Keywords
Problematic videogame play; Addiction; Substance use disorder
Introduction
Developing a specific definition for a “videogame” is an everevolving process, as technology continually changes this term’s referent. While the central tenet of playing an electronic game through a visual display remains static, the games themselves have grown in significant ways and changed the landscape of plot-based media from a passive (e.g., television) into an active process. The Entertainment Software Association (2012) [1] has reported that the average household in the United States owns at least one device capable of playing a videogame, the average gamer is 30 years old, and the total revenue for the videogame industry as a whole in 2011 was $24.75 billion. Clearly, playing some form of videogame has become a normative experience for individuals across the entire demographic spectrum. However, this has also opened up entirely new sects of the population to the possibility of problematic play that may result in a host of psychological, behavioral, and interpersonal problems.
The literature is still unclear about the level of “pathology” associated with videogame play, and the term “addiction” references specific features that have not been conclusively demonstrated with regard to videogame play [2]. Thus, “problematic videogame play” (PVGP) has been suggested as the most appropriate term [3,4]. Although the conceptualization of PVGP and its accompanying symptomatology varies across studies, most researchers agree that the term refers to negative consequences resulting from game play, not simply the amount of time spent playing. This constellation of symptoms that encapsulates more than just excessive play may constitute a behavioral addiction, with symptoms that align with those characteristic of addictive disorders. For example, impulsivity is a hallmark of substance use disorders, and this same trait is observed amongst those with PVGP, suggesting a potential for common etiological factors [5,6]. A parallel can be drawn from PVGP and SUD when impulsivity is examined at both the behavioral and electrophysiological levels, lending further support to shared features across PVGP and SUD [7]. Therefore, the potential for using the DSM-5 criteria for substance-related disorders as a model from which to adapt our conceptualization of PVGP will be explored. Towards this end, we used items from validated measures of PVGP [8] to tap specific DSM-5 symptoms, as no single measure of PVGP currently exists that adequately captures the full DSM-5 criteria for SUD or “addiction” [9]. In order to conceptualize PVGP as an addictive behavior, it must first be assessed in accordance with establish criteria for addictive disorders to allow for the comparison with traditional addictions, such as substance use disorder. This marks the first attempt to move the field of video game research in the direction of measuring PVGP as an addiction, without simply defining the behavior as atheoretically “pathological”.
Blaszczynski [10] has noted that simply experiencing negative consequences from excessive playing, a common focus of current literature is not sufficient for addiction. He argues that impaired control, which is central to the concept of addiction, has not been effectively demonstrated. Referencing internet addiction, Shaffer, Hall, and Vander Bilt [11] argue that so-called technological addictions may represent manifestations of other disorders or maladaptive patterns and are not necessarily unique psychiatric conditions. Therefore, there is presently considerable controversy in the literature as to whether excessive gaming constitutes addictive behavior or simply some variant of “problematic” behavior. Regardless, it is generally agreed upon that excessive game playing can have personal and social consequences, and, as such, a number of measures have been developed to assess this phenomenon.
The DSM-5 [12] includes Internet Gaming Disorder (IGD) under the “Conditions for Further Study” section and further exemplifies that gaming may represent an addiction. Specifically, the DSM-5 highlights that videogame playing shares similarities with SUDs and even notes that the Chinese government has labeled internet gaming as an addiction. IGD is characterized as “a pattern of excessive and prolonged Internet gaming that results in a cluster of cognitive and behavioral symptoms, including progressive loss of control over gaming, tolerance, and withdrawal symptoms, analogous to the symptoms of substance use disorders” [12]. While only one study to date has evaluated the diagnostic accuracy of IGD specifically [13], other studies have highlighted the addictive quality of videogames [14,15]. One issue with the current conceptualization of videogame addiction in DSM- 5 is that it emphasizes the internet as a functional component of the playing process. As King and Delfabbro [16] highlight, this “confuses two different delivery mechanisms (i.e., the internet and a video-game) within a single classification” (p. 21). Similarly, Baer, Saran & Green [17] report high correlations between measures assessing online and offline videogame use and further highlight that videogame playing (regardless of online status) “is consistently correlated with emotional and functional problems in youth across multiple measures of addiction and impairment as well as multiple informants” (p. 430). Thus, the DSM-5 conceptualization may be focusing too narrowly on one subtype of videogames (i.e., those played online). Further, a recent review of the neuroscience literature highlights that “Internet gaming addiction appears similar to other addictions, including substance-related addictions, at the molecular, neurocircuitry, and behavioral levels” [18]. Thus, increasing evidence for an addiction model of videogame playing has been materializing. However, one of the main issues that prevented IGD from being formalized within the DSM-5 was the lack of standardized diagnostic criteria across the current literature [19]. Additionally, there are concerns that inclusion of the disorder will eventually lead the term “addiction” to be used for any excessive behavior that causes problems [20].
This lack of a standardized measure for assessing the criteria and severity of IGD has recently led to the creation of a number of scales that attempt to capture this problematic behavior. Unlike the present study, however, these have adhered to the DSM-5 suggested symptomology for IGD, rather than mirroring SUD symptomology, specifically.
Rehbein, Kliem, Baier, Moble and Petry (2015) [21] created the Video Game Dependency Scale by adapting an existing measure to cover the nine DSM-5 criteria required for IGD and tested its validity on a sample of German adolescents, resulting in strong reliability of this measure. This scale represents a highly conservative method of assessing IGD and was constructed in a similar way to Cho et al.’s [22] Internet Addiction (IA) scale, which gathered items from previous internet addiction scales in order to create a new scale aimed at assessing generalized internet addiction. Pontes, Király, Demetrovics and Griffiths [23] assessed both online and offline gaming addiction and created the Internet and Gaming Disorder Test (IGD-20), which has high correlations between the conceptualized 6 factors measured and IGD’s 9 criteria for diagnosis. This new measure was further refined and shortened to a 9 item version that serves as a brief yet valid tool for assessing IGD [24]. Lemmens, Valkenburg, Gentile, [25] also tested both dichotomous and polytomous scales as well as varying measure length in the creation of four different survey measures based on the conception of IGD as comprised of a single factor made up of 9 items representative of the DSM-5 criteria. Regardless of what psychometric tools ultimately become the standard practice within the research, diagnosis, and treatment of IGD, it is imperative that IGD is examined within the context of traditional methods of assessing behavioral addiction. It is important to not only pursue a valid and reliable measure, but also to examine how the constructs of IGD and PVGP are related to other factors associated with methods of understanding addiction that have been studied extensively, such as the criteria and methods of assessing SUD within individuals.
In an attempt to identify the psycho-structural characteristics unique to videogame playing, Wood, Gupta, and Derevensky [26] assessed which game features gamers found most important. The primary categories assessed consisted of sound (sound effects, speaking characters, background music, narration), graphics (realistic graphics, cartoon graphics, full motion video), background and setting (based on an existing story, realistic or fantasy settings), duration of game (long, medium, or short), rate of play (absorption rate), advancement rate (how fast the game play advances), use of humor, control options (player adjustable difficulty, controls, etc.), game dynamics (exploration, quest fulfillment, collecting items, puzzle solving, etc.), winning and losing features (especially points), character development (customization options), brand assurance (brand loyalty), and multiplayer features (online vs. local, cooperative vs. competitive). Results demonstrated that participants placed the highest importance on realistic sound, graphics, and setting. This suggests that for many gamers, realistic, high quality experiences are more attractive and potentially more addicting. Interestingly, when females were analyzed separately (due to their underrepresentation in the general sample), results indicated that women were more likely to prefer nonviolent, less competitive, gentler-paced, cartoon-style games that involve fantasy instead of realism. Thus, gender differences may also exist regarding what is most reinforcing about the gaming experience.
King, Delfabbro and Griffiths [27] have since expanded upon Wood et al.’s [26] taxonomy by addressing some of its limitations, such as refining variables that were difficult to operationalize and better incorporating gambling structural characteristics [28]. Further, King and colleagues [27] noted that their classifications were designed to help future researchers identify the factors that contribute to problematic videogame playing. This model consists of the following five features and their respective subfeatures: Social Features (social utility features, social formation/ institutional features, leader board features, support network features), Manipulation and Control Features (user input features, save features, player management features, noncontrollable features), Narrative and Identity Features (avatar creation features, storytelling device features, theme and genre features), Reward and Punishment Features (general reward type features, punishment features, meta-game reward features, intermittent reward features, negative reward features, near miss features, event frequency features, event duration features, payout interval features), and Presentation Features (graphics and sound features, franchise features, explicit content features, in-game advertising features).
In a follow-up paper, King, Delfabbro and Griffiths [29] assessed videogame players recruited via online advertisements using their Video Game Structural Characteristics Survey, a 37-item self-report measure based on the aforementioned taxonomy. Participants were asked to rate how much they enjoyed each feature, the overall importance of each feature, and how much that feature related to time playing games. Problematic players had higher enjoyment of adult content, finding rare items, watching cut-scenes, and the tactile sensation of the controller. They further reported managing in-game resources, earning points, getting 100% in the game, and mastering the game as the most important aspects. Lastly, leveling up, earning metagame rewards, and fast loading times had the greatest behavioral impact with regard to length of play.
