Keywords
complications; Early Diagnosis; Pancreatitis; Acute
Necrotizing; presepsin protein; human
Abbreviations
ANP acute necrotizing pancreatitis; ROC receiveroperating
characteristic
INTRODUCTION
Acute necrotizing pancreatitis (ANP) is a surgical
disease caused by primary aseptic necrosis of the
pancreatic tissues, accompanied by the development of
SIRS in both aseptic and infected necrosis. In recent years
there has been a significant increase in the number of
patients with infected forms of ANP and the development
of septic complications, whose mortality reaches 5.5-
35.2% [1, 2, 3]. Early diagnosis of infection occurrence
is crucial for choosing the optimal treatment strategy
[4, 5]. At the same time, infectious complications at ANP
do not have specific symptoms and clinical features that
distinguish sterile from infected pancreatic necrosis.
Computed tomography (CT) which is currently the
imaging study of choice for diagnosis of acute pancreatic
and peri-pancreatic necrotic collections can only suggests
the presence of infection. The appearance of air bubbles within the necrotic pancreatic parenchyma on CT scans is
considered as an almost pathognomonic finding indicating
the presence of infected pancreatic necrosis, but in some
cases the presence of gas indicates a connection with the
gastrointestinal tract. Besides, this finding is observed in
only one third of patients with infected pancreatic necrosis,
and therefore its absence cannot exclude the diagnosis
of infected pancreatic necrosis [6, 7]. Bacteriological
examination by means of fine needle aspiration of the
necrotic collection, which is considered to be the diagnostic
"gold standard", needs a lot of time and costs while nearly
a third of the patients will receive the negative results [8].
For differential diagnosis of SIRS and abdominal sepsis
currently determination of the level of several serological
markers of inflammation were applied and presepsin was
recognized as most promised [9, 10]. So aim of our research
was to study the diagnostic utility of the presepsin for early
diagnosis of infectious complications of ANP.
MATERIAL AND METHODS
This study was performed at Regional Emergency
Hospital, Chernivtsi, Ukraine, between February 2014 and
December 2017. During this period 408 patients with acute
pancreatitis were admitted to clinic. Acute pancreatitis
was defined according to the 2012 revision of the
Atlanta classification as an association of two of the three
following features: typical abdominal pain (acute onset of a persistent, severe, epigastric pain often radiating to the
back), serum lipase or amylase activity at least three times
greater than the upper limit of normal, and characteristic
findings of acute pancreatitis on abdominal cross-sectional
imaging studies [11]. Necrotizing pancreatitis was
characterized by inflammation and associated pancreatic
parenchymal necrosis and/or peripancreatic necrosis, as
shown by a lack of pancreatic parenchymal enhancement
and/or the presence of findings of acute necrotic collection
and walled-off necrosis on contrast-enhanced computed
tomography (CT). The CT-protocol for pancreatic
evaluation consisted in a retarded venous phase after
35 s of venous contrast administration. A CT scans were
performed in all patients for establishing diagnosis of ANP
between 72-96 h after the onset of abdominal pain and
were repeated if indications for intervention appeared.
Only patients to whom interventional treatment was
applied were included to current study. Besides, persons
were excluded if any of the following criteria were present:
a) age < 18 and > 80 years; b) recent surgical interventions;
c) psychoses; d) pregnancy; e) previously history of chronic
pancreatitis. After exclusion of abovementioned cases we
enrolled to current study 70 patients with ANP.
In line with international guidelines, intervention was
generally only performed in case of suspected or confirmed
infection of pancreatic necrosis or peri-pancreatic necrosis
alone accompanying an aggravated general condition
[12, 13]. The decision to intervene was based on clinical
grounds (presence of SIRS and ongoing organ failure)
and results of CT scans. Whenever possible, intervention
was postponed until approximately four weeks after the
onset of disease. Microbiological investigation of biological
material from necrotic collections was performed at
time of intervention and every 3rd day in case draining
was applied until removing of drains. Blood culture was
performed in all persons at time of intervention and
repeated in case deterioration of patient’s condition.
Before interventional treatment EDTA plasma samples
were collected for presepsin determination. The plasma
samples were categorized into 4 groups according to
results of microbiological assay at time of intervention and
clinical conditions of patients: SIRS without infection, local
infection, sepsis and septic shock. Besides, plasma samples
were collected from 10 healthy persons as control values
for presepsin.
Severity of ANP was determined in line with the
recently revised Atlanta Classification [11, 12, 13] by
presence and duration of organ failure as well as by
APACHE II score. Organ failure was defined by modified
Marshall scoring system. The diagnoses of SIRS, sepsis
and septic shock were made according to the criteria
described by the American College of Chest Physicians/
Society of Critical Care Medicine (ACCP/ SCCM) [14]. All
patients received fluid resuscitation, and full laboratory
investigations were performed on the first 3 days and in
the 24 hours before any intervention. Nasojejunal enteral
feeding was initiated if an oral diet was not tolerated
after 48-72 hours after admission. If there were problems with nasojejunal intubation nasogastric tube feeding was
started. Parenteral nutrition was only initiated when oral
route was not tolerated or sufficient, but at least small
amount of enteral feeding was present in all patients.
