Keywords
Aneurysm, False; Angiography; Hemorrhage; Pancreatic Pseudocyst; Splenectomy; Venous Thrombosis
Abbreviation
SVT: splenic vein thrombosis
INTRODUCTION
Most cases of pancreatitis are mild and selflimited. On the other hand, approximately one quarter of patients with pancreatitis may develop vascular complications. Vascular complications in pancreatitis are well recognized. Their exact incidence is not known. The most common complications are haemorrhage into a pseudocyst, erosions of the upper gastrointestinal arteries, thromboses of the portal venous system, formation of varices or pseudoaneurysms and rupture of a pseudoaneurysm. Pancreatitis in combination with vascular complications is dangerous and potentially lethal. The survival of patients with pancreatitis and vascular complications depends on the early diagnosis of these complications. This article focuses on the aetiology, presentation, recent developments in diagnosis and management of such complications.
Search Methods
To set the findings of the present study in the context of available evidence, a computerised literature search of PubMed, Embase, ISIS and CAS was carried out. The key words/subject headings used were “hemorrhage,” “pancreatitis,” “false aneurysms,” “venous thrombosis,” “angiography” and “therapeutic embolisation”. Limits applied were to restrict searches as follows: human and English language. All references were reviewed to retrieve additional articles. Other sources included review articles and text-books.
Haemorrhage
Haemorrhage is one of the most lifethreatening complications of pancreatitis [1, 2]. Haemorrhage is usually due to erosion of a major pancreatic or peripancreatic blood vessel or due to the formation and subsequent rupture of an arterial pseudoaneurysm [1]. The frequency of fatal haemorrhagic complications of pancreatitis varies between 1.2% and 14.5%, and these complications seem to be related to the severity of disease [3, 4, 5, 6, 7].
The pathogenesis of haemorrhagic complications is multifactorial. One of the factor is mediated by severe pancreatic inflammation and pancreatic necrosis which takes place during the early phase of acute pancreatitis. Local spread of the inflammatory process and extravasation of proteolytic and lipolytic enzymes further exacerbate the necrotizing process and initiate the damage of any vascular structure proximal to the necrotizing process, rendering them susceptible to rupture or subsequent pseudoaneurysm formation.
Haemorrhage tends to occur rather frequently in patients requiring operation for necrosectomy and debridement of infected pancreatic sequestra (sequestrectomy) [4, 5]. Kriwanek et al. showed that patients developed complications (including bleeding) more often after early operations than after delayed interventions (42.8% vs. 8.7%, respectively) [8]. Early operations do not allow a satisfactory debridement of the pancreatic and peripancreatic tissue as the necrosis is not well demarcated. During surgical intervention, an aggressive or traumatic technique may lead to vessel wall weakening and may expose it to further damage from activated enzymes or foreign bodies such as drains or dry gauze. Packing of the residual spaces after necrosectomy or sequestrectomy with gauze utilized in the open technique might expose the unprotected denuded vessels to injury during removal of the adherent gauze packing [9]. The long term placement of drains for postoperative lavage can lead to vessel wall weakening and rupture caused by the mechanical irritation exerted by the drains [5].
Another mechanism that may lead to severe haemorrhage is associated with the development of pancreatic and peripancreatic abscesses. This is more often observed weeks to months after the onset of a necrotizing form of severe pancreatitis or after necrosectomy and insufficient debridement. The combination of ischaemic necrosis, enzymatic destruction of tissues and bacterial contamination may lead to severe vessel damage as well as perforation of adjacent organs. In such events, bleeding can take place within the abscess cavity and from that to any other intra-abdominal or retroperitoneal space.
A third pathogenic mechanism is mediated by long-standing pseudocysts. Vessels may be eroded as a consequence of persistent compression, ischaemia, and elastolytic action of the enzymatic content of pseudocysts [4, 10, 11]. Frequently, these mechanisms can lead to the formation of pseudoaneurysms. Their rupture or a direct vessel rupture within a pseudocyst converts it into a pseudoaneurysmatic pseudocyst (pulsatile pseudocyst), which may eventually rupture in the retroperitoneum or peritoneal cavity or communicate with adjacent hollow structures such as the stomach, jejunum, colon, and Wirsung duct (haemosuccus pancreaticus).
A fourth pathogenic mechanism bleeding is caused by isolated obstruction of the splenic vein due to thrombosis from a necrotizing process and severe contiguous inflammation, abscess or pseudocysts. Splenic vein obstruction usually leads to left-sided portal hypertension, oesophagogastric variceal formation and eventual bleeding. In a series reported by Madsen et al., massive bleeding in the form of haematemesis and melena was observed in 72% of patients; 4 out of 13 (30%) bleeding patients treated conservatively without splenectomy died [12].