Although the Video Game Structural Characteristics Survey requires psychometric validation and replication is sorely needed, this study represents one of the first attempts to determine which specific aspects of videogames may differentiate problematic players from normative videogamers. This is especially important with modern videogames that no longer mirror real-world “games” with opponents trying to beat each other and instead represent alternate realities in which players reside. Critics of the concept of videogame addiction have specifically argued that these digital playgrounds are too complicated to manifest a simple behavioral addiction analogous to gambling. Thus, attempts at understanding which features relate to problematic play can help quell these concerns and aid in diagnostic understanding.
Given the debate as to whether excessive game play is a symptom of some other unresolved problem or an addictive disorder in its own right, the primary aim of the present study was to determine if a measure that maps onto Substance Use Disorder (SUD) criteria would be conceptually valid and relate in meaningful fashion to a set of variables that are well-documented to be associated with addictive disorders in general, i.e., impulsivity [30], depression [31], self-consciousness [32], poor coping skills [33], and family history of addiction [34]. Due to the abundance of research that went into identifying criteria used for addictive behaviors, it was hypothesized that a DSM-5 conceptualization of PVGP would have better internal consistency and a more robust factor analytic structure than traditional measures of PVGP that are not empirically or theory-driven. It was also predicted that the modified DSM-5 conceptualization of PVGP would have greater criterion validity than existing measures of PVGP. Specifically, an aggregated SUD-based score, using items reflective of each DSM- 5 SUD symptoms, was expected to yield stronger relationships with constructs generally associated with addiction than would scores on existing measures of PVGP, discussed below. Finally, we present a structural model that captures the risk factors for gaming addiction in accordance with factors known to be associated with addictive behavior.
Method
Participants
Participants (N=1,103) were recruited from an undergraduate student population at a large Midwestern University through inclass announcements and a cloud-based participant management software system (SONA-systems.com). Inclusionary criteria consisted of being at least 18 years old and playing videogames at least 1 hour a week. The sample reflected an equal percentage of both male (n=459) and female (n=534) participants whose ages ranged from 18 to 66, with the overall sample matching the typical college-age population (M = 21.36, Mdn= 20, SD = 4.44). The predominant ethnicities within our sample were Caucasian (57.9%) and African American (22.0%). The average time spent playing videogames on a week day was 4.34 hours and the average time spent playing during a weekend day was 5.37 hours (Table 1).
| |
Number of Participants
(n) |
Percentage of Sample |
| Gender |
| Male |
459 |
45.3% |
| Female |
534 |
52.7% |
| Ethnicity |
| Caucasian |
587 |
57.9% |
| African American |
223 |
22.0% |
| Middle Eastern |
32 |
3.2% |
| Asian |
28 |
2.8% |
| Other |
39 |
3.9% |
| Multiracial |
94 |
9.3% |
| Relationship Status |
| Single |
529 |
52.2% |
| Non-cohabiting |
350 |
34.6% |
| Romantic Relationship |
| Married |
64 |
6.3% |
| Living with a Partner |
49 |
4.8% |
| Other |
10 |
1.0% |
Average Time Spent
Playing Videogames |
| On a Week Day |
4.34 Hours |
SD = 2.99 |
| On a Weekend Day |
5.37 Hours |
SD = 3.16 |
Table 1: Participant Characteristics.
Procedure
Before data collection began, study procedures were approved by the Eastern Michigan University Institutional Review Board. Study volunteers first read and digitally signed an informed consent agreement before being eligible to continue. All participants were placed into a raffle with the possibility of winning one of two $50 Amazon.com gift cards.
Measures
Demographic Information: Demographic information was collected, including age, gender, ethnicity, socioeconomic status, years of education, current marital status, current employment status, economic status of current household, and annual household income.
Problematic Video Game Play - Revised (PVGP-R) Scale: The PVGP-R is the newest version of the scale created by Tolchinsky and Jefferson [3]. Questions address the psychological, physical, and social consequences of problematic gameplay. Internal consistencies for each subscale ranged from α = .76 to α = .85, and construct validity was demonstrated using average number of hours spent playing [35].
Video-Game Use (VGU): The VGU is an 11-item measure of PVGP created by Gentile [36]. Rated on a 3-point scale (“yes,” “no,” or “sometimes”), the VGU is adapted from the criteria for pathological gambling, although the wording of some items closely resembles SUD constructs. Internal consistency was reported at α = .78.
Videogame Addiction Scale (VGAS): As highlighted earlier, no single measure of PVGP effectively captures the DSM-5 criteria for SUD [9,37]. Thus, items were chosen from existing measures to develop a set of items that mapped onto SUD criteria. These items were not re-administered; rather, answers to them were lifted from responses to the above-described measures, to create a VGAS score used in the analyses described below. SUD Criterion 1, referencing usage in larger amounts or over a longer period than was intended, was assessed by item 23 on the PVGP-R (“I play video games over a longer time period than I intended”). The second criterion, which highlights a persistent desire or unsuccessful effort to cut down or control substance use, was captured in the third item of the VGU (“Have you tried to play video games less often or for shorter periods of time, but were unsuccessful?”). Criterion 3 requires that a great deal of time is spent in obtaining, using, or recovering from substance use. Given that obtainment of and recovery from videogames are not nearly as problematic as for psychoactive substances, item 6 of the PVGP-R (“I spend an increasing amount of time playing video games”) was deemed to assess the problematic amount of time invested. DSM-5 Criterion 4 assesses cravings, defined as a strong desire or urge to use the substance. In an effort to capture the future-oriented aspect of cravings (e.g., the preoccupation with wanting to use the substance again), item 11 on the PVGP-R (“When I am not playing video games, I am often planning how I will play my next game”) was chosen. Criterion 5 refers to a failure to fulfill major role obligations at work, school, or home due to substance use. Interestingly, several measures of PVGP merge school/work problems with interpersonal problems, which represent separate criteria for SUD. Thus, item 25 of the PVGP-R (“In order to play video games, I have skipped class or work”) was chosen, as it does not include other functional impairments. Criterion 6 represents persistent or recurrent social or interpersonal problems and was captured via item 20 on the PVGP-R (“In order to play video games, I get into arguments with people”). Criterion 7 captures the reduction or giving up of social, occupational, or recreational activities and is reflected in item 2 of the PVGP-R (“Because of my video game playing, I have spent less time with my friends and family”). Criterion 8, which highlights physically hazardous situations related to substance use, was not assessed, as videogames do not have an obvious parallel. Criterion 9 assesses continued substance use despite physical or psychological problems. With the exception of the PVGP-R, no other measure explicitly captures the physical problems associated with problematic videogame playing. However, the PVGP-R includes items referencing neck pain (#7), wrist pain (#14), headaches (#22), hand pain (#24), and back pain (#33). Inclusion of physical effects from problematic playing allows for an extension beyond solely psychological effects and creates a closer analogue to SUD. Thus, affirmation of any of the aforementioned items on the PVGP-R was considered as endorsement of criterion 9. Criterion 10 captures the concept of tolerance, defined as either a need for increased amounts to achieve the desired effect or as a diminished effect when using the same amount. Item 2 of the VGU (“Do you need to spend more and more time and/ or money on video games in order to feel the same amount of excitement?”) alone captures the SUD conceptualization of tolerance and thus was included in this aggregation. Lastly, Criterion 11 refers to withdrawal, which includes either the characteristic withdrawal symptoms of a substance or the use of the substance to avoid these withdrawal symptoms. Given that pathological gambling literature has consistently shown that withdrawal from gambling typically includes restlessness and irritability [38], similar symptom markers were used to assess videogame withdrawal. Item 4 of the VGU (“Do you become restless or irritable when attempting to cut down or stop playing video games?”) appeared to suitably capture the concept. Withdrawal symptoms have been reported in individuals with gambling disorder and some substance use disorders as well as in individuals who engage in PVGP, with reports of similar symptom manifestation when there is an inability to initiate or purposefully stop engaging in the activity [8].
Merged together, these 10 items represented the 10 SUD criteria measured in this study. However, the PVGP-R and VGU utilize different metrics for responding, with the former employing a 5-point Likert scale and the latter a 3-point scale. To correct for this, scores on VGU items were mapped onto a 5-point scale such that “no” becomes “never” (1), “maybe” becomes “sometimes” (3), and “yes” becomes “often” (5). Although another option would have been to mathematically transform the 3 anchors to fit on a 5-point scale (e.g., multiply each score by 1.667), this would place a negative response in between “never” and “sometimes” on the PVGP-R scale. Thus, individuals who have never experienced the symptom of a given item would have artificially inflated scores on the three items from the VGU as compared to the seven PVGP-R items. It should be noted that the complete PVGP-R and VGU measures were administered as part of the online questionnaire, negating the need to form a specific survey or to group items accordingly. This allowed for the evaluation of PVGP as intended by the scales’ creators in addition to the examination of SUDadapted criteria.
