Keywords
Canada; Neoplasms; Second Primary; Nova Scotia; Palliative Care; Pancreatic Neoplasm
Abbreviations
ICD-O-3 International classification of disease for oncology, 3rd edition; NSCR Nova Scotia cancer registry; PC pancreatic cancer
INTRODUCTION
Pancreatic adenocarcinoma (PC) represents the fourth leading cause of cancer-related deaths in Canada [1]. The vast majority of patients are incurable at the time of diagnosis [2] and palliative chemo or chemoradiation therapy remain their only treatment options [3]. There is growing evidence that a significant proportion of PC patients do not receive chemotherapy, either for adjuvant purpose or for palliation [4, 5, 6, 7]. As a result, PC has the lowest rates of cancer-directed therapy out of all solid tumors [8]. This represents a modifiable factor that contributes to the poor prognosis of these patients [9].
In Canada, there continues to be a paucity of studies on factors that might be responsible for the low rate of cancer-directed therapy for PC patients [10, 11]. Therefore, primary aim of this study was to assess the management of pancreatic adenocarcinoma in Nova Scotia and the proportion of patients with PC who were referred to medical oncology specialists. Secondary outcomes were to assess if there was an increasing utilization of medical oncology resources over time and to explore if there were clinical and socio-demographic factors associated with medical oncology consultations.
METHODS
Patients Selection
The study population included a cohort of all patients older than 18 years of age who had the diagnosis of primary pancreatic cancers (PC) in the province of Nova Scotia, Canada over a ten-year period (April 1, 2001-March 31, 2011). Diagnostic codes of the International Classification of Disease for Oncology, 3rd edition (ICD-O-3) were used to select patients with PC from NSCR, a prospectively maintained database of all patients affected by malignant diseases in Nova Scotia and required by provincial law. Diagnostic codes of malignancies of the exocrine pancreas used for this study are summarized in Table 1. Each patient who satisfied the inclusion criteria was assigned an identification (ID) number to protect patients’ privacy. Additional administrative datasets were linked to the NSCR for completion of socio-demographic and clinical data as represented in Figure 1. Linked datasets included the Oncology Patient Information System (OPIS), Medical Service Insurance (MSI) Physician Services, Medical Service Insurance (MSI) Patient Registry, and the Canadian Institutes of Health Information (CIHI) Discharge Abstract Database (DAD) [12]. These datasets were linked to the NSCR by the Population Health Research Unit (PHRU) at Dalhousie University. The methodology used to link these administrative datasets has been described in details in previous manuscripts published by our group.
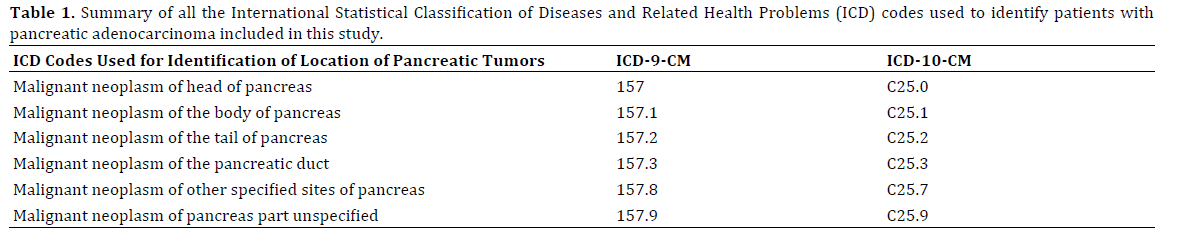
Figure 1. Schematic representation on how all the administrative database linkage was obtained to identify all the individuals affected by pancreatic cancer in Nova Scotia during the period between January 1, 2001 and December 31, 2011. Legend: NSCR (Nova Scotia Cancer Registry), HCN (Health Care Number), CHRD (Capital Health Radiology Department), PHRU (Population Health Research Unit, Dalhousie University).
