbreviations
HbA1c: hemoglobin A1c; MEN-1: multiple endocrine neoplasia type 1; PP: pancreatic polypeptide
INTRODUCTION
Multiple endocrine neoplasia type 1 (MEN-1) is an autosomal dominant syndrome characterized by functioning or nonfunctioning tumors of the parathyroid glands, anterior pituitary gland, and the pancreatic islet cells or duodenum. MEN-1 results from a mutation of the MEN-1 tumor-suppressor gene located on chromosome 11q13 encoding the MENIN protein [1]. Over 600 different germline mutations have been found to cause MEN-1, which occurs in an estimated 1 in 30,000 people, with equal incidence in males and females [2].
Hyperparathyroidism is the most common manifestation of MEN-1 found in 95% of patients by 40 years of age [3, 4, 5, 6, 7]. Endocrine tumors of the pancreas or duodenum are the second most common manifestation affecting up to 75% of patients [8, 9, 10, 11]. Approximately 30% of patients develop pituitary adenomas, most commonly prolactinoma [8]. Less common manifestations include adrenal tumors, thymic and bronchial carcinoids, lipomas, angiofibromas, thyroid neoplasms, pheochromocytoma, melanoma, and teratomas [8, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21]. Pancreatic endocrine tumors may be functional or nonfunctional. Of all pancreatic endocrine tumors twothirds are functional but in patients with MEN-1 most are nonfunctional. Among MEN-1 patients with functioning pancreatic endocrine tumors, gastrinoma is the most commonly observed malignant tumor (20- 70%) [8, 22, 23, 24]. Patients with pancreatic endocrine tumors present with a wide range of gastrointestinal symptoms or they may be asymptomatic with pancreatoduodenal tumors discovered incidentally on imaging or during workup of known or suspected MEN syndrome. Early detection of functional pancreatic endocrine tumors through biochemical screening is important to ameliorate the development of clinical symptoms. Annual biochemical surveillance is recommended including serum calcium, PTH, glucose, gastrin, insulin, proinsulin, chromogranin A, pancreatic polypeptide, vasoactive intestinal polypeptide, glucagon, prolactin, and IGF-1 [4, 5, 7, 15].
Imaging modalities used to identify functional or nonfunctional pancreatic endocrine tumors include computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography, somatostatin receptor scintigraphy, and endoscopic or intraoperative ultrasound [25]. The frequently multifocal nature, small size, and similarity to pancreatic tissue of pancreatic endocrine tumors in MEN patients make accurate assessment of tumor burden difficult. EUS and intraoperative ultrasound are thought particularly useful for identifying small tumors, but are known to be operator dependent.
Surgical options for treatment of pancreatic endocrine tumors include simple enucleation, partial pancreatectomy (distal, central, subtotal, or near-total pancreatectomy), pancreaticoduodenectomy, total pancreatectomy, and the Thompson procedure (distal to subtotal pancreatectomy, enucleation of pancreatic head tumors, peripancreatic lymph node dissection, duodenal exploration with tumor excision for patients with gastrinoma, and cholecystectomy) [23]. The degree of tumor resection is determined by weighing the risks of malignant transformation or tumor recurrence against the risks of pancreatic gland removal with subsequent development of endocrine or exocrine insufficiency [23]. Surgical decision making is complicated by the fact that these tumors are frequently multifocal and distributed throughout the pancreatic parenchyma. In addition, the potential for malignant transformation of pancreatic endocrine tumors in this subgroup is difficult to predict. Surgical and autopsy series have demonstrated pre-neoplastic changes distributed throughout the pancreas in affected patients, limiting chances of cure with partial resection alone [26, 27].
We present our experience at a tertiary referral center for patients with MEN-1 and pancreatic endocrine tumors over the course of a 2-year time period. Sensitivity of preoperative imaging studies, extent of resection, and number of pancreatic endocrine tumors found in the specimen were specifically addressed.