Brief Version of Video Game Structural Characteristics: The original version of this measure [29] included 111 items assessing game features related to social aspects, manipulation and control, narrative and identity, reward and punishment, as well as presentation. Specifically, 37 structural characteristics were rated on three items assessing enjoyment (“How much do you enjoy this feature of the video game?”), perceived importance (“How important do you believe this feature is to the playing experience?”), and behavioral impact (“What is the extent to which this feature contributes to longer playing times?”). Responses were scored on a 5-point Likert scale ranging from “Not at all” to “High importance.” However, King and colleagues [29] highlighted only the top 15 characteristics for each question, as the authors noted that these had the strongest statistical findings and the most utility. Thus, in an effort to increase the brevity of this measure, only the top 15 items on enjoyment, perceived importance, and behavioral impact were used for the current study.
AUDIT: The Alcohol Use Disorders Identification Test (AUDIT; [39] is generally considered one of the best screening tools for assessing a range of alcohol problems (Fiellin, Carrington, O’Connor, 2000) [40].
Brief Young Adult Alcohol Consequences Questionnaire (B-YAACQ): The B-YAACQ [41] is a 24-item measure of problematic drinking specifically for use with college students. This measure has been shown to have high internal consistency, minimal item redundancy, reliability over time, sensitivity to change, and does not yield floor or ceiling effects [42].
Family History of Addiction: One item from the South Oaks Gambling Screener (SOGS) [43] assessing “Which of the following people in your life has (or had) a gambling problem” was adapted for the current study. Specifically, participants completed this question with regard to SUDs, gambling, and videogame playing. In the current study, three variables were constructed and reported: total individuals with a gambling problem, total number with an alcohol or other drug (AOD) problem, and total number with a videogame problem.
Patient Health Questionnaire – Depression Scale (PHQ-9): The PHQ-9 [44] is the 9-item depression subscale of the PHQ, which assesses the level of depression over the past two weeks using a 4-point Likert scale ranging from “Not at all” to “Nearly every day.” Total scores range from 0 to 27, with suggested severity categories of 0-4 (none), 5-9 (mild), 10-14 (moderate), 15 -19 (moderately severe), and 20-27 (severe).
Barratt Impulsiveness Scale, Version 11 (BIS-11): The BIS-11 [45] is a commonly utilized measure of impulsivity. Consisting of 30 items rated on a 4-point Likert scale (ranging from “Rarely/ Never” to “Almost always/Always”), the BIS-11 comprises three subscales: motor impulsivity (action without thought), nonplanning impulsivity (lack of future orientation), and cognitive impulsivity (poor attention and concentration).
Self-Consciousness Scale (SCS): The SCS [46] measures selfconsciousness in three domains: private self-consciousness (attending to inner thoughts and feelings), public selfconsciousness (general awareness of the self in a social context), and social anxiety (the experience of discomfort in the presence of others). The measure consists of 23 items rated on a 5-point Likert scale, ranging from “Extremely Uncharacteristic” to “Extremely Characteristic.”
Brief Coping Orientation for Problems Experienced (COPE) Inventory: The Brief COPE [47] is a 28-item measure of the way in which individuals cope with stress. Its 14 subscales include active coping, planning, positive reframing, acceptance, humor, religion, using emotional support, using instrumental support, self-distraction, denial, venting, substance use, behavioral disengagement, and self-blame.
Data Analysis
Participants were divided into two samples that did not meaningfully differ on PVGP-related variables or demographic characteristics (henceforth referred to as the validation and cross-validation samples). Exploratory factor analyses using geomin rotation were then conducted on the validation sample, and these models were subsequently tested via confirmatory factor analyses with the cross-validation sample. Separate analyses were conducted for the PVGP-R, the VGU, and the VGAS, respectively. Factor inclusion was determined using the following techniques: the screen test [48], which involves an examination of the scree plot, the Kaiser-Guttman rule, in which factors with eigenvalues greater than 1 are included in the model [49], and parallel analysis, for which each factor’s eigenvalue is compared with those obtained from a random data matrix [50]. Further, internal consistency was examined using Cronbach’s alpha. Factor analyses were conducted using Mplus© 5.21 [51]. Once sufficient results had been achieved with the EFA, a confirmatory factor analysis (CFA) was conducted on the cross-validation sample. The fit of the CFA model to the cross-validation data was determined using the root mean square error of approximation (RMSEA) [52,53] and the comparative fit index (CFI; Bentler, 1990) [54].
As we also aimed to compare the relationships between various measures of PVGP and constructs theoretically related to addiction, correlation matrices were calculated for each measure of PVGP (PVGP-R, VGU, and our extracted VGAS score) and the BIS- 11, PHQ-9, B-YAACQ, and family history of addiction. Correlation matrices were then compared using Fisher’s transformation [55], which converted r values into z-scores. Thus, the strength of these relationships was statistically compared to determine if one scoring method yielded significantly stronger correlations with variables generally associated with addictive disorders.
Lastly, SEM was used to develop a model that accurately described the relationship between variables. Modeling was conducted using Mplus© 5.21 [51]. Prior to data collection, it was difficult to develop hypotheses about how the specific variables would interact, although model fit was examined to determine the best arrangement of variables. In order to address any missing data, the CFA used the full information maximum likelihood (FIML) method, which allowed Mplus to estimate the missing values.
Results
VGU: As this measure is conceptualized as being unidimensional, an initial CFA was conducted using the validation sample to determine if a one-factor solution adequately fit the data; results suggested poor fit using the CFI (.72) and RMSEA (.12) fit indices, χ2 (44) = 345.71, p < .001. This suggests that the 11 items of the VGU likely represent more than one latent construct and would likely load onto several factors.
Thus, an EFA was conducted on the VGU items for participants in the validation sample. Regarding the Kaiser-Guttman rule [49], the eigenvalues suggested a 3-factor solution. For the screen test [48], results suggested that the third factor represented the “break point” of the graph, warranting the retention of a 3-factor solution. Results of the parallel analysis [50] suggested that a 2-factor solution was best.
Given the discrepancy between the parallel analysis and other factor retention methods, the CFI and RMSEA fit indices were examined as well. Results of the 2-factor EFA yielded a CFI of .94 and an RMSEA of .06, χ2 (34) = 99.98, p < .001; whereas, the 3-factor solution generated a CFI of .98 and an RMSEA of .04, χ2 (25) = 44.75, p = .01. A chi-square model comparison suggested that these models were statistically different from one another, Δ χ2 (9) = 55.23, p < .01. However, the fit indices suggest that both models had good fit. The specific loadings for each item on the resulting factors were statistically evaluated to determine how items grouped across factors for the two models. To make this determination, the standard errors of the factor loadings were used to examine fit by determining significance using the z-statistic. The two-tailed Bonferroni critical value was calculated at α = .05 by accounting for the number of factors and items to adjust for alpha inflation, yielding a critical z-statistic of 3.02 for the 2-factor and 3.10 for the 3-factor solutions. Thus, all estimated/standard error values for the item loadings that exceeded the respective number loaded significantly on that factor, regardless of the loading value itself. Results of the 2-factor solution suggested that 10 items of the VGU significantly loaded on only one factor and one item loaded on two factors; whereas, for the 3-factor solution, two items cross-loaded. Overall, the 3-factor solution generated good fit indices, appeared to have a better fit based on a chi-square model comparison, and seemed most appropriate based on the Kaiser-Guttman rule as well as visual examination of the scree plot. Thus, the 3-factor solution, which accounted for 54.99% of the variance, was adopted.
To determine if this model accurately reflected the data, a CFA of the 3-factor model was conducted on the cross-validation sample. Results suggested mediocre fit using both CFI (.91) and RMSEA (.07), χ2 (40) = 128.39, p < .001. The VGU’s internal consistency was calculated across the entire sample (validation and cross-validation combined), yielding a Cronbach’s alpha of .77, which is similar to the value provided by the measure’s author (α = .78; 36)
PVGP-R: An initial CFA was conducted on the PVGP-R items within the validation sample using the 6-factor solution provided by Tolchinsky [35]. This yielded inadequate fit, as measured by the CFI (.88) and RMSEA (.07), χ2 (309) = 1124.35, p < .001. Thus, an EFA was conducted on the 27 items of the PVGP-R and the aforementioned factor retention methods analyzed. Specifically, the Kaiser-Guttman rule [49] advocated that a 6-factor solution was best, the scree plot (Cattel, 1966) [48] was suggestive of a 4-factor solution, and the parallel analysis [50] indicated a 4-factor solution kept eigenvalues above chance values. The fit indices of both the 4-factor and 6-factor solutions were compared: the 4-factor solution resulted in poor fit (CFI = .88, RMSEA = .08, χ2 (249) = 1029.81, p < .001) and the 6-factor solution generated better fit (CFI = .93, RMSEA = .07, χ2 (226) =702.56, p < .001). A chi-square model comparison suggested that the 6-factor solution may better represent the data, Δ χ2 (23) = 327.25, p < .001, and was chosen for further examination. The resulting 6-factor solution accounted for 64.93% of the variance. Loadings were evaluated using an adjusted two-tailed Bonferroni critical value converted into a critical z-statistic of 3.55. All items significantly loaded on at least one factor, though five items significantly loaded on more than one factor.