Data on medical and radiation oncology referrals and consultations were captured using OPIS registry in the interval of time between 3 months prior to and 6 months after the date of diagnosis. Similarly, surgical referrals were captured using MSI billing codes for consultation with a surgeon within 3 months prior to diagnosis and 6 months after diagnosis. Comorbidity index for administrative databases developed by Elixhauser et al. was used to identify patients affected by comorbidities in addition to PC [13]. Median geographical census income data obtained from Canadian Statistics [14, 15] were used as a marker for patients’ socioeconomic status, with incomes divided into quintiles for statistical analysis.
The study protocol (CDHA-RS/2012-206) was approved by all the ethic review boards at each health district where patients received their treatment in the province of Nova Scotia and the investigators ensured adherence to confidentiality and safe storage of patients’ information.
STATISTICAL ANALYSIS
Variables analysed in this study included sociodemographic, clinical, oncologic and administrative characteristics. Sociodemographic variables were patients’ age and sex while clinical characteristics were patients’ comorbidity score, rate of referral to surgical specialists and rate of surgical interventions, rate of medical and radiation oncology consultations and percentage of patients who received cancer directed therapy. Tumor data included anatomical stage and location of the neoplasms in the pancreatic gland. Finally, administrative characteristics included variables such as zip codes of patients’ primary addresses that were used as proxies for median census income as published in previous studies and to stratify patients in groups living in rural versus urban areas. Distance to travel to tertiary medical centers were also calculated by using administrative data.
Continuous variables were expressed by median and inter-quartile range, and normality of data were checked using the Shapiro-Wilks test. Categorical variables were examined using Fisher’s exact test when appropriate or Pearson chi square test and reported as proportion or percentages. Multivariate logistic regression analysis by maximum likelihood estimation was used to test the null hypothesis where referral to medical oncology was the dependent variable and age, gender, sociodemographic characteristics, number of comorbidities, surgical resection were potential predictors. A second logistic analysis was performed to evaluate predictors of consultations by medical oncologists after patients’ referral. For logistic regression analysis, covariates were selected based on clinical relevance and from previous scientific literature and included if their p value was <0.20. If meaningful interactions between variables were identified, they were incorporated into the final models. Statistical significance of continuous and categorical variables, after checking for collinearity and adjusting for confounders and effect modifiers produced the final model.
All statistical analysis was carried out using SAS® (Version 8.2, Cary, North Carolina). Two-tailed analyses were performed unless otherwise specified and all statistical analyses were considered significant for P≤0.05.
RESULTS
Socio-demographic characteristics of the study population are summarized in Table 2. A total of 1,161 patients, with mean age of 72 years and equal distribution between males and females, satisfied the inclusion criteria. Patients living in rural areas and with low income represented 31% and 40% of the sample respectively. The head of the pancreas was the most frequent anatomical location (45%) of PC, and distant metastases were present in 50% of patients at the time of diagnosis. Surgical therapy with curative intent was performed on 136 patients (11.7%) while the rest of the cohort received best supportive therapy or palliative chemotherapy. Medical oncology referrals were requested for 39.5% of patients included in this study and consultations were documented in 33.6% of the entire cohort. When stratified by treatment modality, 60% of patients who underwent surgical resection were referred to medical oncologists in comparison to 36.2% of patients who did not undergo surgery (P<0.001) Figure 2 and medical oncology consults were completed in 46% of surgical patients vs. 31% of non-surgical patients (P<0.001). No significant changes in the frequency of medical oncology referrals or consultations were observed over the study period Figure 3. At univariate analysis, factors that were associated with a higher likelihood of patients being referred to medical oncologists were younger age, low comorbidity score, higher income quintile, living in an urban area and surgical therapy for PC Table 3. When adjusted for age, sex, comorbidity score and place of residence, the only significant factors associated with the likelihood of referral to or consultation with a medical oncologist were younger age and a low comorbidity score Tables 4, 5.