Pseudoaneurysms
The formation of pseudoaneurysms occurring as a result of pancreatitis is well established [10, 13, 14]. A pseudoaneurysm has been reported to occur in 3.5-10% of patients with pancreatitis [15]. The development of a pseudoaneurysm from vessel wall erosion by a pseudocyst is due to uncontrolled, severe inflammation necrotising the vessel [1]. It may also occur as a result of release of the pancreatic enzymes eroding the peripancreatic vessels, sometimes even vessels distant from the pancreas, to cross tissue planes and boundaries [16]. The intense inflammatory changes surrounding a pseudoaneurysm makes surgical control extremely challenging associated with a high morbidity and mortality [10].
The arteries involved include, in order of frequency, the splenic (40%), gastroduodenal (30%), pancreaticoduodenal (20%), gastric (5%), hepatic (2%), others (superior mesenteric, jejunal, ileocaecal, aorta) (1-3%) [16, 17, 18, 19, 20, 21]. Rupture of a pseudoaneurysm is a disastrous complication of pancreatitis. A pseudoaneurysm may rupture into a pseudocyst, the gastrointestinal tract, peritoneal cavity or pancreatic parenchyma [22, 23, 24]. Suzuki et al. reported a rare case wherein a pseudoaneurysm of the gastroduodenal artery ruptured into the superior mesenteric vein [18]. The size of the pseudoaneurysm is not a determinant of rupture [25].
Clinical Features
Patients may present with sudden exacerbation of severe abdominal pain, distension, and clinical signs of blood loss (tachycardia and hypotension) but also, more rarely, in the form of slow intermittent bleeding. Some patients may present with haematemesis or melena. In patients who have previously undergone operations for necrosectomy or debridement or have had abscesses drained, bleeding from drains is usually the earliest sign [11]. Flati et al. found that bleeding occurred as a sudden exsanguinating process in 7.5% of patients, leading to death in all patients within minutes or hours [5]. However, the diagnosis of acute haemorrhage is not always easy to diagnose particularly in patients with severe acute pancreatitis with multiple organ dysfunction.
Investigations
Although angiography is considered the gold standard, the initial imaging of these patients is usually helical computerised tomography (CT) scan, as angiography is not always available. The CT scan finding of contrast enhancement within or adjacent to a suspected pseudocyst is suspicious of a pseudoaneurysm. The enhancement may be similar to that of the abdominal aorta. The finding of increased attenuation within a fluid collection on a non-enhanced scan may indicate recent haemorrhage [26].
Superior mesenteric angiography has been shown to be effective in localizing the bleeding site and control the bleeding [4, 5, 10, 17, 27, 28]. Angiography should be utilized in all patients, if possible, to show the precise site and source of bleeding [29]. In some instances angiography may fail to demonstrate bleeding, which may be due to venous bleeding, intermittent arterial bleeding or bleeding from a large surface area. Colour Doppler ultrasonography and magnetic resonance imaging (MRI) may be helpful in visualizing pseudoaneuryms, thrombotic vessels, necrotic areas, abscess cavities and extension of the inflammatory process [5].
Suzuki et al. recommend that abdominal colour Doppler ultrasound be performed at regular intervals in patients with chronic pancreatitis to prevent delay in the diagnosis and management of a pseudoaneurysm [18]. However, a thrombus within the pseudoaneurysm may result in negative findings at colour Doppler ultrasound scan therefore, such findings should not preclude contrast-enhanced CT scan and angiography [30].
Treatment
Immediate surgery is the gold standard if the patient is haemodynamically unstable. Patients who are haemodynamically stable and who have angiographic evidence of bleeding can be treated with transcatheter embolization. This may result in permanent control of the bleeding thereby providing definitive treatment. Patients who are unstable or who have vascular involvement that is not amenable to transcatheter embolization should have emergency surgery [14]. Preoperative angiography should be performed prior to surgery, if possible. Angiography can show the surgeon the exact vessel involved, as well as the surrounding vascular anatomy, thus facilitating the surgical approach. In selected patients, occlusion balloon catheters can be employed to obtain haemostasis during or after pancreatic surgery. Recently, percutaneous injection of thrombin into the sac of pseudoaneurysms have been shown to be effective in the treatment of this condition [31, 32, 33, 34].