To determine if this model accurately reflected the data, a CFA of the 6-factor model was conducted on the cross-validation sample. Results suggested poor fit using CFI (.88) and mediocre fit using RMSEA (.07), χ2 (304) = 1074.41, p < .001. The internal consistency of the PVGP-R was calculated across the entire sample (validation and cross-validation combined), yielding a Cronbach’s alpha of .92.
VGAS: Because the aggregated scale was created for the purposes of the current study and no a priori model existed, an EFA was conducted on the 10 items used for the VGAS. While the Kaiser-Guttman rule [49] suggested that two factors would be appropriate, the third factor generated an eigenvalue of 0.99, which is just below the cutoff. Further, the screen test [48] and parallel analysis [50] corroborated the 2-factor solution as most appropriate. Interestingly, when examining the fit indices for the 2-factor (CFI = .96, RMSEA = .07, χ2 (26) = 80.29, p < .001) and 3-factor (CFI = .99, RMSEA = .03, χ2 (18) = 26.36, p = .09) solutions, the chi-square test of model fit yielded non-significant results for the 3-factor solution. Non-significance denotes that the sample covariance matrix does not differ from the population covariance matrix (null hypothesis), which is the desired result. While chi-square is typically sensitive to sample size and can generate significant results even in good models that utilize a large number of participants [56,57], the aforementioned nonsignificance speaks to the 3-factor solution’s strength. A chisquare model comparison was conducted to compare the two solutions; results indicated that they statistically differed from one another, Δ χ2 (8) = 53.93, p < .001. Given that the 3-factor solution generated robust fit indices and accounted for 61% of the variance, it was selected for subsequent analyses. Examination of the item loadings within the model suggests that the first factor captures underlying mechanisms of tolerance and withdrawal as well as the associated loss of control over use. The second factor highlights issues related to the amount of time spent playing as well as physical pain (i.e., likely a function of excessive play time). Lastly, the third factor addresses both social problems and a failure to fulfill social role obligations (Table 2).
| S.no |
|
Factor 1 |
Factor 2 |
Factor 3 |
| 1) |
Play for longer period than intended |
.01 |
.73 |
-.20 |
| 2) |
Unsuccessfully tried to play for less time |
.79 |
-.01 |
-.26 |
| 3) |
Spend increasing amount of time playing |
-.04 |
.85 |
-.01 |
| 4) |
Planning how I will play my next game |
-.01 |
.57 |
.31 |
| 5) |
Skipped class/work to play |
.21 |
.10 |
.44 |
| 6) |
In order to play, I get into arguments with people |
.26 |
-.01 |
.62 |
| 7) |
Spent less time with family/friends |
.16 |
.59 |
.01 |
| 8) |
Experienced neck, wrist, hand, or back pain or headaches |
.14 |
.42 |
.17 |
| 9) |
Spend more time/money to feel same excitement |
.39 |
.10 |
.12 |
| 10) |
Become restless/irritable when cutting down |
.83 |
-.01 |
.01 |
Bold loadings represent p < .05.
Table 2: Exploratory Factor Structure of the Videogame Addiction Scale (VGAS).
As with the previous models, a CFA of the 3-factor solution was conducted on the cross-validation sample (Figure 1). Results suggested good model fit, based on the CFI (.96) and RMSEA (.06), χ2 (30) = 83.43, p < .001. This suggests that the model generated as part of the EFA was accurately representing the data in CFA when loadings were constrained to the a priori relationship. The internal consistency of the aggregated model was α = .81. Examination of the item loadings within the model suggests that the first factor captures tolerance and withdrawal as well as the associated lack of control when trying to stop. The second factor highlights consequences related to the amount of time spent playing as well as physical pain. Lastly, the third factor addresses both social problems and failure to fulfill role obligations.
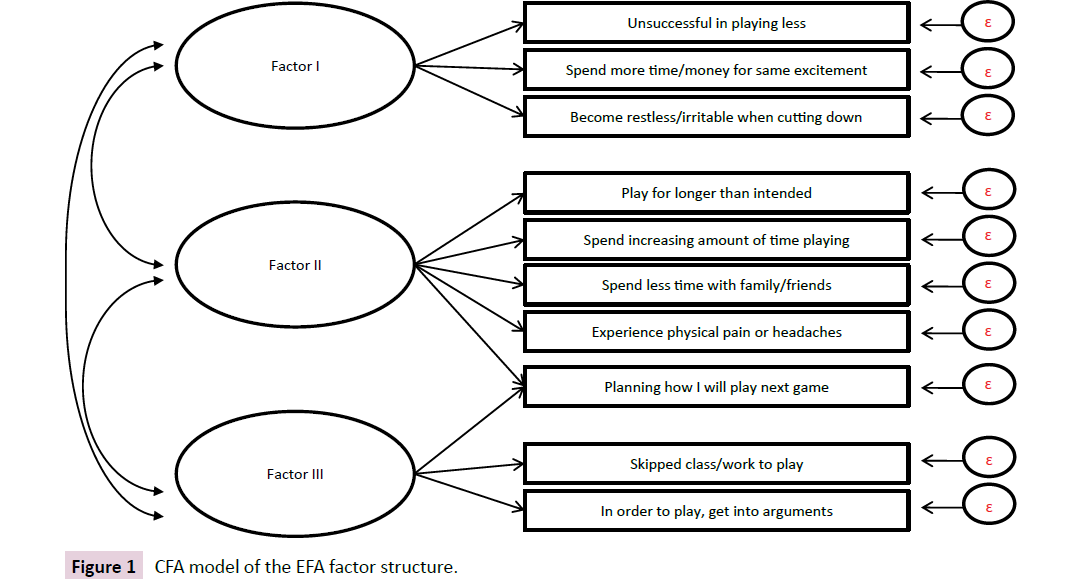
Figure 1: CFA model of the EFA factor structure.
To evaluate the criterion validity of the three measures of PVGP, each score was correlated with the BIS-11, PHQ-9, B-YAACQ, AUDIT, COPE, SCS, and family history of addiction. Examination of the correlation coefficients (Table 3) yielded expected relationships with related variables, including inattention, particular methods of coping, self-consciousness, substance use, and acquaintances/ peers suffering from videogame-related issues.
| |
PVGP-R |
VGU |
Videogame
Addiction Scale |
| Total Score for the PVGP-R |
|
| Total Score for the VGU |
.61** |
|
| Total Score for the Videogame Addiction Scale |
.86** |
.74** |
|
| Cognitive/Attentional Subscale of the BIS-11 Scale |
.28** |
.29** |
.30** |
| Motor Subscale of the BIS-11 |
.22** |
.25** |
.26** |
| Non-planning Subscale of the BIS-11 |
.07 |
.20** |
.16** |
| Total Score for PHQ-9 |
.37** |
.36** |
.37** |
| Active Coping Subscale of the COPE |
.02 |
-.11** |
-.08* |
| Planning Subscale of the COPE |
.02 |
-.07* |
-.04 |
| Positive Reframing Subscale of the COPE |
.07* |
-.03 |
.01 |
| Acceptance Subscale of the COPE |
.09** |
-.02 |
.01 |
| Humor Subscale of the COPE |
.20** |
.14** |
.16** |
| Religion Subscale of the COPE |
-.03 |
-.05 |
.02 |
| Using Emotional Support Subscale of the COPE |
.02 |
-.04 |
-.04 |
| Using Instrumental Support Subscale of the COPE |
.04 |
-.02 |
-.01 |
| Self-Distraction Subscale of the COPE |
.23** |
.15** |
.13** |
| Denial Subscale of the COPE |
.23** |
.19** |
.27** |
| Venting Subscale of the COPE |
.19** |
.14** |
.18** |
| Substance Use Subscale of the COPE |
.19** |
.18** |
.21** |
| Behavioral Disengagement Subscale of the COPE |
.29** |
.24** |
.32** |
| Self-Blame Subscale of the COPE |
.23** |
.20** |
.21** |
| Private Self-Consciousness Subscale of the SCS |
.15** |
.03 |
.06 |
| Public Self-Consciousness Subscale of the SCS |
.17** |
.04 |
.10** |
| Social Anxiety Subscale of the SCS |
.18** |
.10** |
.14** |
| Total Score for the B-YAACQ |
.14** |
.17** |
.18** |
| Total score for AUDIT Items |
.15** |
.15** |
.14** |
| Total # of People in Life that have Gambling Problem |
.05 |
.07* |
.06 |
| Total # of People in Life that have AOD Problem |
.07* |
.05 |
.06 |
| Total # of People in Life that have Videogame Problem |
.16** |
.14** |
.15** |
Note: * p < .05; ** p < .01
Table 3: Correlation Coefficients for Measures of PVGP and Criterion Variables.