METHODS
A retrospective chart review of a prospectively maintained pancreatic surgery database was conducted for patients with MEN-1 and pancreatic endocrine tumors treated from December 2008 to May 2011 at the Mayo Clinic Jacksonville, FL, USA. All patients met accepted criteria for diagnosis of MEN-1 [28]. Standard clinicopathologic parameters were analyzed including presence of symptoms, functionality of tumors determined by laboratory analysis, radiographic findings, surgical procedure, final pathology including number of tumors found, involved lymph nodes, and tumor size, postoperative complications, and morbidity at follow up. Surgical resection was guided by anticipated location of tumor(s) based on preoperative imaging. All patients underwent laparoscopic resection.
The development of post-operative endocrine and exocrine insufficiency requiring insulin and/or enzyme supplementation is also described.
Preoperative Workup
Patients with known or suspected MEN-1 underwent biochemical and radiographic testing to determine presence and functionality of pancreatic tumors as well as determine extent of disease. Biochemical testing for pancreatic endocrine tumors was conducted after diagnosis of MEN-1 and consisted of serum gastrin, baseline glucose, insulin, proinsulin, chromogranin A, pancreatic polypeptide, vasoactive intestinal polypeptide, glucagon, prolactin, and IGF-1. Radiographic testing consisted of MRI and EUS to delineate location and extent of pancreatic involvement for surgical planning. Additional radiologic testing with CT or somatostatin receptor scintigraphy was left to the discretion of the referring physician. All patients were referred preoperatively for nutritional assessment and for diabetes education. Post-splenectomy vaccines were administered 2 weeks before operation.
Postoperative Care
At the conclusion of the procedure, a jejunostomy tube was placed and maintained for 4-8 weeks postoperative, with the decision to remove the feeding tube based on nutritional status at follow up. Postoperative, patients are placed on an insulin drip and enzyme supplementation is initiated with diet advancement or initiation of enteral feeding. Exocrine insufficiency is assessed by the number of bowel movements per day and overall nutritional status, with changes to enzyme supplementation made as needed.
ETHICS
This study was approved by the Mayo Clinic Institutional Review Board. Written consent was obtained from each patient. This study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects.”
STATISTICS
Descriptive statistics only were computed: mean, median, range and frequency.
RESULTS