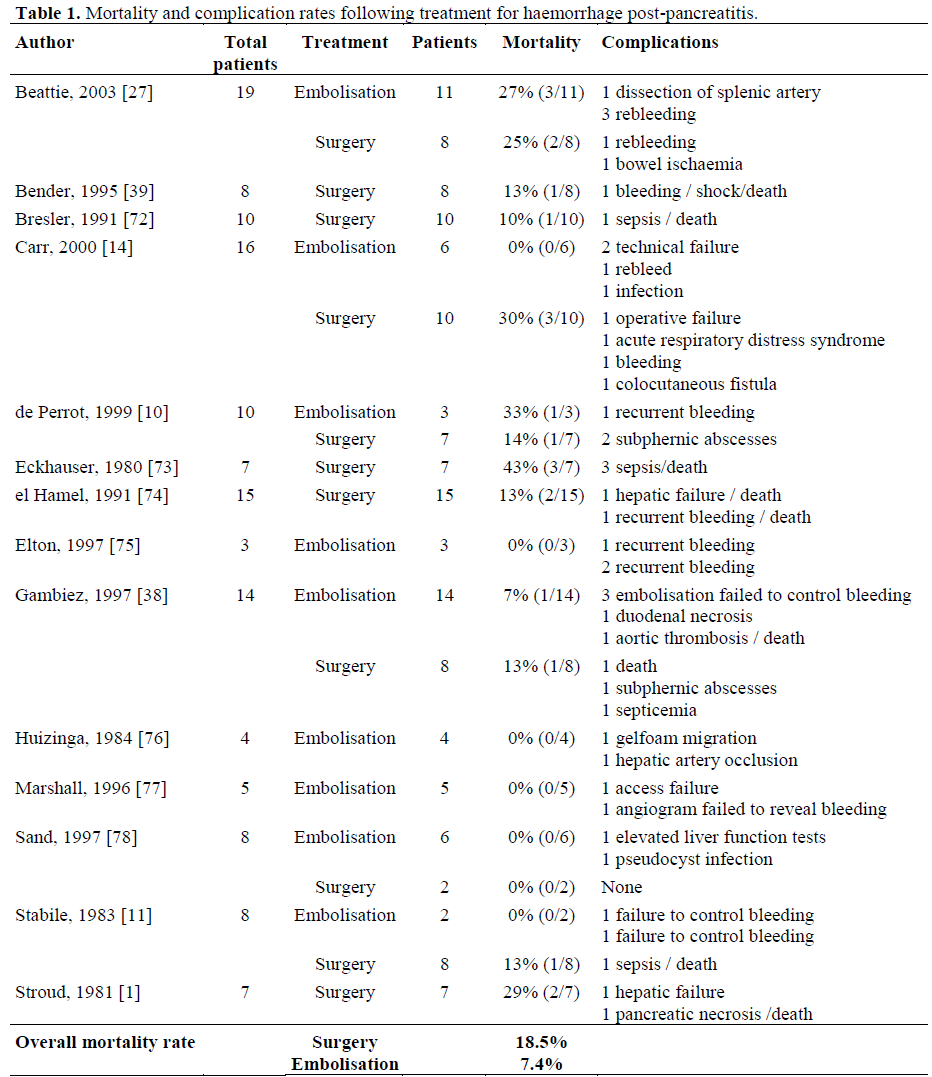
The success rates of transcatheter embolisation have varied over the years, with the initial reports citing a significant number of rebleeds (Table 1). As the past decade progressed, the success rates began to show a great deal of improvement [35]. This is attributed to improved design of catheters, embolic material technology and to the improvement in technical expertise [35, 36]. The earliest problems associated with transcatheter control of bleeding in pancreatitis was the inability to reach the small and tortuous target vessels with the large calibre catheters that were available. Micro-catheters, primarily designed for use for embolisation in the cerebral vessels, were then adapted for visceral arteries. It was with the aid of these catheters that even the small intra pancreatic arteries could be catheterised and embolic material delivered.
Along with the development of the catheters, came an understanding about the techniques involved in successful embolisation in pancreatitis. Due to the excellent collateral circulation around the pancreas, it is essential to occlude the artery proximal and distal to the arterial pathology, failing which the artery can refill and the bleeding will not cease. If the vessel is severely involved , additional liquid embolic material such as glue could be used for effective embolisation [37]. The expertise of the interventional radiologist plays an important role in suspecting this potential problem and addressing it immediately [38].
The most common surgical procedure is suture ligation of the bleeding point; however, this procedure results in a high recurrence of bleeding [11]. The bleeding vessel should be identified and ligated proximally and distally whenever possible [39, 40]. This may be impossible to perform in a pancreas with a severe necrotizing process [5]. Proximal or distal pancreatic resections may occasionally be needed, however they can be successfully performed only when bleeding occurs in patients who have already recovered from acute pancreatitis [28]. Primary resection of the pseudoaneurysm with pancreatic resection is required in some cases with pseudoaneurysms [10]. Table 1 shows the complication rates of surgery and embolisation in different studies
Splenic Vein Thrombosis (SVT)
Isolated splenic vein thrombosis (SVT) is relatively common in patients with chronic pancreatitis, occurring in as many as 10-40% of cases [41]. Although much less common, portal and superior mesenteric vein thrombosis can also occur as a result of pancreatitis [42].
Pathophysiology
The pathogenesis of SVT is related to the close proximity of the splenic vein to pancreas [41]. There are three factors that can lead to the development of SVT.
1. Secondary involvement of the vein by the surrounding oedema, cellular infiltration, and the inflammatory process of chronic pancreatitis, particularly with calcified pancreas [43, 44, 45].
2. Compression by a pseudocyst or enlarged pancreatic parenchyma; pseudocysts of the caudal pancreas are complicated by splenicvein obstruction in nearly 30% of cases [41].