To compare the strengths of the relationships between the three measures of PVGP and associated criterion variables, Fisher’s r-to-z transformation analyses were computed [55]. Two z-values can then be statistically compared in order to obtain a p-value and determine if they significantly differ from each other. Further, the positive or negative value of the z-score can help determine the direction of the correlation, ensuring that relationships are manifested in expected ways. Thus, three calculations were computed for each criterion variable: a comparison of PVGP-R to VGU, PVGP-R to the VGAS, and VGU to the VGAS. The Z-critical values for p < .05 and p < .01 are 1.96 and 2.58 respectively (Table 4).
| |
PVGP-R & VGU |
PVGP-R & Addiction Scale |
VGU & Addiction Scale |
| Cognitive/Attentional Subscale of the BIS-11 Scale |
-0.23 |
-0.37 |
-0.14 |
| Motor Subscale of the BIS-11 |
-0.78 |
-1.03 |
-0.25 |
| Non-planning Subscale of the BIS-11 |
-3.00** |
-1.95 |
1.05 |
| Total Score for PHQ-9 |
0.24 |
0.02 |
-0.22 |
| Active Coping Subscale of the COPE |
2.77** |
2.10* |
-0.66 |
| Planning Subscale of the COPE |
1.88 |
1.32 |
-0.56 |
| Positive Reframing Subscale of the COPE |
2.08* |
1.49 |
-0.59 |
| Acceptance Subscale of the COPE |
2.44* |
1.71 |
-0.73 |
| Humor Subscale of the COPE |
1.29 |
0.97 |
-0.33 |
| Religion Subscale of the COPE |
0.38 |
-1.17 |
-1.55 |
| Using Emotional Support Subscale of the COPE |
1.34 |
1.28 |
-0.06 |
| Using Instrumental Support Subscale of the COPE |
1.30 |
1.06 |
-0.23 |
| Self-Distraction Subscale of the COPE |
1.81 |
2.07* |
0.26 |
| Denial Subscale of the COPE |
0.90 |
-0.90 |
-1.80 |
| Venting Subscale of the COPE |
1.02 |
0.29 |
-0.74 |
| Substance Use Subscale of the COPE |
0.20 |
-0.46 |
-0.66 |
| Behavioral Disengagement Subscale of the COPE |
1.18 |
-0.84 |
-2.03* |
| Self-Blame Subscale of the COPE |
0.67 |
0.38 |
-0.29 |
| Private Self-Consciousness Subscale of the SCS |
2.45* |
1.95 |
-0.50 |
| Public Self-Consciousness Subscale of the SCS |
2.68** |
1.59 |
-1.09 |
| Social Anxiety Subscale of the SCS |
1.66 |
0.82 |
-0.83 |
| Total Score for the B-YAACQ |
-0.73 |
-0.97 |
-0.23 |
| Total score for AUDIT Items |
-0.04 |
0.28 |
0.32 |
| Total # of People in Life that have Gambling Problem |
-0.26 |
-0.13 |
0.13 |
| Total #of People in Life that have AOD Problem |
0.50 |
0.26 |
-0.24 |
| Total # of People in Life that have Videogame Problem |
0.56 |
0.22 |
-0.33 |
Note: * p < .05; ** p < .01
Table 4: Z-scores for Comparisons of the Three PVGP Measures.
Taken together, results suggest that the VGAS exhibits good criterion validity when compared to measures of impulsivity, depression, less adaptive coping strategies (e.g., denial, substance use, behavioral disengagement, self-blame), self-consciousness and social anxiety when in public, and alcohol use. Results also indicate that the factor analytic structure of the VGAS is excellent (CFI = .99, RMSEA = .03, χ2(18) = 26.36, p = .09) and accurately represents the data from a separate sample (CFI = .96, RMSEA = .06, χ2(30) = 83.43, p < .001). Lastly, the VGAS has good internal consistency, as measured by Cronbach’s Alpha (α = .81).
The structural characteristics that were deemed to contribute to longer playing times were also analyzed (Table 5). Specifically, 11 items were evaluated via 3x2 ANOVAs, which were all significant and ranged from F(5,902) = 7.39, p < .001 (different story outcomes) to F(5,902) = 14.71, p < .001 (emotional investment in a character). Further, all genre main effects were significant as well in the same pattern (i.e., MMORPG > Shooter > Other). Only three structural characteristics yielded significance, including ability to correct mistakes by reloading a save file, F(1,902) = 4.04, p = .05, emotional investment in a character, F(1,902) = 9.57, p = .002, and sound, F(1,902) = 9.00, p = .003. Post-hoc analyses confirmed that greater endorsement of these items was observed for the high VGAS group. There were no significant interactions, including no interaction between game genre and structural characteristics. While each variable was tested separately within the models highlighted below, the summed characteristics associated with longer playtime fit notably better each time; thus, descriptions of the following models all refer to the total of the structural characteristics rated as most related to playing longer. Specifically, these were the ability to correct mistakes by reloading a save file, emotional investment in a game character, and sound.
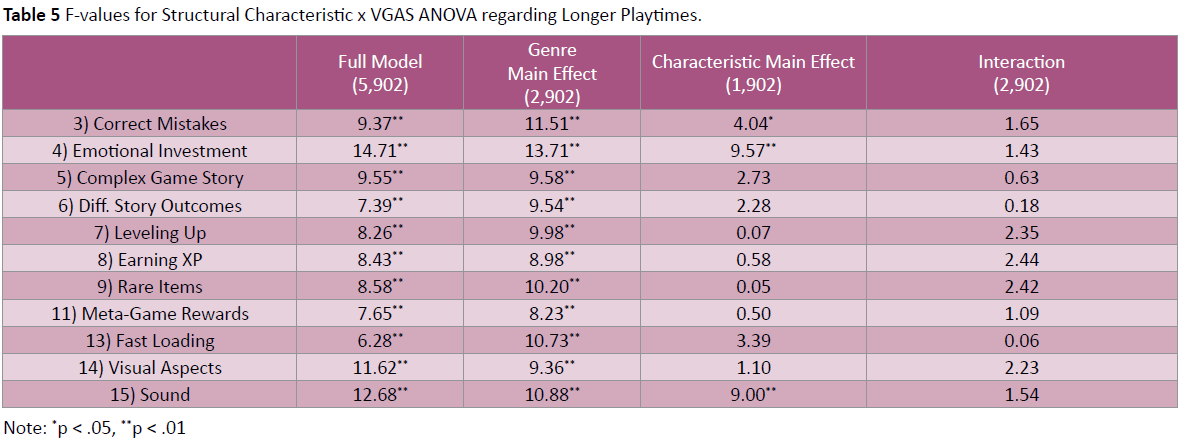
Table 5: F-values for Structural Characteristic x VGAS ANOVA regarding Longer Playtimes.
To further evaluate whether “problematic play” might best be conceptualized as addictive behavior, we tested models that included variables that are generally associated with addiction to predict VGAS scores. The variables described above were evaluated via structural equation modeling using Mplus© 5.21 [51]. A number of models were tested, with the best fit obtained by the final model, which hypothesized that VGAS scores would be predicted by the measures of playtime, impulsivity, and coping strategies. Further, weekly playtime and the structural characteristics were allowed to correlate. Lastly, playtime was assumed to be predicted by impulsivity. This model is visually represented in Figure 2. Results yielded good model fit based on the CFI (.97) and nearly good fit using the RMSEA (.07), χ2 (2) = 11.79, p = .003. This suggests that impulsivity likely leads to longer playtime, which in turn relates to the videogame characteristics that players’ value. Lastly, maladaptive coping strategies, weekly playtime, and valued structural characteristics all predict VGAS scores.
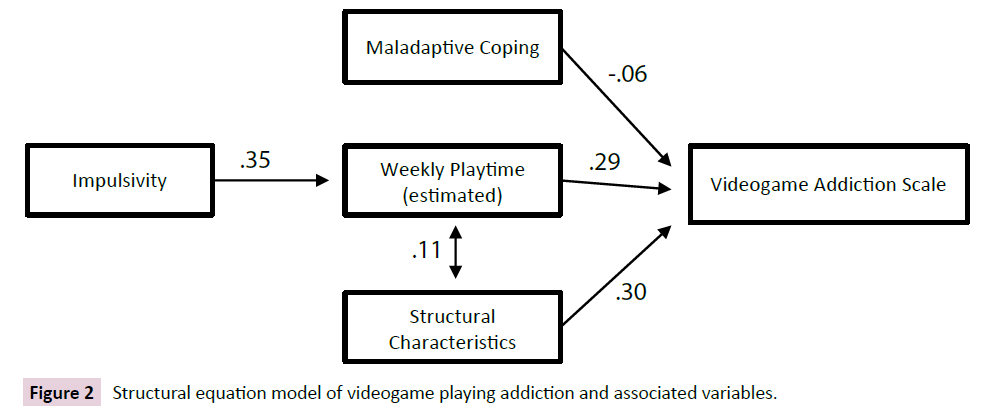
Figure 2: Structural equation model of videogame playing addiction and associated variables.