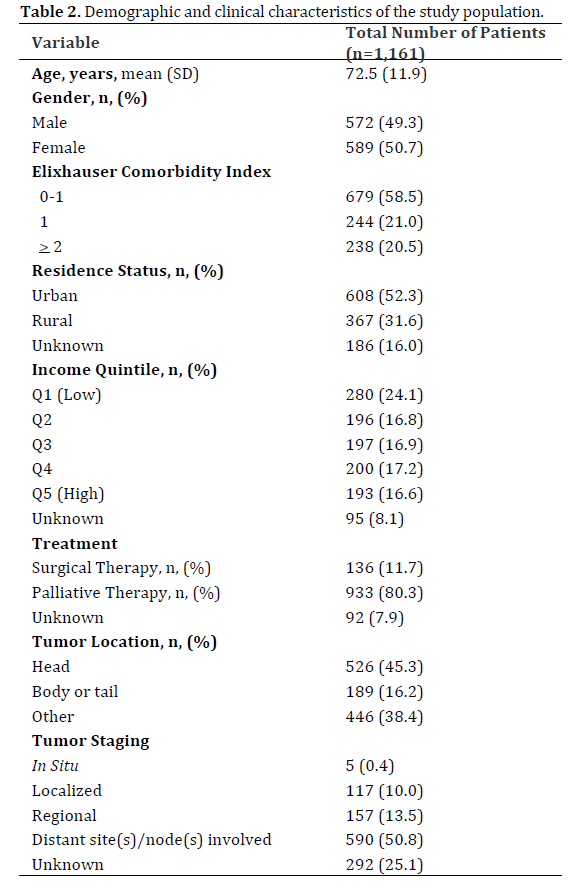
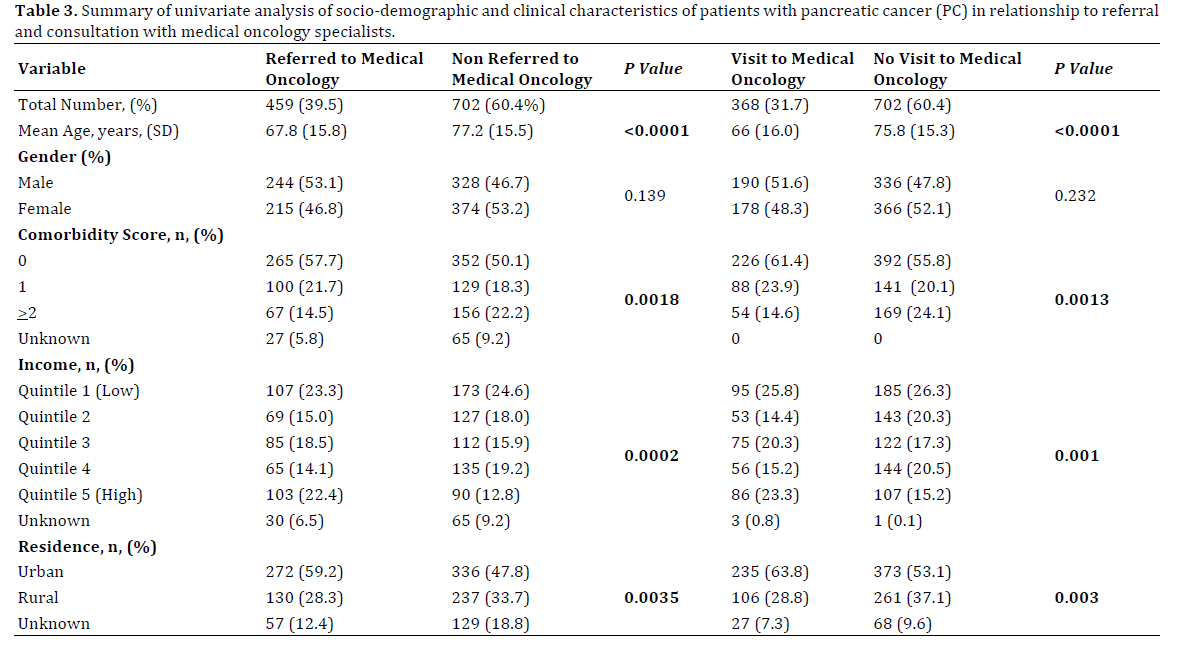
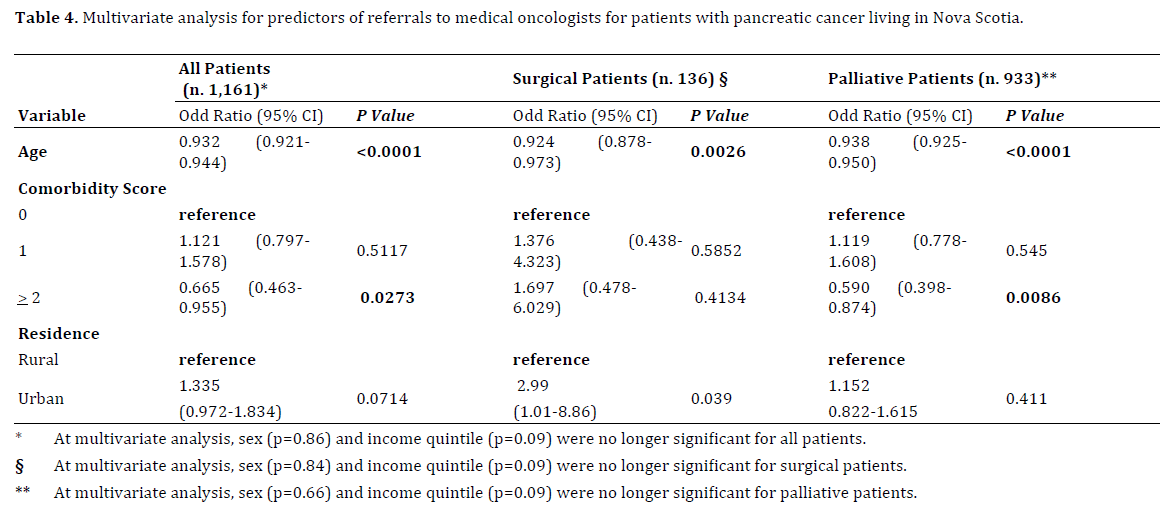
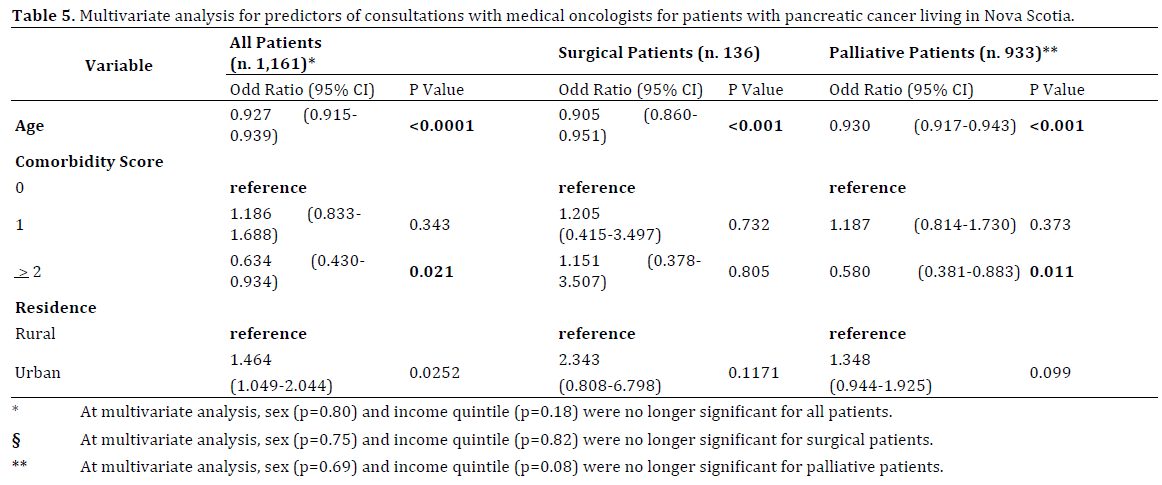
Figure 2. Histogram representing the percentage of patients who were referred to a medical oncologist and the percentage of patients who had a consultation with a medical oncology specialist. There were significant differences in the proportion of referrals and consultations between the patients who had surgical interventions and patients who were palliated. In both groups, attrition between referral and consultation was significant as 24% of patients who had surgery and who were referred for adjuvant chemotherapy did not have a medical oncology consultation. Similarly, 14% of patients who were referred for palliative chemotherapy did not have a consultation with a medical oncologist.