3. Intimal injury and venous thrombosis, especially when SVT is due to acute pancreatitis or recurrent episodes of pancreatitis.
In either the intrinsic or extrinsic mechanisms stasis of blood flow occurs and eventually leads to thrombosis [46].
The splenic artery remains intact and thus enables continued high pressure in the spleen, which forces an abnormal outlet through collaterals [47]. Therefore, regardless of the mechanism of SVT, venous blood is forced to return to low pressure systems via collaterals [44]. Increased blood flow through the short gastric veins to the coronary vein or through the gastroepiploic vein to the pancreaticoduodenal vein creates a localized form of "left-sided" portal hypertension with dilatation of the submucosal veins within the stomach wall, producing the formation of gastric varices along the greater curvature and the fundus of the stomach [44, 46]. A second pathway involves the portosystemic collaterals, which develop along the lower end of the oesophagus, with direct connection to the azygous system [48]. Because portal venous pressure is normal and oesophageal veins can usually drain through the patent coronary vein, the development of associated oesophageal varices is prevented [44, 49, 50]. However, sometimes combined oesophageal and gastric varices are observed in sinistral portal hypertension and even isolated oesophageal varices without gastric varices [49].
Clinical Features
SVT may be silent or present with symptoms [51]. Gastrointestinal bleeding of various severities (anaemia, haematemesis, melena, or haematochezia) is the commonest manifestation of the syndrome (15-50%) [52, 53, 54]. Splenomegaly is a frequent accompaniment of SVT [51]. Occasionally, manifestations of congestive splenomegaly such as thrombocytopenia or pancytopenia and abdominal pain are present [51]. As this syndrome occurs in the absence of cirrhosis, there are no stigmata of chronic liver disease.
Investigations
As SVT is asymptomatic in the majority of cases, diagnosis may be difficult. Abdominal CT scan is very helpful in the diagnosis of SVT. The findings on CT scan are: extensive, irregular, enhancing vessels around the splenic vein (short gastric veins in the gastrosplenic ligament, dilated gastroepiploic or coronary vein) or a vein with a centre of lower attenuation which does not enhance after intravenous injection of contrast material [55]. The identification of an enlarged left gastroepiploic vein, without a recanalised umbilical vein, strongly suggests a diagnosis of SVT and not portal hypertension and is therefore useful for the differential diagnosis between these two vascular complications; this distinction is important, since their treatment differs totally [56]. In addition, the presence of normally enhanced portal and superior mesenteric veins supports the diagnosis of SVT [57]. Dynamic CT with bolus injections can detect SVT with a sensitivity of 71% [58].
As upper gastrointestinal bleeding is the commonest clinical manifestation of SVT, upper gastrointestinal endoscopy is the diagnostic method of choice to ascertain the source of haemorrhage [51]. Patients with chronic pancreatitis have many potential sources of bleeding (most commonly peptic ulcer). Endoscopy is indicated even in asymptomatic patients with SVT found incidentally, to show the presence and extent of varices [46]. It should be noted that the barium meal often misses the gastric varices and therefore this should not be relied on to diagnose varices in patients with known or suspected SVT [48].
Angiography with venous phase (preferentially selective intra-arterial digital splenic angiography) is the gold standard technique for diagnosing SVT [59]. The angiographic features of SVT are well described by Cho and Martel [60]: 1) focal or complete non-opacification of the splenic vein despite filling of splenic hilar and parenchymal veins; 2) filling of collateral channels of venous drainage (gastric, gastroesophageal, or omental varices); and 3) patency of the portal vein with filling via the splenic vein collaterals. Ultrasonography (with or without colour Doppler) [61, 62, 63], MRI [64, 65] and endoscopic ultrasound [66, 67] are now available as non-invasive techniques for the diagnosis of SVT.
Treatment
Many patients with SVT develop silent collaterals without gastric or gastrooesophageal varices. These patients are very unlikely to bleed. Therefore, asymptomatic patients without gastric or gastro-oesophageal varices should be observed [58]. In other words, SVT per se is not considered an indication for prophylactic splenectomy [44, 46]. Observation should be focused on the possibility of varices formation, which may be complicated by upper gastrointestinal bleeding. However, later varices formation is unlikely if they were not present at the time of diagnosis of SVT [51].
Splenectomy is the treatment of choice in symptomatic patients and is highly effective [41]. Removal of the spleen decreases the venous outflow by way of the collaterals and decompresses the associated varices by cutting off inflow, thereby preventing further haemorrhage [46]. Splenectomy can be performed during pancreatic surgical procedures such as distal pancreatectomy or lateral pancreaticojejunostomy, which is frequently indicated for the treatment of underlying chronic pancreatitis [46, 68].