Four patients were identified to have MEN-1 and pancreatic endocrine tumors requiring pancreatic resection over a 2-year time period. Preoperative characteristics, imaging findings, operation performed, and pathology results are listed in Table 1. Ages of our patients were 29, 35, 37, and 42 years. Gastrointestinal symptoms were present in 1 of 4 patients. All patients were previously diagnosed with pituitary adenoma, 1 patient additionally had a history of gastrinoma and gastric carcinoid. Preoperative imaging with MRI and EUS showed a median of 1 and 5 tumors, respectively.
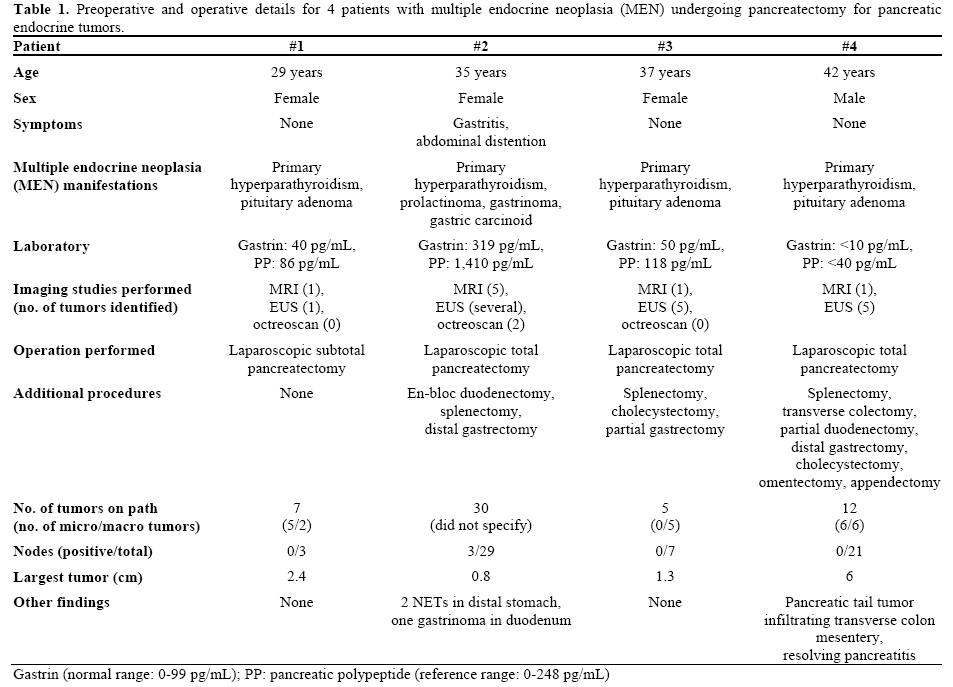
Octreoscan was performed in 3 patients, identifying 2 pancreatic endocrine tumors in a single patient. Three patients underwent laparoscopic total pancreatectomy and 1 patient underwent laparoscopic subtotal pancreatectomy for predominantly distal pancreatic disease. Additional procedures as required are listed in Table 1. A mean of 13.5 tumors were found on final pathology (range: 5 to 30), with an average size of 2.6 cm (range: 0.8 to 6 cm). Only one patient had lymph node positive disease with median 14 lymph nodes analyzed for the group.
The operative time for laparoscopic subtotal pancreatectomy was 200 minutes with an estimated blood loss of less than 100 mL. Mean operative time for laparoscopic total pancreatectomy was 567 minutes, with a mean estimated blood loss of 267 mL. Postoperative blood transfusion of 2 units was required in a single patient after total pancreatectomy.
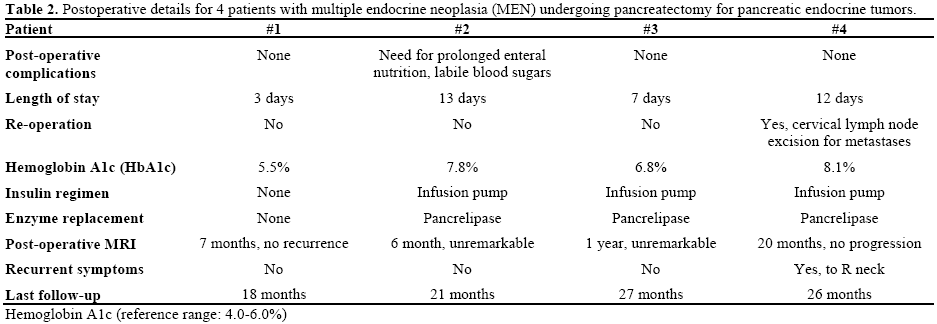
Postoperative complications, development of endocrine/ exocrine insufficiency, and state of disease at last follow up are listed in Table 2. Average length of hospitalization was 8.7 days (range: 3 to 13). One patient developed prolonged ileus postoperatively requiring discharge home with jejunostomy tube feeds. One patient required reoperation 6 months later for biopsy-proven metastatic neuroendocrine tumor to cervical chain lymph nodes. No patients required reoperation for recurrent abdominal disease or due to postoperative complication. All patients who had total pancreatectomy required an insulin pump for glucose management as well as pancreatic enzyme supplementation. Metastatic disease was identified in a single patient with no mortalities observed at last follow up (range: 18 to 27 months).
DISCUSSION
Most patients with MEN-1 develop endocrine tumors of the pancreas or duodenum. Unique to the pancreatic involvement of pancreatic endocrine tumors in this population is their diffuse nature and predisposition towards multifocal disease [8]. Gauger et al. and Kouvaraki et al. examined 49 and 38 patients with MEN-1 and pancreatic endocrine tumors finding multiple pancreatic endocrine tumors in 100% and 71% of patients, respectively [11, 23]. There is no clear evidence delineating the timeline or risk of malignant transformation of small pancreatic endocrine tumors in these patients, therefore the proper timing and extent of resection remains controversial.