Discussion
The current study sought to explore the concept of problematic videogame playing (PVGP), comparing the most notable PVGP measures to each other in order to determine the best instrument for capturing the phenomenon of excessive game playing. The large sample recruited for the current study allowed for a variety of statistical analyses to be conducted, including modeling on subsamples that require hundreds of individuals. Thus, this paper represents one of the first systematic attempts to directly compare measures of PVGP on their factor analytic structure, and it is the first to explicitly address the extent to which PVGP fits with an addiction model akin to that applied to substance use disorders.
Results of exploratory factor analyses suggested that the scale generated from adapting the substance use disorder (SUD) criteria of the DSM-5 [12], i.e., our VGAS, had the best overall model fit. Further, when models were tested via confirmatory methods, only the VGAS yielded a good fit. Thus, the addiction model of problematic videogame playing seems to represent the current data well. Examination of the VGAS’ factor structure highlighted that the first factor captured items assessing unsuccessful efforts to play less (criterion 2), spending more time/money for the same excitement (criterion 10), and becoming restless/irritable when cutting down (criterion 11). Thus, this factor appears to capture the underlying mechanisms of tolerance and withdrawal as well as the associated lack of control when trying to stop. The second factor encapsulated playing for longer than intended (criterion 1), spending increasing amounts of time playing (criterion 3), spending less time with family/friends (criterion 7), experiencing physical pain (criterion 9), and planning future games when not playing (criterion 4). Thus, the second factor consisted of the items addressing time playing and not doing other activities as well as playing games to the point of experiencing physical pain. Collectively, these items seem to capture the narrow reinforcement menu that is common to other forms of addiction, wherein the primary source of reward and motivation comes from substance/activity to which one is “addicted,” to the exclusion of other available reinforcers. Lastly, the third factor included preoccupation with how to play future games, as well as skipping class/work to play (criterion 5) and getting into arguments with others (criterion 6). Thus, the last factor captured primarily psychosocial problems associated with game play. Interestingly, it was the item addressing craving/preoccupation that cross loaded; suggesting that elements of having a strong desire to play videogames when not actually playing may relate to time spent playing as well as psychosocial difficulties. The VGAS is available in Appendix A.
While this factor structure appears to fit the current data, it does not match the factor analytic investigations of substance use disorders. Although less research is available on the current criteria for SUD within DSM-5 [12], several studies have combined the abuse and dependence criteria from DSM-IV-TR [58], which collectively align with the current conceptualization of SUD.Thus, when combining the DSM-IV abuse and dependence criteria together, Saha et al. [59] yielded 1-factor solutions for amphetamines, cocaine, prescription drugs, tranquilizers, and opioids (CFIs = .97 to .99, RMSEAs = .03 to .05). Similar results were found by Fulkerson, Harrison, and Beebe [60] across two samples (Goodness-of-Fit = .99, RMSEA = .05 for both). Additionally, unidimensional models were presented by Rounsaville, Bryant, Babor, Kranzler, and Kadden [61] and Nelson, Rehm, Ustun, Grant, and Chatterji [62]. Taken together, this suggests that while videogame addiction may be best assessed using the same criteria as for SUDs, the relationships between these criteria differ. That is, our results did not support the unidimensional model proposed in the SUD literature.
Model of Videogame Addiction
Utilizing the results obtained from the previous analyses, a model of videogame addiction was constructed to help determine if the association between variables followed expected patterns, based on the SUD literature. Specifically, the following variables were included in the model: impulsivity, maladaptive coping, weekly playtime, and the structural characteristics associated with longer playtime. A brief overview of the literature with regard to analogous substance-related variables is presented below.
Elevated impulsivity, as measured by self-report, has been observed among those who experience SUDs involving psychostimulants [63], opiates [64-66], alcohol [67], and ecstasy [68,69]. Additionally, elevated impulsivity scores have been observed among those with pathological gambling [70,71]. Taken together, these results suggest that impulsivity should be included in an adapted model of videogame addiction.
When examining the literature regarding coping mechanisms, different coping strategies are generally classified into one of two categories: active coping, which often involve problemsolving, planning, and help-seeking behaviors; and avoidant/ negative coping, which includes denial, self-distraction, behavioral disengagement, and substance use [72]. Negative coping strategies have been associated with or predicted SUDs in a variety of populations, including homeless adults [73], incarcerated individuals [74], manufacturing workers [75], working professionals [76], adolescents [77,78], abuse victims [79], and so on. Thus, it appears that across a variety of demographic characteristics, engaging in maladaptive coping behaviors may lead to or at least be associated with SUDs. Interestingly, the coping strategies most related to VGAS scores in the current study were the following: behavioral disengagement, denial, self-blame, and substance use. All of these constitute avoidant/negative coping strategies, making the current findings commensurate with the broader SUD literature.
For the purposes of evaluating an addictions model within the current study, weekly playtime was conceptualized as a measure of “exposure.” This made conceptual sense, given that playtime is a direct measure of the amount of hours one is exposed to the desired stimulus; in this case videogames. Further, given that playtime is not necessarily indicative of problematic videogame play [80], it was deemed appropriate to conceptually separate playtime from scores of videogame addiction.
Lastly, in line with literature that “route of administration” within SUD forms of addiction can act as a determinant of problematic use, the structural characteristics were included in the overall model. That is, structural characteristics were regarded as mechanisms for more rapid exposure to potentially addictive elements of gaming. Therefore, given that these structural characteristics essentially address the user experience and interaction with a game, the literature regarding route of substance delivery was examined. For example, Hatsukami and Fischman [81] highlight that the difference in addiction levels between cocaine hydrochloride (snorted) and crack cocaine (smoked) is primarily due to the rate of onset as well as the intensity and duration of the effect. Further, many users of crack cocaine actually began with intranasally-administered cocaine hydrochloride and shifted delivery mechanisms to smoking crack [82-85]. Thus, while the two types of cocaine are chemically the same, the characteristics of route of administration play a role. Similarly, games that allow players to correct mistakes by reloading a saved file, feel an emotional connection to a character, and experience immersive sound may also exhibit a higher addictive potential as a function of how they “deliver” the game.
The overall best-fitting model highlighted that impulsivity predicts weekly playtime; thus, individuals with higher self-reported impulsivity tend to play more throughout the week. Playtime was correlated with the structural characteristics associated with longer playtime, which makes intuitive sense. Specifically, individuals who report that certain characteristics impact their playtime are thus likely to play longer. Lastly, avoidant/negative coping, weekly playtime, and the structural characteristics all predicted videogame addiction. The relationships of these variables is commensurate with what would be expected based on the previously discussed addiction literature. Thus, similar underlying mechanisms may ultimately contribute to the manifestation of addiction symptomatology for both videogames and substances.
Limitations
The current study has some limitations. First, given that the survey was open to all undergraduate students, it is not possible to calculate response rates. Further, it is unclear if individuals who completed the survey represent a specific subsample of eligible individuals or if results are generalizable to a general student population. As noted earlier, the age of videogame players may shape the reported reasons for playing [86]; even if all individuals are playing the same game. Thus, our results may only capture the characteristics of videogame addiction as well as the relationship of associated variables within a Midwestern college population. However, given the ubiquity of videogame play among college students as well as the possibility for addiction to negatively impact students’ academic/career trajectories, this is still a population worth investigating.
Additionally, except for the PVGP items, it was permissible for participants to skip survey items, and, as such, there was some missing data throughout the database. Thus, it is unclear if there were meaningful differences between participants who completed a given measure and those who did not. However, with a sample size of over a thousand participants, it was conjectured that a pattern of systematic bias was unlikely, as the sheer number of participants would likely counteract any emerging patterns of bias.
The current study also did not allow for teasing apart how different game types influence differences in regard to addiction level or severity of PVGP. For example, criterion 7 of the VGAS, which focuses on the reduction or giving up of social, occupational, or recreational activities, reflected in item 2 of the PVGP-R (“Because of my videogame playing, I have spent less time with my friends and family”), does not take into account whether the term “videogame playing” refers to online or offline videogame playing. However, the present study did not assess the degree to which participants may have spent less time with some offline friends but more time with other online players. Future studies should address this limitation by further investigating the way different structural characteristics within videogames can affect the level to which an individual engages in problematic use, including assessment of gaming impact on online versus offline social interaction. In addition, future research should examine if certain game types are more addictive than others based on their structural characteristics and how these characteristics can impact the level of addiction behavior.