Whereas splenectomy is clearly indicated in SVT, the role of prophylactic splenectomy in patients with asymptomatic SVT associated with gastric or gastro-oesophageal varices remains controversial. Bradley [44], on the basis of long-term observations, concluded that the long-term risk of bleeding in patients with SVT and significant varices exceeds the risk of elective splenectomy with possible postsplenectomy sepsis and that in
asymptomatic patients with gastric or gastrooesophageal varices, prophylactic splenectomy may be useful. However, Bernades et al. disagree about the role of prophylactic splenectomy in these patients [41]. The study of Sakorafas et al. at the Mayo Clinic, which included 34 patients with SVT complicating chronic pancreatitis, support the strategy of concomitant prophylactic splenectomy in patients undergoing operative treatment of symptomatic chronic pancreatitis if sinistral portal hypertension associated with gastric or gastro-oesophageal varices is also present [69]. Although most patients remain totally asymptomatic until the onset of haemorrhage [48], variceal bleeding may be life threatening [52, 53, 54]. The risk of variceal bleeding appears to be greater in large varices and when red wale markings are observed during endoscopy [70]. However, it should be emphasized that there is no absolute way of accurately predicting the risk of variceal haemorrhage and therefore the possibility of this dangerous complication cannot be excluded with certainty.
SVT may frequently complicate pancreatic surgery because of extensive intra-operative blood loss from collateral circulation [51]. Preoperative recognition of SVT, even if asymptomatic, is important when operation is being considered for chronic pancreatitis or its complications, since it may significantly alter treatment options [46]. Alternatively, the splenic artery may be ligated away from the hilum at the upper border of the pancreas (supragastric approach to control the proximal splenic artery), provided the associated chronic pancreatitis does not prevent this from being done safely [51].
The distinction between generalized portal hypertension and sinistral (left-sided) segmental portal hypertension secondary to SVT is very important [52]. Whereas, in generalised portal hypertension the treatment of choice is a shunt procedure. In sinistral hypertension secondary to SVT portosystemic shunting fails to decompress the gastric or oesophageal-gastric varices , may be associated with severe complications (such as encephalopathy and delayed hepatic failure), and is therefore contraindicated [52, 71]. When the two conditions coexist, splenectomy should be considered in addition to a shunt procedure [7, 52]. Percutaneous splenic artery embolization is an alternative often referred to as "non-surgical splenectomy" [46, 50]. The inability to treat coexisting pancreatic disease and the possibility of the formation of a splenic abscess make this a less than optimal alternative [46, 50]. Currently, the role of transcatheter embolization should be as a planned first stage of a two-stage therapy (embolisation followed by splenectomy). Preoperative splenic artery embolisation occludes the splenic artery and reduces the left upper quadrant varices; this can greatly facilitate subsequent surgery [50]. Embolisation without splenectomy may be reserved for patients who are haemodynamically unstable despite supportive therapy and for high-risk patients who are unlikely to survive operation [46, 48, 50].
Conclusion
Although the vascular complications following pancreatitis are not very common, they should be considered in every patient with pancreatitis. These complications if diagnosed and managed early will result in considerable reduction of morbidity and mortality.
References
- Stroud WH, Cullom JW, Anderson MC. Hemorrhagic complications of severe pancreatitis. Surgery 1981; 90:657-65. [PMID 6974412]
- Vujic I. Vascular complications of pancreatitis. Radiol Clin North Am 1989; 27:81-91. [PMID 2642279]
- Bittner R. Surgical management of pancreatic abscess. In: Beger H, Warshaw AL, Buchler M, eds. The Pancreas. Oxford, United Kingdom: Blackwell Science, 1998:627-31.
- Flati G, Salvatori F, Porowska B, Talarico C, Flati D, Proposito D, et al. Severe hemorrhagic complications in pancreatitis. Ann Ital Chir 1995; 66:233-7. [PMID 7668500]
- Flati G, Andren-Sandberg A, La Pinta M, Porowska B, Carboni M. Potentially fatal bleeding in acute pancreatitis: pathophysiology, prevention, and treatment. Pancreas 2003; 26:8-14. [PMID 12499910]
- Frey CF. Hemorrhagic pancreatitis. Am J Surg 1979; 137:616-23. [PMID 453456]
- Warshaw AL, Jin GL. Improved survival in 45 patients with pancreatic abscess. Ann Surg 1985; 202:408-17. [PMID 4051596]
- Kriwanek S, Gschwantler M, Beckerhinn P, Armbruster C, Roka R. Complications after surgery for necrotising pancreatitis: risk factors and prognosis. Eur J Surg 1999; 165:952-7. [PMID 10574103]
- Tsiotos GG, Munoz Juarez MM, Sarr MG. Intraabdominal hemorrhage complicating surgical management of necrotizing pancreatitis. Pancreas 1996; 12:126-30. [PMID 8720657]
- de Perrot M, Berney T, Buhler L, Delgadillo X, Mentha G, Morel P. Management of bleeding pseudoaneurysms in patients with pancreatitis. Br J Surg 1999; 86:29-32. [PMID 10027355]
- Stabile BE. Hemorrhagic complications of pancreatitis and pancreatic pseudocysts. In: Beger H, Warshaw AL, Buchler M, eds. The Pancreas. Oxford, United Kingdom: Blackwell Science, 1998:606-13.