Figure 3. Graphical representation of the proportion of patients who were referred to a medical oncologist for consultation for adjuvant or palliative chemotherapy for pancreatic cancer in Nova Scotia during the period of nine years (2002-2010). No significant changes were identified in the trend of medical oncology referrals and consultations.
DISCUSSION
For patients with PC, the survival benefit of chemotherapy remains in the order of just a few months [2, 15]. Nevertheless, patients who receive chemotherapy enjoy better quality of life in comparison to best supportive therapy [2, 3, 4, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32]. Ideally, every patient with PC should be assessed and educated on the risks and the benefits of chemo or radiation therapies and ongoing clinical trials [33]. For most of other solid tumors, this is done in the settings of outpatient medical and radiation oncology clinics where patients can be actively engaged in important decisions regarding their treatments [34, 35, 36, 37]. However, this is not always the case and PC patients continue to have one of the lowest rates of cancer directed therapies among all patients with gastrointestinal tumors. Our study confirmed these findings as referrals to medical oncology in Nova Scotia were offered only to 39% of patients diagnosed with PC, and despite the growing evidence of the benefits provided by chemotherapy [38, 39], medical oncology referral rates did not increase over time.
For some patients, the decision not to be referred might have been due to their advanced age, comorbidities, and frailty or personal preferences. On the other hand, we cannot exclude that there might have been some inconsistencies in how physicians managed these patients as fewer patients were referred if they did not undergo surgery [7]. The low rate of referral for chemotherapy in PC is not a new finding [5]. Some of the barriers that prevent PC patients to receive cancer-directed therapy may be due to the perception that surgery or chemotherapy medications are not sufficiently effective to justify their side effects or the costs associated with their use [40]. Our data would suggest that this perception might be stronger among medical specialists than surgeons. Unfortunately we were not able to explore this further as important clinical variables such as nutritional parameters, frailty scores and patients’ preferences were not captured in administrative datasets.
There are several limitations of this study that must be acknowledged. In our opinion the most important is the retrospective design. Other shortcomings are the use of administrative databases and the fact that we enrolled only patients living in Nova Scotia where the effects of aging population, physicians shortages and reduced percapita resources dedicated to health-care might have had a considerable effect on patients’ management. Another limitation was the lack of histological confirmation of the diagnosis of PC for most of the patients who did not undergo surgery.
Our findings are comparable to several other population studies from the USA and Europe [5, 40, 41, 42, 43, 44]. On the other hand, outcomes of patients with PC in Canada are heterogeneous [45] and the results of our study might not be generalizable to other Canadian provinces. During the ten-year period analyzed, most of the patients with PC in Nova Scotia were treated with 5-Fluorouracil as Gemcitabine was only approved in the province in 2010. It is possible that the late approval of Gemcitabine might have had an effect on how medical oncologists perceived the benefits of systemic therapy and their likelihood of recommending it but we think that it was less likely to have a significant negative effect on referral rates.