The most important cause of death in patients affected with MEN-1 is malignant transformation of pancreatic endocrine tumors [4, 5]. Gauger et al. found that 46% of patients in this group died as a result of their pancreatic neoplasm(s) [23]. A second group identified a median survival of 19.5 years after treatment for pancreatic endocrine tumors, noting a better survival in patients with functioning tumors, no metastatic disease, and after complete surgical resection [11]. In patients with advanced pancreatic endocrine tumors, 50-80% died within 5 years of tumor progression [29, 30]. Higher morbidity was noted in patients with nonfunctional pancreatic endocrine tumors due to the development of locally advanced or metastatic tumors coupled with more difficult reoperative procedures when performed [31]. It is known that the majority of disease-related complications and death in MEN-1 gene mutation carriers relates to malignant duodenopancreatic and intrathoracic tumors (bronchial and thymic carcinoids) [32, 33]. Metastatic potential in functional pancreatic endocrine tumors (gastrinomas) has been shown to correlate with size of tumor and is the basis for the practice of early surgical excision of functional pancreatic endocrine tumors in these patients [34]. An estimated 1/3 of patients with pancreatic endocrine tumors have metastases at initial presentation [35]. The presence of lymph node involvement and metastases to the liver are known to be major factors limiting survival [36]. Lymph node metastases have been found with increased frequency in patients with tumors greater than 3 cm, but no correlation has been shown between the size of the primary pancreatic endocrine tumor and incidence of metastases [8, 37]. The development of liver metastases has been found to occur in up to 50% of patients with malignant pancreatic endocrine tumors and is a significant cause of morbidity and mortality [32, 38, 39, 40]. Pancreatic endocrine tumors larger than 3 cm have also been shown to have a higher prevalence of malignancy.
Current imaging modalities have specific limitations in their ability to detect small, multifocal pancreatic endocrine tumors characteristic of the MEN syndromes [41]. CT and somatostatin receptor scintigraphy have been shown to identify 59-69% of pancreatic endocrine tumors, but are known to underestimate overall tumor burden when compared to the number of tumors found at operation [8]. The sensitivity of MRI in detecting pancreatic endocrine tumors has ranged from 75 to 85% with a recent study by Caramella et al. finding 95% sensitivity for detecting these tumors, though this high sensitivity may represent selection bias [42, 43, 44]. Endoscopic ultrasound is particularly sensitive at early detection of pancreatic endocrine tumors in patients with MEN (70-90%), revealing lesions as small as 5 mm [45, 46, 47]. In our cohort, when compared to findings at pathology, preoperative imaging studies identified only macrotumors (greater than 0.5 cm), with size limitation alone the most likely explanation for lack of identification of microtumors. Additionally, none of the “occult” lesions identified at pathology had more malignant characteristics than the index lesion or lesions. Intraoperative ultrasonography has also been shown highly sensitive in identifying pancreatic endocrine tumors (up to 83%) with the ability to identify tumors as small as 3 mm [3]. Although highly sensitive at detection, this method is notably operator dependent [3]. Our group utilizes intraoperative ultrasonography both for open and laparoscopic cases, finding high resolution imaging helpful at determining the required degree of pancreatic resection, ability to achieve adequate margins, and define the relationship to adjacent structures. Subjectively we note no difference in the ability to identify macro- or micro-tumors when ultrasound is performed laparoscopically compared to open. Despite advanced imaging techniques, tumor burden in patients with MEN and multifocal disease remains underestimated [8, 41].