- Madsen MS, Petersen TH, Sommer H. Segmental portal hypertension. Ann Surg 1986; 204:72-7. [PMID 3729585]
- Burke JW, Erickson SJ, Kellum CD, Tegtmeyer CJ, Williamson BR, Hansen MF. Pseudoaneurysms complicating pancreatitis: detection by CT. Radiology 1986; 161:447-50. [PMID 3763917]
- Carr JA, Cho JS, Shepard AD, Nypaver TJ, Reddy DJ. Visceral pseudoaneurysms due to pancreatic pseudocysts: rare but lethal complications of pancreatitis. J Vasc Surg 2000; 32:722-30. [PMID 11013036]
- White AF, Baum S, Buranasiri S. Aneurysms secondary to pancreatitis. Am J Roentgenol 1976; 127:393-6. [PMID 183522]
- Woods MS, Traverso LW, Kozarek RA, Brandabur J, Hauptmann E. Successful treatment of bleeding pseudoaneurysms of chronic pancreatitis. Pancreas 1995; 10:22-30. [PMID 7899456]
- Boudghene F, L'Hermine C, Bigot JM. Arterial complications of pancreatitis: diagnostic and therapeutic aspects in 104 cases. J Vasc Interv Radiol 1993; 4:551-8. [PMID 8353353]
- Suzuki T, Ishida H, Komatsuda T, Oyake J, Miyauchi T, Heianna J, Miyashita M. Pseudoaneurysm of the gastroduodenal artery ruptured into the superior mesenteric vein in a patient with chronic pancreatitis. J Clin Ultrasound 2003; 31:278-82. [PMID 12767023]
- Toscano RL, Ruiz OR, Gerace CA Jr. Rupture of splenic artery pseudoaneurysm. Am Surg 1995; 61:940-2. [PMID 7486420]
- Yeh TS, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen MF. Massive extra-enteric gastrointestinal hemorrhage secondary to splanchnic artery aneurysms. Hepatogastroenterology 1997; 44:1152-6. [PMID 9261616]
- Giles RA, Pevec WC. Aortic pseudoaneurysm secondary to pancreatitis. J Vasc Surg 2000; 31:1056- 9. [PMID 10805901]
- Dinu F, Deviere J, Van Gossum A, Golzarian J, Dussaussois L, Delhaye M, Cremer M. The wirsungorrhagies: causes and management in 14 patients. Endoscopy 1998; 30:595-600. [PMID 9826136]
- Kuganeswaran E, Smith OJ, Goldman ML, Clarkston WK. Hemosuccus pancreaticus: rare complication of chronic pancreatitis. Gastrointest Endosc 2000; 51:464-5. [PMID 10744821]
- MacMahon MJ. Acute pancreatitis. In: Misiewicz JJ, Pounder RE, Venables CW, eds. Diseases of the Gut and Pancreas. London, United Kingdom: Blackwell Scientific, 1994:411.
- Tessier DJ, Stone WM, Fowl RJ, Abbas MA, Andrews JC, Bower TC, et al. Clinical features and management of splenic artery pseudoaneurysm: case series and cumulative review of literature. J Vasc Surg 2003; 38:969-74. [PMID 14603202]
- Balthazar EJ, Fisher LA. Hemorrhagic complications of pancreatitis: radiologic evaluation with emphasis on CT imaging. Pancreatology 2001; 1:306-13. [PMID 12120209]
- Beattie GC, Hardman JG, Redhead D, Siriwardena AK. Evidence for a central role for selective mesenteric angiography in the management of the major vascular complications of pancreatitis. Am J Surg 2003; 185:96- 102. [PMID 12559436]
- McMahon MJ, Playforth MJ, Hill GL. The management of haemorrhagic complications of pseudocysts and abscesses of the pancreas. Aust N Z J Surg 1980; 50:141-6. [PMID 6770804]
- Adams DB, Zellner JL, Anderson MC. Arterial hemorrhage complicating pancreatic pseudocysts: role of angiography. J Surg Res 1993; 54:150-6. [PMID 8479174]
- Kahn LA, Kamen C, McNamara MP Jr. Variable color Doppler appearance of pseudoaneurysm in pancreatitis. AJR Am J Roentgenol 1994; 162:187-8. [PMID 8273662]
- Armstrong EM, Edwards A, Kingsnorth AN, Freeman S, Roobottom CA. Ultrasound guided thrombin injection to treat a pseudoaneurysm secondary to chronic pancreatitis. Eur J Vasc Endovasc Surg 2003; 26:448-9. [PMID 14512011]
- Manazer JR, Monzon JR, Dietz PA, Moglia R, Gold M. Treatment of pancreatic pseudoaneurysm with percutaneous transabdominal thrombin injection. J Vasc Surg 2003; 38:600-2. [PMID 12947284]
- Puri S, Nicholson AA, Breen DJ. Percutaneous thrombin injection for the treatment of a postpancreatitis pseudoaneurysm. Eur Radiol 2003; 13(Suppl 4):L79-82. [PMID 15018170]