An additional limitation of the current study is that the VGU responses that are measured using a 3-point Likert scale had to be compared and mapped onto the 5-point scale of the PVGP-R. The scales were left intact in their original format in order to ensure that the questions asked were not redundant and to avoid corrupting the original measures. Unfortunately, this meant that the participants had to utilize different scales when responding. This also created the dilemma of respondents selecting “maybe” without the response being directly equivalent to responding “sometimes.” Future studies should examine these responses using the same metric in order to avoid discrepancies between scales.
Conclusion
To date, many measures of problematic videogame play have been utilized in the literature without any systematic investigation of which is the most appropriate/accurate or if common variables exist across measures. This lack of a standardized definition was cited as one of the major reasons for classifying Internet Gaming Disorder (IGD) as a “condition for further study” within DSM-5 and not as a diagnosable disorder [19]. Further, while the term “addiction” is used loosely across studies, few researchers have sought to adapt the substance use disorder criteria for use in videogame research, which would allow direct comparisons between drug addiction and behavioral addiction. Thus, this study represents the first to compare primary measures of problematic videogame playing as well as to combine items across measures to map onto the current criteria for substance use disorder. As expected, the aggregated questionnaire, which we refer to as the VGAS, was the most compelling measure of videogame-related impairment, based on both psychometric analysis as well as criterion validity. These results partially support the criteria of Internet Gaming Disorder as outlined in the DSM-5; however, IGD appears to adapt the Gambling Disorder criteria and vernacular as opposed to utilizing a substance use conceptualization. Thus, additional research is needed to reproduce the current findings and to lend further support for an addictions model of problematic videogaming.
Although the current study has generated several important conclusions, future empirical endeavors can help solidify an addictions-based perspective of problematic videogame play. Specifically, validation of the VGAS within a clinical sample would help ensure that the current conceptualization of addiction is reflected in individuals seeking treatment for their impairment. Further, evaluation of a clinical sample would help determine if the VGAS is sensitive to clinical change. It would be anticipated that scores on the VGAS would drop in response to treatment or diminishment of symptomatology. Future studies that aim to identify common biological underpinnings of SUD, other addictive behavior, and PVGP will allow for a more encompassing understanding of the nature of PVGP and the extent to which it shares features in common with addictive disorders.
Appendix A
Videogame Addiction Scale (VGAS)
| |
Never |
|
Sometimes |
|
Often |
| 1) I play video games over a longer time period than I intended |
1 |
2 |
3 |
4 |
5 |
| 2) I have tried to play video games less often or for shorter periods of time, but was unsuccessful |
1 |
2 |
3 |
4 |
5 |
| 3) I spend an increasing amount of time playing video games |
1 |
2 |
3 |
4 |
5 |
| 4) When I am not playing video games, I am often planning how I will play my next game |
1 |
2 |
3 |
4 |
5 |
| 5) In order to play video games, I have skipped class or work |
1 |
2 |
3 |
4 |
5 |
| 6) In order to play video games, I get into arguments with people |
1 |
2 |
3 |
4 |
5 |
| 7) Because of my video game playing, I have spent less time with my friends and family |
1 |
2 |
3 |
4 |
5 |
| 8) Because of my video game playing, I have experienced headaches or my neck, wrist, hand(s), or back hurt |
1 |
2 |
3 |
4 |
5 |
| 9) I need to spend more and more time and/or money on video games in order to feel the same amount of excitement |
1 |
2 |
3 |
4 |
5 |
| 10) I become restless or irritable when attempting to cut down or stop playing video games |
1 |
2 |
3 |
4 |
5 |
References
- Entertainment Software Association (2012) Industry Facts
- Petry NM (2010) Pathological gambling and the DSM-V. International Gambling Studies, 10: 113-115.
- TolchinskyA&Jefferson SD (2011) Problematic video game play in a college sample and its relationship to time management skills and attention-deficit/hyperactivity disorder symptomology. CyberpsycholBehavSocNetw14: 489-496.
- Wood RTA (2008) Problems with the concept of video game "Addiction": Some case study examples. International Journal of Mental Health and Addiction 6: 169-178.
- Irvine MA, Worbe Y, Bolton S, Harrison NA, Bullmore ET, et al. (2013) Impaired decisional impulsivity in pathological videogamers. PLoS One 8: e75914.
- Walther B, Morgenstern M, Hanewinkel R (2012) Co-occurrence of addictive behaviours: personality factors related to substance use, gambling and computer gaming. Eur Addict Res 18: 167-174.
- Littel M, Berg I, Luijten M, Rooij AJ, Keemink L, et al. (2012) Error processing and response inhibition in excessive computer game players: an eventrelated potential study. Addict Biol17: 934-947.
- Petry NM, Rehbein F, Gentile DA, Lemmens JS, Rumpf HJ, et al. (2014) An international consensus for assessing internet gaming disorder using the new DSM-5 approach. Addiction 109: 1399-1406.
- King DL, Haagsma MC, Delfabbro PH, Gradisar M, Griffiths MD (2013)Toward a consensus definition of pathological video-gaming: A systematic review of psychometric assessment tools. ClinPsychol Rev 33: 331-342.
- Blaszczynski A (2008) Commentary: A response to Problems with the concept of video game addiction: Some case study examples. International Journal of Mental Health and Addiction 6: 179-181.
- Shaffer HJ, Hall MN, Vander Bilt J (2000) "Computer addiction": a critical consideration. Am J Orthopsychiatry 70: 162-168.
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
- Ko CH, Yen JY, Chen SH, Wang PW, Chen CS, et al. (2014) Evaluation of the diagnostic criteria of Internet gaming disorder in the DSM-5 among young adults in Taiwan. J Psychiatr Res 53:103-110
- Festl R, Scharkow M, Quandt T (2013) Problematic computer game use among adolescents, younger and older adults. Addiction 108: 592-599.
- Van Rooij AJ, Schoenmakers TM, Vermulst AA, Van den Eijnden RJ, Van de Mheen D (2011) Online video game addiction: identification of addicted adolescent gamers. Addiction 106: 205-212.
- King DL, Delfabbro PH (2013) Issues for DSM-5: video-gaming disorder? Aust N Z J Psychiatry 47: 20-22.
- Baer S, Saran K, Green DA (2012) Computer/gaming station use in youth: Correlations among use, addiction and functional impairment. Paediatr Child Health 17: 427-431.
- Kuss DJ (2013) Internet gaming addiction: current perspectives. Psychol Res BehavManag 6: 125-137.
- Petry NM, O'Brien CP (2013) Internet gaming disorder and the DSM-5. Addiction 108: 1186-1187.
- Starcevic V (2013) Video-gaming disorder and behavioural addictions. Aust N Z J Psychiatry 47: 285-286.
- Rehbein F, Kliem S, Baier, D., Moble, T, Petry NM (2015). Prevalence of internet gaming disorder in German adolescents: diagnostic contribution of the nine DSM-5 criteria in a statewide representative sample. Addiction 110: 842-851.
- Cho H, Kwon M, Choi JH, Lee SK, Choi JS, et al. (2014) Development of the Internet addiction scale based on the Internet Gaming Disorder criteria suggested in DSM-5. Addict Behav39: 1361-1366.
- Pontes HM, Király O, Demetrovics Z, Griffiths MD (2014) The conceptualisation and measurement of DSM-5 Internet Gaming Disorder: the development of the IGD-20 Test. PLoS One 9: e110137.
- Pontes HM&Griffiths MD (2015) Measuring DSM-5 internet gaming disorder: Development and validation of a short psychometric scale. Computers in Human Behavior 45: 137-143.
- Lemmens JS, Valkenburg PM, Gentile DA (2015) The Internet Gaming Disorder Scale. Psychol Assess 27: 567-582.
- Wood RTA, Gupta R, Derevensky JL, Griffiths M (2004) Video game playing and gambling in adolescents: Common risk factors. Journal of Child & Adolescent Substance Abuse 14: 77-100.
- King D, Delfabbro P, Griffiths M (2010) The convergence of gambling and digital media: implications for gambling in young people. J Gambl Stud 26: 175-187.
- Parke J & Griffiths MD (2007)The role of structural characteristics in gambling. In D. Smith, D. Hodgins, & R. Williams (Eds.), Research and measurement issues in gambling studies,New York: Elsevier 211-243.
- King DL, Delfabbro PH, Griffiths MD (2011) The role of structural characteristics in problematic video game play: An empirical study. International Journal of Mental Health and Addiction 9: 320-333.
- Goldstein RZ, Volkow ND (2002) Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am J Psychiatry 159: 1642-1652.
- Conner KR, Pinquart M, Duberstein PR (2008) Meta-analysis of depression and substance use and impairment among intravenous drug users (IDUs). Addiction 103: 524-534.
- Crawford LA, Novak KB (2013) The effects of public self-consciousness and embarrassability on college student drinking: evidence in support of a protective self-presentational model. J SocPsychol 153: 109-122.
- Wagner EF, Myers MG, McIninch JL (1999) Stress-coping and temptation-coping as predictors of adolescent substance use. Addict Behav 24: 769-779.