Management strategies for pancreatic endocrine tumors in patients with MEN-1 are aimed at early detection and resection before metastatic spread. Considerable controversy exists relating to the timing of metastatic spread or development of recurrence [11]. Conservative management has been proposed for small, asymptomatic nonfunctional pancreatic endocrine tumors, emphasizing the low risk of death from islet cell tumors of the pancreas (15%), the significant morbidity of pancreatic surgery, and the inability to prevent new tumor development unless total pancreatectomy is performed [8, 32, 33, 38, 48, 49, 50, 51]. A different recommended strategy emphasizes early resection when the diagnosis of pancreatic endocrine tumors are made whether via imaging or laboratory analysis (i.e., elevated pancreatic polypeptide) to prevent the risk of malignant transformation [10, 38, 52, 53, 54, 55]. An even more aggressive approach recommends early surgical exploration with resection based on suggestive biochemical analysis alone, even before tumors are detected on imaging [56, 57, 58, 59]. Our current practice shadows that of Lairmore et al. who recommends resection of any functional pancreatic endocrine tumor at diagnosis or of any nonfunctional pancreatic endocrine tumor larger than 1 cm [8]. Cure rates are unfortunately low secondary to the diffuse nature of pancreatic involvement in these patients coupled with high rates of recurrence, even if complete resection is performed [11, 23]. Gauger et al. examined 49 patients with MEN-1 with recurrent pancreatic endocrine tumors after Thompson procedure, noting a need of 8/49 (16%) for completion pancreatectomy and duodenectomy [23]. Despite complete resection, recurrence has been seen in up to 30% of patients as far as 8 years after operation [11].
Modern pancreatic enzyme supplementation and improved diabetes education and insulin administration via infusion pumps has decreased the overall morbidity associated with total pancreatectomy [42]. At our institution, a team approach is ensured through a clinical pathway for patients undergoing total pancreatectomy. We emphasize preoperative diabetes education and provide a diabetic counselor to answer questions and design an insulin regimen while the patient is hospitalized to improve compliance and glucose control in the outpatient setting. Our pathway also includes preoperative nutritional assessment and nutritional support that continues during hospitalization with pancreatic enzyme supplementation and a multivitamin with frequent assessment of nutritional intake upon discharge. A feeding jejunostomy is placed and kept for 4-8 weeks postoperatively at which time a nutritional assessment is performed with the decision to remove the feeding tube based on whether a patient is meeting adequate caloric needs. In our experience, even if not used, the jejunostomy serves as a safety net for those patients having difficulty maintaining adequate nutrition. Thus far, our pathway has helped to decrease re-hospitalization rates and reduce the morbidity associated with the metabolic derangements expected after total pancreatectomy.
By decreasing the severity of metabolic derangements associated with total pancreatectomy and improving patient compliance and comfort with supplementation and insulin administration, we believe the utility of total pancreatectomy for multifocal pancreatic endocrine tumors in patients with MEN-1 may be worth revisiting. The laparoscopic approach is safe in experience hands and may be the preferred route for selected patients. This approach may be associated with faster recovery times and less postoperative complications when compared to open total pancreatectomy.
The use of laparoscopy may also cut down on the historic morbidity of total pancreatectomy. We believe for some patients, the laparoscopic approach may be preferred to the more traditional operation in the hands of a skilled laparoscopist, decreasing hospitalization, patient discomfort, and minimizing postoperative complications. Our group has also shown improved lymph node harvest during laparoscopic compared to open pancreatic resections, analyzing a 5-year experience comparing pancreaticoduodenectomy/total pancreatectomy and distal pancreatectomy for adenocarcinoma [60]. This analysis demonstrated a statistically significant increase in mean number of lymph nodes analyzed via the laparoscopic approach (23.8 vs. 14.7 for pancreaticoduodenectomy/total pancreatectomy, and 26.3 vs. 11.8 for distal pancreatectomy) [60]. Compared to patients who have partial pancreatic resection for pancreatic endocrine tumors, total pancreatectomy will further minimize the risk of local recurrence and the need for lifelong screening via MRI or EUS.
Our study has several important limitations. The retrospective nature of the review and lack of a control group allows inherent bias. We detail a single center, single surgeon experience with a preference for laparoscopic surgery, leaving no comparison to total pancreatectomy performed open. The small number of patients included in our series is a significant limitation but mirrors the relative paucity of patients in the general population with MEN-1.