- Sparrow P, Asquith J, Chalmers N. Ultrasonicguided percutaneous injection of pancreatic pseudoaneurysm with thrombin. Cardiovasc Intervent Radiol 2003; 26:312-5. [PMID 14562987]
- Stosslein F, Zimmermann L, Bulang T. Embolization treatment of bleeding complications in pancreatitis. J Hepatobiliary Pancreat Surg 1998; 5:344-7. [PMID 9880786]
- Steckman ML, Dooley MC, Jaques PF, Powell DW. Major gastrointestinal hemorrhage from peripancreatic blood vessels in pancreatitis. Treatment by embolotherapy. Dig Dis Sci 1984; 29:486-97. [PMID 6609804]
- Yamakado K, Nakatsuka A, Tanaka N, Takano K, Matsumura K, Takeda K. Transcatheter arterial embolization of ruptured pseudoaneurysms with coils and n-butyl cyanoacrylate. J Vasc Interv Radiol 2000; 11:66-72. [PMID 10693716]
- Gambiez LP, Ernst OJ, Merlier OA, Porte HL, Chambon JP, Quandalle PA. Arterial embolization for bleeding pseudocysts complicating chronic pancreatitis. Arch Surg 1997; 132:1016-21. [PMID 9301616]
- Bender JS, Bouwman DL, Levison MA, Weaver DW. Pseudocysts and pseudoaneurysms: surgical strategy. Pancreas 1995; 10:143-7. [PMID 7716138]
- Schecter LM, Gordon HE, Passaro E Jr. Massive hemorrhage from the celiac axis in pancreatitis. Am J Surg 1974; 128:301-5. [PMID 4546386]
- Bernades P, Baetz A, Levy P, Belghiti J, Menu Y, Fekete F. Splenic and portal venous obstruction in chronic pancreatitis. A prospective longitudinal study of a medical-surgical series of 266 patients. Dig Dis Sci 1992; 37:340-6. [PMID 1735356]
- Rattner DW, Warshaw AL. Venous, biliary, and duodenal obstruction in chronic pancreatitis. Hepatogastroenterology 1990; 37:301-6. [PMID 2197206]
- Ammann RW, Akovbiantz A, Largiader F, Schueler G. Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medicalsurgical series of 245 patients. Gastroenterology 1984; 86:820-8. [PMID 6706066]
- Bradley EL III. The natural history of splenic vein thrombosis due to chronic pancreatitis: indications for surgery. Int J Pancreatol 1987; 2:87-92. [PMID 3500243]
- Lankisch PG. The spleen in inflammatory pancreatic disease. Gastroenterology 1990; 98:509-16. [PMID 2403954]
- Lillemoe KD, Yeo CJ. Management of complications of pancreatitis. Curr Probl Surg 1998; 35:1-98. [PMID 9462408]
- Khan AH, O'Reilly CJ, Avakian VA, Lucina PA. Splenic vein thrombosis: an unusual case of gastric bleeding. Angiology 1977; 28:725-7. [PMID 303066]
- Evans GR, Yellin AE, Weaver FA, Stain SC. Sinistral (left-sided) portal hypertension. Am Surg 1990; 56:758-63. [PMID 2268102]
- Little AG, Moossa AR. Gastrointestinal hemorrhage from left-sided portal hypertension. An unappreciated complication of pancreatitis. Am J Surg 1981; 141:153-8. [PMID 6970001]
- McDermott VG, England RE, Newman GE. Case report: bleeding gastric varices secondary to splenic vein thrombosis successfully treated by splenic artery embolization. Br J Radiol 1995; 68:928-30. [PMID 7551796]
- Sakorafas GH, Tsiotou AG. Splenic-vein thrombosis complicating chronic pancreatitis. Scand J Gastroenterol 1999; 34:1171-7. [PMID 10636062]
- Yale CE, Crummy AB. Splenic vein thrombosis and bleeding esophageal varices. JAMA 1971; 217:317-20. [PMID 5314826]
- Johnston FR, Myers RT. Etiologic factors and consequences of splenic vein obstruction. Ann Surg 1973; 177:736-9. [PMID 4541094]
- Burbige EJ, Tarder G, Carson S, Eugene J, Frey CF. Colonic varices. A complication of pancreatitis with splenic vein thrombosis. Am J Dig Dis 1978; 23:752-5. [PMID 685944]
- Belli AM, Jennings CM, Nakielny RA. Splenic and portal venous thrombosis: a vascular complication of pancreatic disease demonstrated on computed tomography. Clin Radiol 1990; 41:13-6. [PMID 2297961]
- Marn CS, Edgar KA, Francis IR. CT diagnosis of splenic vein occlusion: imaging features, etiology and clinical manifestations. Abdom Imaging 1995; 20:78- 81. [PMID 7894307]