This study has several strengths as it investigated a large population of PC patients in a Canadian province where, ideally, patients’ socio-economic status should not have prevented access to health care as it is equally accessible to all Canadian citizens. In addition, this is the first populationbased study on the utilization of medical oncology services for patients with PC in Nova Scotia and it is one of the few carried out in Canada.
Several conclusions could be drawn from our data. The first is that cancer directed therapy for PC continues to be offered only to a minority of patients. Therefore, more integrated multidisciplinary models of cancer care should be implemented since 5-year survival of PC patients in Nova Scotia remains one of the lowest in Canada [45].
The second is that the proportion of patients who were diagnosed with resectable disease remained below the desirable level reported in other centers where surgery is performed in up to 20-25% of patients [44]. The last point is that a significant proportion of patients were not referred to medical oncologists for chemotherapy due to their age or comorbidities. This was more common for patients living in non-urban locations, with lower socio-economic status and who did not undergo surgical therapy. Although lower rates of cancer-directed therapy in some groups of patients may reflect personal preferences or a low functional status, the extent of variations seen in this study would suggest that physicians’ attitudes may have played an important role.
Conflict of Interest
The authors declare that there is no conflict of interests regarding the publication of this paper.
References
- Society CC. Canadian Cancer Statistics. In Society CC (ed). Toronto, ON: 2011.
- Sharma C, Eltawil KM, Renfrew PD, Walsh MJ, Molinari M. Advances in diagnosis, treatment and palliation of pancreatic carcinoma: 1990-2010. World J Gastroenterol 2011; 17:867-897. [PMID:21412497]
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817-1825. [PMID:21561347]
- Krzyzanowska MK, Weeks JC, Earle CC. Treatment of locally advanced pancreatic cancer in the real world: population-based practices and effectiveness. J Clin Oncol 2003; 21:3409-3414. [PMID:12972517]
- Sharp L, Carsin AE, Cronin-Fenton DP, O'Driscoll D, Comber H. Is there under-treatment of pancreatic cancer? Evidence from a population-based study in Ireland. Eur J Cancer 2009; 45:1450-1459. [PMID: 19268569]
- Takhar AS, Palaniappan P, Dhingsa R, Lobo DN. Recent developments in diagnosis of pancreatic cancer. BMJ 2004; 329:668-673. [PMID: 15374918]
- Visser BC, Ma Y, Zak Y, Poultsides GA, Norton JA, Rhoads KF. Failure to comply with NCCN guidelines for the management of pancreatic cancer compromises outcomes. HPB (Oxford) 2012; 14:539-547. [PMID: 22762402]
- O'Connell JB, Maggard MA, Ko CY. Cancer-directed surgery for localized disease: decreased use in the elderly. Ann Surg Oncol 2004; 11:962-969. [PMID: 15525824]
- Nordby T, Ikdahl T, Lothe IM,Ånonsen K, Hauge T, Edwin B, Line PD, et al. Opportunities of improvement in the management of pancreatic and periampullarytumors. Scand J Gastroenterol 2013; 48:617-625. [PMID: 23597153]
- Kim C, Owen D, Gill S. Real-world impact of availability of adjuvant therapy on outcomes in patients with resected pancreatic adenocarcinoma: a Canadian Cancer Agency experience. Am J Clin Oncol 2012; 35:212-215. [PMID: 21358297]
- Akahori T, Sho M, Tanaka T, Kinoshita S, Nagai M, Nishiwada S, Nishiofuku H, et al. Factors associated with failure to complete adjuvant chemotherapy in pancreatic cancer. Am J Surg 2016; 211:787-792. [PMID: 26846177]
- Canadian Institute for Health Information, Discharge Abstract Database (DAD). In. 2015; Originally developed in 1963, the Discharge Abstract Database (DAD) captures administrative, clinical and demographic information on hospital discharges (including deaths, sign-outs and transfers). Some provinces and territories also use the DAD to capture day surgery.
- Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care 1998; 36:8-27. [PMID: 9431328]
- Canada S. Canada, Statistics. In. Ottawa: Canadian Statistics 2006.
- Fung MC IH, Takayama S, Morizane T, Adachi S, Sakata T. Survival benefit of chemotherapy treatment in advanced pancreatic cancer: a meta-analysis [abstract]. Proc Ann Meet Am Soc Clin Oncol 2003; 22:1155.
- Bilimoria KY, Bentrem DJ, Lillemoe KD, Talamonti MS, Ko CY; Pancreatic Cancer Quality Indicator Development Expert Panel, American College of Surgeons. Assessment of pancreatic cancer care in the United States based on formally developed quality indicators. J Natl Cancer Inst 2009; 101:848-859. [PMID: 19509366]
- Gooden HM, White KJ. Pancreatic cancer and supportive care--pancreatic exocrine insufficiency negatively impacts on quality of life. Support Care Cancer 2013; 21:1835-1841. [PMID: 23397095]
- Raval MV, Bilimoria KY, Talamonti MS. Quality improvement for pancreatic cancer care: is regionalization a feasible and effective mechanism? Surg Oncol Clin N Am 2010; 19:371-390.
- Bilimoria KY, Bentrem DJ, Tomlinson JS. Quality of pancreatic cancer care at Veterans Administration compared with non-Veterans Administration hospitals. Am J Surg 2007; 194:588-593. [PMID: 20159520]
- Brennan MF. Quality pancreatic cancer care: it's still mostly about volume. J Natl Cancer Inst 2009; 101:837-838. [PMID: 19509363]
- Gangl O, Froschl U, Fugger R. Surgical quality data and survival after pancreatic cancer resections: a comparison of results for octogenarians and younger patients. Wien Klin Wochenschr 2014; 126:757-761. [PMID: 25249303]
- Chakraborty S, Singh S. Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study. Ann Gastroenterol 2013; 26:346-352. [PMID: 24714323]
- Yuan C, Rubinson DA, Qian ZR, Wu C, Kraft P, Bao Y, Ogino S, et al. Survival among patients with pancreatic cancer and long-standing or recent-onset diabetes mellitus. J Clin Oncol 2015; 33:29-35. [PMID: 25403204]
- Kim DD, Zhu H, Nassri AB, Mokdad A, Kukreja S, Polanco P, Huerta S, et al. Survival analysis of veteran patients with pancreatic cancer. J Dig Dis 2016; 17:399-407.
- Christians KK, Heimler JW, George B, Ritch PS, Erickson BA, Johnston F, Tolat PP, et al. Survival of patients with resectable pancreatic cancer who received neoadjuvant therapy. Surgery 2016; 159:893-900. [PMID: 26602840]
- Kizilbash SH, Ward KC, Liang JJ, Jaiyesimi I, Lipscomb J. Survival outcomes in patients with early stage, resected pancreatic cancer - a comparison of gemcitabine- and 5-fluorouracil-based chemotherapy and chemoradiation regimens. Int J Clin Pract 2014; 68:578-589. [PMID: 24472057]
- Bernards N, Haj Mohammad N, Creemers GJ, de Hingh IH, van Laarhoven HW, Lemmens VE. Ten weeks to live: a population-based study on treatment and survival of patients with metastatic pancreatic cancer in the south of the Netherlands. Acta Oncol 2015; 54:403-410. [PMID: 25263080]
- Baxter NN, Whitson BA, Tuttle TM. Trends in the treatment and outcome of pancreatic cancer in the United States. Ann Surg Oncol 2007; 14:1320-1326. [PMID: 17225980]
- Sun H, Ma H, Hong G, Sun H, Wang J. Survival improvement in patients with pancreatic cancer by decade: a period analysis of the SEER database, 1981-2010. Sci Rep 2014; 4:6747. [PMID: 25339498]