CONCLUSION
In patients with MEN-1 and multifocal pancreatic endocrine tumors, current imaging modalities may underestimate overall tumor burden. Total pancreatectomy may be considered as a drastic but potentially curative measure in these patients. With the help of modern insulin monitoring and delivery systems, enzyme supplementations, and a minimal access surgical technique, the morbidity of a total pancreatectomy may have significantly decreased over the past few years to the point where this may become a preferred treatment for this rare disease.
Acknowledgment
Kelly Rapier, ARNP
Disclosures
The authors report no potential conflicts of interest
References
- Chandrasekharappa S, Guru S, Manickamp P, et al. Positional cloning of the gene for multiple endocrine neoplasia type 1. Science 1997;276:404-407.
- Guo S, Sawicki M. Molecular and genetic mechanisms of tumorigenesis in multiple endocrine neoplasia type 1. MolEndocrin 2001;15(10):1653-1664.
- Kang C, Park S, Kim K, Choi J, et al. Surgical experiences of functioning neuroendocrine neoplasm of the pancreas. Yonsei Medial Journal 2006;47(6):833-839.
- Skogseid B, Eriksson B, Lundqvist G, et al. Multiple endocrine neoplasia type 1: a 10 year prospective screening study in four kindreds. J Clin Endocrinol Metab 1991;73:281-287.
- Skogseid B, Rashad J, Akerstrom G. Pancreatic endocrine tumors in multiple endocrine neoplasia type 1. In: Doherty GM, Skogseid B, editors. Surgical endocrinology. Philadelphia: Lippincott Williams and Wilkins; 2001. p 511-524.
- Lairmore T, Piersall L, DeBenedetti M, et al. Clinical genetic testing and early surgical intervention in patients with multiple endocrine neoplasia type 1 (MEN 1 ). Ann Surg 2004;239;637-645.
- Brandi M, Gagel R, Angelli A, et al. Guidelines for diagnosis and therapy of MEN type 1 and 2. J Clin Endocrin Metab 2001;86:5658-5671.
- Lairmore T, Chen V, DeBenedetti M, Gillanders W, et al. Duodenopancreatic Resections in Patients with Multiple Endocrine Neoplasia Type 1. Annals of Surgery 2000; 231 (6): 909-918.
- Vasen H, Lamers C, Lips C. Screening for the multiple endocrine neoplasia syndrome type 1: a study of 11 kindreds in The Netherlands. Arch Int Med. 1989;149:2717-2722.
- Skogseid B, Eriksson B, Lundqvist G, et al. Multiple endocrine neoplasia type 1: a 10 year prospective screening study in four kindreds. J Clin Endocrin Metab 1991;73:281-287.
- Kouvaraki M, Shapiro S, Cote G, et al. Management of pancreatic endocrine tumors in multiple endocrine neoplasia type 1. World J Surg 2006; 30: 643-653.
- Ballard FB, Hartstock RJ. Familial endocrine adenoma-peptic ulcer complex. Medicine (Baltimore) 1964; 43:481-516.
- Gibril F, Chen Y, Schrump D, et al. Prospective study of thymic carcinoids in patients with multiple endocrine neoplasia type 1. J Clin Endocrin Metab 2003;88(3):1066-1081.
- Marx S, Spiegel A, Skarulis M, et al. Multiple endocrine neoplasia type 1: clinical and genetic topics. Ann Intern Med 1998;129(6):484-494.
- Brandi M, Gagel R, AngeliA et al. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrin Metab 2001;86(12):5658-5671.
- Burgess J, Greenaway T, Shepherd J. Expression of the MEN-1 gene in a large kindred with multiple endocrine neoplasia type 1. J Inten Med 1998;243(6):465-470.
- Darling T, Skarulis M, Steinberg S, et al. Multiple facial angiofibromas and collagenomas in patients with multiple endocrine neoplasia type 1. Arch Dermat 1997;133(7)853-857.
- Duh Q, Hybarger C, Geist R, et al. Carcinoids associated with multiple endocrine neoplasia syndromes. Am J Surg 1987;154(1):142-148.
- Metz D. Multiple endocrine neoplasia type 1. SeminGastrointest Dis 1995;6(2):56-66.