- Mauro MA, Schiebler ML, Parker LA, Jaques PF. The spleen and its vasculature in pancreatitis: CT findings. Am Surg 1993; 59:155-9. [PMID 8476152]
- Hofer BO, Ryan JA Jr, Freeny PC. Surgical significance of vascular changes in chronic pancreatitis. Surg Gynecol Obstet 1987; 164:499-505. [PMID 3589904]
- Illig KA, Spitzer RM, Oates TK. Optimal diagnosis of splenic vein thrombosis: brief clinical report. Am Surg 1997; 63:1005-6. [PMID 9358791]
- Cho KJ, Martel W. Recognition of splenic vein occlusion. AJR Am J Roentgenol 1978; 131:439-43. [PMID 98986]
- Komatsuda T, Ishida H, Konno K, Hamashima Y, Ohnami Y, Naganuma H, et al. Color Doppler findings of gastrointestinal varices. Abdom Imaging 1998; 23:45-50. [PMID 9437062]
- Perisic-Savic M, Colovic R, Milosavljevic T, Ivanovic L. Splenic vein thrombosis. Diagnosed with Doppler ultrasonography. Hepatogastroenterology 1991; 38:557-60. [PMID 1778591]
- Weinberger G, Mitra SK, Yoeli G. Ultrasound diagnosis of splenic vein thrombosis. J Clin Ultrasound 1982; 10:345-6. [PMID 6815237]
- Levy HM, Newhouse JH. MR imaging of portal vein thrombosis. AJR Am J Roentgenol 1988; 151:283-6. [PMID 3293373]
- Taylor CR, McCauley TR. Magnetic resonance imaging in the evaluation of the portal venous system. J Clin Gastroenterol 1992; 14:268-73. [PMID 1564304]
- Lewis JD, Faigel DO, Morris JB, Siegelman ES, Kochman ML. Splenic vein thrombosis secondary to focal pancreatitis diagnosed by endoscopic ultrasonography. J Clin Gastroenterol 1998; 26:54-6. [PMID 9492865]
- Wiersema MJ, Wiersema LM. Endosonography of the pancreas: normal variation versus changes of early chronic pancreatitis. Gastrointest Endosc Clin N Am 1995; 5:487-96. [PMID 7582575]
- Haff RC, Page CP, Andrassy RJ, Buckley CJ. Splenectomy: its place in operations for inflammatory disease of the pancreas. Am J Surg 1977; 134:555-7. [PMID 920879]
- Sakorafas GH, Sarr MG, Farley DR, Farnell MB. The significance of sinistral portal hypertension complicating chronic pancreatitis. Am J Surg 2000; 179:129-33. [PMID 10773149]
- Trudeau W, Koffila R. Gastrointestinal Manifestations of Portal Hypertension. Gastrointestinal Diseases, an Endoscopic Approach. Volume 1. Oxford, United Kingdom: Blackwell Science, 1997:424-45.
- Salam AA, Warren WD, Tyras DH. Splenic vein thrombosis: a diagnosable and curable form of portal hypertension. Surgery 1973; 74:961-72. [PMID 4542994]
- Bresler L, Boissel P, Grosdidier J. Major hemorrhage from pseudocysts and pseudoaneurysms caused by chronic pancreatitis: surgical therapy. World J Surg 1991; 15:649-52. [PMID 1949866]
- Eckhauser FE, Stanley JC, Zelenock GB, Borlaza GS, Freier DT, Lindenauer SM. Gastroduodenal and pancreaticoduodenal artery aneurysms: a complication of pancreatitis causing spontaneous gastrointestinal hemorrhage. Surgery 1980; 88:335-44. [PMID 6968101]
- el Hamel A, Parc R, Adda G, Bouteloup PY, Huguet C, Malafosse M. Bleeding pseudocysts and pseudoaneurysms in chronic pancreatitis. Br J Surg 1991; 78:1059-63. [PMID 1933185]
- Elton E, Howell DA, Amberson SM, Dykes TA. Combined angiographic and endoscopic management of bleeding pancreatic pseudoaneurysms. Gastrointest Endosc 1997; 46:544-9. [PMID 9434224]
- Huizinga WK, Kalideen JM, Bryer JV, Bell PS, Baker LW. Control of major haemorrhage associated with pancreatic pseudocysts by transcatheter arterial embolization. Br J Surg 1984; 71:133-6. [PMID 6607086]
- Marshall GT, Howell DA, Hansen BL, Amberson SM, Abourjaily GS, Bredenberg CE. Multidisciplinary approach to pseudoaneurysms complicating pancreatic pseudocysts. Impact of pretreatment diagnosis. Arch Surg 1996; 131:278-83. [PMID 8611093]
- Sand JA, Seppanen SK, Nordback IH. Intracystic hemorrhage in pancreatic pseudocysts: initial experiences of a treatment protocol. Pancreas 1997; 14:187-91. [PMID 9057192]