- Opfermann KJ, Wahlquist AE, Garrett-Mayer E, Shridhar R, Cannick L, Marshall DT. Adjuvant radiotherapy and lymph node status for pancreatic cancer: results of a study from the Surveillance, Epidemiology, and End Results (SEER) Registry Data. Am J Clin Oncol 2014; 37:112-116. [PMID: 23211221]
- Gooiker GA, van der Geest LG, Wouters MW, Vonk M, Karsten TM, Tollenaar RA, Bonsing BA. Quality improvement of pancreatic surgery by centralization in the western part of the Netherlands. Ann Surg Oncol 2011; 18:1821-1829. [PMID: 21544657]
- Desai NV, Sliesoraitis S, Hughes SJ, Trevino JG, Zlotecki RA, Ivey AM, George TJ Jr. Multidisciplinary neoadjuvant management for potentially curable pancreatic cancer. Cancer Med 2015; 4:1224-1239. [PMID: 25766842]
- (R)) NCPGiONG. Pancreatic Adenocarcinoma. In National Comprehensive Cancer Network. Practice Guidelines for Pancreatic Cancer. Accessed on August 8 (ed) I.2016 Edition. National Comprehensive Cancer Network 2016.
- Back A. Patient-physician communication in oncology: what does the evidence show? Oncology (Williston Park) 2006; 20:67-74; discussion 77-68, 83. [PMID: 16572594]
- Blanchard CG, Labrecque MS, Ruckdeschel JC, Blanchard EB. Information and decision-making preferences of hospitalized adult cancer patients. Soc Sci Med 1988; 27:1139-1145. [PMID: 3206248]
- Boivin A, Green J, van der Meulen J, Légaré F, Nolte E. Why consider patients' preferences? A discourse analysis of clinical practice guideline developers. Med Care 2009; 47:908-915. [PMID: 19543120]
- Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med 1997; 44:681-692. [PMID: 9032835]
- Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K, Niedergethmann M, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA 2013; 310:1473-1481. [PMID: 24104372]
- Liao WC, Chien KL, Lin YL, Wu MS, Lin JT, Wang HP, Tu YK. Adjuvant treatments for resected pancreatic adenocarcinoma: a systematic review and network meta-analysis. Lancet Oncol 2013; 14:1095-1103. [PMID: 24035532]
- Enewold L, Harlan LC, Tucker T, McKenzie S. Pancreatic cancer in the USA: persistence of undertreatment and poor outcome. J Gastrointest Cancer 2015; 46:9-20. [PMID: 25403828]
- Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP, Talamonti MS. National failure to operate on early stage pancreatic cancer. Ann Surg 2007; 246:173-180. [PMID: 17667493]
- Bilimoria KY, Bentrem DJ, Ko CY, Tomlinson JS, Stewart AK, Winchester DP, Talamonti MS. Multimodality therapy for pancreatic cancer in the U.S. : utilization, outcomes, and the effect of hospital volume. Cancer 2007; 110:1227-1234. [PMID: 17654662]
- Parmar AD, Vargas GM, Tamirisa NP, Sheffield KM, Riall TS. Trajectory of care and use of multimodality therapy in older patients with pancreatic adenocarcinoma. Surgery 2014; 156:280-289. [PMID: 24851723]
- Eloubeidi MA, Desmond RA, Wilcox CM, Wilson RJ, Manchikalapati P, Fouad MM, Eltoum I. Prognostic factors for survival in pancreatic cancer: a population-based study. Am J Surg 2006; 192:322-329. [PMID: 16920426]
- Hurton S, MacDonald F, Porter G, Walsh M, Molinari M. The current state of pancreatic cancer in Canada: incidence, mortality, and surgical therapy. Pancreas 2014; 43:879-885. [PMID: 24763076]