- Trump D, Farren B, Wooding C, et al. Clinical studies of multiple endocrine neoplasia type 1. Q J Med 1996;89:653-669.
- Schussheim D, Skarulis M, Agarwal S, et al. Multiple endocrine neoplasia type 1: new clinical and basic findings. Trends Endocrinol Metab 2001;12:173-178.
- Jensen R. Pancreatic endocrine tumors: recent advances. Ann Oncol 1999;10:170-176.
- Gauger P, Doherty G, Broome J, et al. Completion pancreatectomy and duodenectomy for recurrent MEN-1 pancreaticoduodenal endocrine neoplasms. Surgery 2009; 146(4): 801-808.
- Waldman J, Fendrich V, Habbe N, Bartsch D, et al. Screening of patients with multiple endocrine neoplasia type 1: A critical analysis of its value. World J Surg 2009;33:1208-1218.
- Dralle H, Krohn S, Karges W, Boehm B, et al. Surgery of resectable nonfunctioning neuroendocrine pancreatic tumors. World J Surg 2004;28:1248-1260.
- Majewski J, Wilson D. The MEN1 syndrome: an all or none phenomenon? Surgery 1979; 86:475-484.
- Thompson N, Lloyd R, Nishiyama R, et al. MEN 1 pancreas: a histological and immunohistochemical study. World J Surg 1984;8:561-574
- Marini F, Falchetti A, Luzi E, et al. Multiple Endocrine Neoplasia Type 1 (MEN1) Syndrome. [July 18, 2008 [updated [August 9, 2008]. In: Riegert-Johnson DL, Boardman LA, Hefferon T, Roberts M, eds. Cancer Syndromes (Internet). Bethesda (MD): National Center for Biotechnology Information ; 2009.
- Mignon M. Natural history of neuroendocrine enteropancreatic tumors. Digestion 2000;62:51-58.
- Jensen R. Natural history of digestive endocrine tumors. In: Mignon M, Colombel J, eds. Recent advances in pathophysiology and management of inflammatory bowel disease and digestive endocrine tumors. Paris, France: John LibbeyEurotext Publishing Co;1999:192-219.
- Norton J. Neuroendocrine tumors of the pancreas and duodenum. CurrProbSurg 1994;31:71-156.
- Wilkinson S, The B, Davey K, et al. Cause of death in multiple endocrine neoplasia type 1. Arch Surg 1993; 128: 683.
- Doherty G, Olson J, Frisella M, et al. Lethality of multiple endocrine neoplasia type 1. World J Surg 1997; 22: 581-586.
- Weber HC, Venzon DJ, Lin JT, Fishbein VA, Orbuch M, Strader DB, et al. Determinants of metastatic rate and survival in patients with Zollinger-Ellison syndrome: a prospective long-term study. Gastroenterology 1995; 108:1637-49. [PMID 7768367]
- Solica E, Kloeppel G, Sobin L. World Health Organization: International Histological Classification of Tumours: Histological Typing of Endocrine Tumors. Berlin: Springer, 2000.
- Weber H, Venzon D, Lin J, et al. Determinant of metastatic rate and survival in patients with Zollinger-Ellison syndrome: a prospective long-term study. Gastroenterology. 1995;108:1637-1649.
- Lowney J, Frisella M, Lairmore T, Doherty G. Pancreatic islet cell tumor metastasis in multiple endocrine neoplasia type 1: correlation with primary tumor size. Surgery 1998; 124: 1043-1049.
- Dean P, van Heerden J, Farley D, et al. Are patients with multiple endocrine neoplasia type 1 prone to premature death? World J Surg 2000;24:1437-1441.
- Ruszniewski P, Podevin P, Cadiot G, et al. Clinical, anatomic, and evolutive features of patients with the Zollinger-Ellison syndrome combined with type 1 multiple endocrine neoplasia. Pancreas 1993;8:295-304.
- Norton J, Alexander H, Fraker D, et al. Comparison of surgical results in patient with advanced and limited disease with multiple endocrine neoplasia type 1 and Zollinger-Ellison syndrome. Ann Surg 2001;234:495-505.