- Russell M, Cooper ML, Frone MR (1990)The influence of sociodemographic characteristics on familial alcohol problems: Data from a community sample. Alcohol ClinExp Res 14: 221-226.
- Tolchinsky A (2013)The development of a self-report questionnaire to measure problematic video game play and its relationship to other psychological phenomena. Unpublished Dissertation, Eastern Michigan University, Ypsilanti, MI.
- Gentile D (2009) Pathological video-game use among youth ages 8 to 18: a national study. PsycholSci 20: 594-602.
- Lortie CL, Guitton MJ (2013) Internet addiction assessment tools: dimensional structure and methodological status. Addiction 108: 1207-1216.
- Toce-Gerstein M, Gerstein DR, Volberg RA (2003) A hierarchy of gambling disorders in the community. Addiction 98: 1661-1672.
- Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M (1993) Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction 88: 791-804.
- Fiellin DA, Reid MC, O'Connor PG (2000) Screening for alcohol problems in primary care: a systematic review. Arch Intern Med 160: 1977-1989.
- Kahler CW, Strong DR, Read JP (2005)Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: The brief young adult alcohol consequences questionnaire. Alcohol ClinExp Res 29: 1180-1189.
- Kahler CW, Hustad J, Barnett NP, Strong DR, Borsari B (2008) Validation of the 30-day version of the Brief Young Adult Alcohol Consequences Questionnaire for use in longitudinal studies. J Stud Alcohol Drugs 69: 611-615.
- Lesieur HR &Blume SB (1987) The South Oaks Gambling Screen (The SOGS): A new instrument for the identification of pathological gamblers.Am J Psychiatry 144: 1184-1188.
- Kroenke K, Spitzer RL, Williams JB (2001) The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 16: 606-613.
- Patton JH, Stanford MS, Barratt ES (1995) Factor structure of the Barratt impulsiveness scale. J ClinPsychol 51: 768-774.
- Fenigstein A, Scheier MF, Buss AH (1975) Public and private self-consciousness: Assessment and theory. Journal of Consulting and Clinical Psychology 43: 522-527.
- Carver CS (1997) You want to measure coping but your protocol's too long: consider the brief COPE. Int J Behav Med 4: 92-100.
- Cattell RB (1966) The screen test for the number of factors. Multivariate Behavioral Research 1: 245-276.
- Kaiser HF (1960)The application of electronic computers to factor analysis. Educational and Psychological Measurement 20: 141-151.
- Horn Jl (1965) A Rationale and Test for the Number of Factors in Factor Analysis. Psychometrika 30: 179-185.
- Muthacn LK&Muthacn BO (2008)Mplus user guide. Los Angeles, CA: Author.
- Steiger JH (1990) Structural model evaluation and modification. Multivariate Behavioral Research 25: 214-212.
- Steiger JH & Lind JM (1980) Statistically-based tests for the number of common factors. Paper presented at the annual Spring Meeting of the Psychometric Society in Iowa City.
- Bentler PM (1990) Comparative fit indexes in structural models. Psychol Bull 107: 238-246.
- Bond CF & Richardson K (2004)Seeing the Fischer Z-formation. Psychometrika 69: 291-303.
- Bentler PM & Bonnet DC (1980) Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin 88: 588-606.
- Janreskog K &Sanrbom D (1993) LISREL 8: Structural equation modeling with the SIMPLIS command language. Chicago, IL: Scientific Software International Inc.
- Lawson AK, Wright CV, Fitzgerald LF (2013) The evaluation of sexual harassment litigants: reducing discrepancies in the diagnosis of posttraumatic stress disorder. Law Hum Behav 37: 337-347.
- Saha TD, Compton WM, Chou SP, Smith S, Ruan WJ, et al. (2012) Analyses related to the development of DSM-5 criteria for substance use related disorders. 1. Toward amphetamine, cocaine and prescription drug use disorder continua using item response theory. Drug Alcohol Depend 122: 38-46.
- Fulkerson JA, Harrison PA, Beebe TJ (1999) DSM-IV substance abuse and dependence: are there really two dimensions of substance use disorders in adolescents? Addiction 94: 495-506.
- Rounsaville BJ, Bryant K, Babor T, Kranzler H, Kadden R (1993) Cross system agreement for substance use disorders: DSM-III-R, DSM-IV and ICD-10. Addiction 88: 337-348.
- Nelson CB, RehmUstun TB, Grant B, Chatterji S (1999) Factor structures for DSM-IV substance disorder criteria endorsed by alcohol, cannabis, cocaine and opiate users: Results from the WHO reliability and validity study. Addiction 94: 843-855.
- Coffey SF, Gudleski GD, Saladin ME, Brady KT (2003) Impulsivity and rapid discounting of delayed hypothetical rewards in cocaine-dependent individuals. ExpClinPsychopharmacol11: 18-25.
- Ersche KD, Clark L, London M, Robbins TW, Sahakian BJ (2006) Profile of executive and memory function associated with amphetamine and opiate dependence. Neuropsychopharmacology 31: 1036-1047.
- Madden GJ, Petry NM, Badger GJ, Bickel WK (1997) Impulsive and self-control choices in opioid-dependent patients and non-drug-using control participants: Drug and monetary rewards. ExpClinPsychopharmacol5: 256-262.
- Verdejo-Garcia A& Perez-Garcia M (2007) Profile of executive deficits in cocaine and heroin polysubstance users: Common and differential effects on separate executive components. Psychopharmacology 190: 517-530.
- Mitchell JM, Fields HL, D'Esposito M, Boettiger CA (2005) Impulsive responding in alcoholics. Alcohol ClinExp Res 29: 2158-2169.
- Butler GK, Montgomery AM (2004) Impulsivity, risk taking and recreational 'ecstasy' (MDMA) use. Drug Alcohol Depend 76: 55-62.
- Morgan MJ (1998) Recreational use of "ecstasy" (MDMA) is associated with elevated impulsivity. Neuropsychopharmacology 19: 252-264.
- Fuentes D, Tavares H, Artes R, Gorenstein C (2006) Self-reported and neuropsychological measures of impulsivity in pathological gambling. J IntNeuropsycholSoc12: 907-912.
- Petry NM (2001) Substance abuse, pathological gambling, and impulsiveness. Drug Alcohol Depend 63: 29-38.
- Lee RM, Liu HT (2001)Coping with intergenerational family conflict: Comparison of Asian American, Hispanic, and European American college students. Journal of Counseling Psychology 48: 410-419.
- Stein JA, Dixon EL, Nyamathi AM (2008) Effects of psychosocial and situational variables on substance abuse among homeless adults. Psychol Addict Behav 22: 410-416.
- Eftekhari A, Turner AP, Larimer ME (2004) Anger expression, coping, and substance use in adolescent offenders. Addict Behav 29: 1001-1008.
- Mohamad MS (2009) Daily hassles, coping strategies, and substance use among Egyptian manufacturing workers. Journal of Muslim Mental Health 4: 17-29.
- Nowack KM&Pentkowski AM (1994) Lifestyle habits, substance use and predictors of job burnout in professional working women. Work & Stress 8: 19-35.
- Frone MR, Windle M (1997) Job dissatisfaction and substance use among employed high school students: the moderating influence of active and avoidant coping styles.Subst Use Misuse 32: 571-585.
- Simons RL & Robertson JF (1989)The impact of parenting factors, deviant peers, and coping style upon adolescent drug use. Family Relations 38: 273-281.
- Min M, Farkas K, Minnes S, Singer LT (2007) Impact of childhood abuse and neglect on substance abuse and psychological distress in adulthood. J Trauma Stress 20: 833-844.
- Van Rooij AJ, Meerkerk G, Schoenmakers TM, Griffiths M, Van de Mheen D (2010) Video game addiction and social responsibility. Addiction Research and Theory 18: 489-493.
- Hatsukami DK, Fischman MW (1996) Crack cocaine and cocaine hydrochloride. Are the differences myth or reality? JAMA 276: 1580-1588.
- Brower KJ, Hierholzer R, Maddahian E (1986)Recent trends in cocaine abuse in a VA psychiatric population. Hosp Community Psychiatry 37: 1229-1234.
- Khalsa HK, Anglin MD, Paredes A, Potepan P, Potter C (1993)Pretreatment natural history of cocaine addiction: Preliminary 1-year followup results. In F. M. Tims& C. G. Leukefeld (Eds.), Cocaine treatment research and clinical perspectives. Rockville, MD: US Dept. of Health and Human Services, 218-235.
- Miller NS, Gold MS (1994) Criminal activity and crack addiction. Int J Addict 29: 1069-1078.
- Pottieger AE, Tressell PA, Surratt HL, Inciardi JA, Citwood DD (1995) Drug use patterns of adult crack users in street versus residential treatment samples. J Psychoactive Drugs 27: 27-38.
- Whitbourne SK, Ellenberg S, Akimoto K (2013) Reasons for playing casual video games and perceived benefits among adults 18 to 80 years old. CyberpsycholBehavSocNetw 16: 892-897.