- Doppman J. Multiple endocrine neoplasia syndromes. A nightmare for the endocrinologic radiologist. SemRoentgenol 1985; 20: 7-16.
- Stauffer JA, Nguyen J, Heckman M, Grewal M, et al. Patient outcomes after total pancreatectomy: a single centre contemporary experience. HPB 2009;11(6):483-492.
- Ichikawa T, Peterson MS, Federle MP et al. Islet cell tumor of the pancreas: biphasic CT versus MR imaging in tumor detection. Radiology 2000; 216:163-171.
- Thoeni RF, Mueller-Lisse UG, Chan R, Do NK, Shyn PB Detection of small, functional islet cell tumors in the pancreas: selection of MR imaging sequences for optimal sensitivity. Radiology 2000; 214:483-490.
- Botsios D, Vasliliadis K, Tsalis K, Iordanidis F, et al. Management of nonfunctioning pancreatic endocrine tumors in the context of multiple endocrine neoplasia type 1 syndrome. J Gastrointestin Liver Dis 2007;16(3):257-262.
- Zimmer T, Stolzel U, Bader M, et al. Endoscopic ultrasonography and somatostain receptor scintigraphy in preoperative localization of insulinomas and gastrinomas. Gut 1996;39:562-568.
- Proye C, Malvaux P, Pattou F, et al. Noninvasive imaging of insulinomas and gastrinomas with endoscopic ultrasonography and somatostatin receptor scintigraphy. Surgery 1998;124:1134-1143.
- Mutch M, Frisella M, DeBenedetti M, et al. Pancreatic polpeptide is a useful plasma marker for radiographically evident pancreatic islet cell tumors in patients with multiple endocrine neoplasia type 1. Surgery 1997;122:1012-1019.
- Goudet P, Calendar A, Cougard P, et al. Multiple endocrine neoplasia type 1 r Werner syndrome: what is important to know about surgery of a rare disease. Ann Chir 2002;127:591-599.
- GTE. Recommendation booklet on MEN1. 2004.
- Doherty G. Multiple endocrine neoplasia type 1: duodenopancreatic tumors. Surg Oncol 2003;12:135-143.
- Akerstrom G, Hessman O, Skogseid B. Timing and extent of surgery in symptomatic and asymptomatic neuroendocrine tumors of the pancreas in MEN1. Langenbecks’ Arch Surg 2002;386:558-569.
- Doherty G, Thompson N. Multiple endocrine neoplasia type 1: duodenopancreatic tumors. J Intern Med 2003;253:590-598.
- Dralle H, Krohn S, Karges W, et al. Surgery of resectable nonfunctioning neuroendocrine pancreatic tumors. World J Surg 2004;28:1248-1260.
- Hausman M, Thompson N, Gauger P, et al. The surgical management of MEN-1 pancreatoduodenal neuroendocrine disease. Surgery 2004;136:1205-1211.
- Skogseid B, Eriksson B, Lundqvist G, et al. Multiple endocrine neoplasia type 1: a 10 year prospective screening study in four kindreds. J Clin Endocrinol Metab 1991;73:281-287.
- Skogseid B, Grama D, Rastad J, et al. Operative tumour yield obviates preoperative pancreatic tumour localization in multiple endocrine neoplasia type 1. J Intern Med 1995;238:281-288.
- Skogseid B, Aberg K, Akerstrom G, et al. Experience with multiple endocrine neoplasia type 1 screening. J Intern Med 1995;238:255-261.
- Skogseid B, Aberg K, Akerstrom G, et al. Limited tumour involvement found at multiple endocrine neoplasia type 1 pancreatic exploration: can it be predicted by preoperative tumor localization. World J Surg 1998;22:673-678.
- Stauffer JA, Rosales-Velderrain A, Goldberg RF, et al. Surrogate oncologic markers for long term survival are improved with the use of minimal access surgery for pancreatic cancer. HPB 2012;14 (Supplement 1), 1-91, page 75.