The plasma samples were stored at −70°C until
measurement. Presepsin was determined using (Mitsubishi
Chemical Medience Co., Tokyo, Japan), a chemiluminescent
enzyme immunoassay for the quantitative measurement
of presepsin concentration in whole blood or plasma.
The test principle is based on the non-competitive
chemiluminescence enzyme immunoassay [10]. During
incubation of the sample with alkaline phosphatase-labeled
anti-presepsin polyclonal antibody and anti- presepsin
monoclonal antibody-coated magnetic particles, presepsin
of the sample binds to the anti-presepsin antibodies,
forming an immune complex with enzyme-labeled
antibody and antibody-coated magnetic particles. After
removal of the unbound substances a chemiluminescent
substrate is added. After a short incubation period, the
luminescence intensity generated by the enzyme reaction
is measured. The luminescence intensity is related to the
presepsin concentration of the sample, which is calculated
by means of a standard curve (measurement range: 20
–20,000 ng/l, functional sensitivity: 57.1 ng/l, reference
interval: 60 –365 ng/l).
Ethics
The study was conducted in accordance with the
principles of the Declaration of Helsinki. The ethics
review board of each participating hospital approved the
study. Patients or their legal representatives gave written
informed consent.
Statistical Analysis
Results of presepsin determination were presented
as median [inter-quartile range (IQR)]. Two-group
comparisons were performed using the Mann–Whitney
U-test with the Bonferroni correction, and multiple
comparisons were performed using the Kruskal–Wallis H
test or one-way repeated-measures analysis of variance
(ANOVA) with Dunnett’s multiple comparison tests. We
used the cut-off value obtained by a receiver-operating
characteristic (ROC) analysis. Values of P less than 0.05
were considered to indicate statistical significance.
Group comparisons and ROC analyses were performed
using JMP software (SAS Institute, Cary, North Carolina,
USA). Analyses of Spearman correlation coefficients and
interactions were performed using SPSS 18 software
(SPSS, Chicago, Illinois, USA).
RESULTS
Although suspension of infected ANP with typical
clinical presentation (SIRS, ongoing organ failure,
leukocytosis, etc.) was the only indication for interventional
treatment in current study bacteriological investigation of
necrotic collections confirmed infection presence in 49
(70.0%) patients. There were no septicemia and organ
dysfunction at time of invasive procedure in 15 of them (Table 1). Positive blood cultures and/or SOFA score
over 2 were estimated in 37 patients with infected ANP
and 12 cases among them were presented with septic
shock.
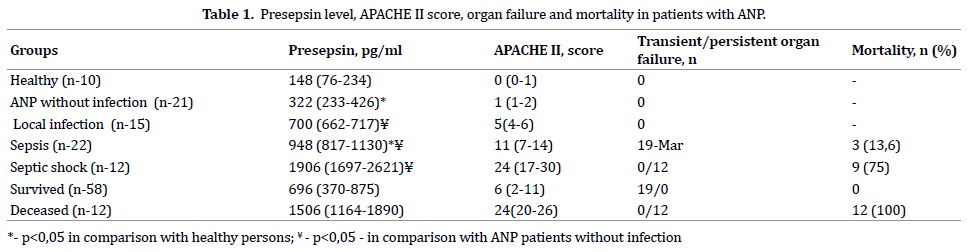
Examination of healthy individuals (control group)
determined presepsin concentration in the blood plasma
on an average level of 148 (76-234) pg/ml. The signs of
SIRS were presented in all patients without infection of
necrotic collection and their presepsin concentration
blood increased on an average to 322 (233-426) pg/ml,
p=0.02. Infection occurrence in patients with ANP was
associated with reliable increase of presepsin level an
average to 880 (714-1247) pg/ml (p=0,001), which is
2.7 times as high as in patients without infection. At early
stages of infected complications when they were local
(without signs of generalization) presepsin level increased
to 700 (662-717) pg/ml, p=0.001. Presepsin concentration
increases progressively with sepsis to 948 (817-1130)
pg/ml and in case of septic shock – to 1906 (1697-2621)
pg/lm, p=0,001. ROC-analysis found a high dependence
of presepsin level on infectious complications available
with acute necrotic pancreatitis (AUC ROC 0.956, СІ 0.883-
0.972, p=0.001, Figure 1). According to the data of the
study critical presepsin concentration which is indicative
of occurrence of infected ANP was 632 pg/ml (sensitivity –
90. 11%, specificity – 92.86%).
Figure 1: AUC Roc for infected acute necrotizing pancreatitis diagnosis by presepsin level in blood.
Generalization of infected complications was followed
by worsening of patients’ condition: the majority of
persons with sepsis developed transient organ failure, in
3 patients occurred persistent organ failure (in all cases
- renal). All the 12 patients with septic shock had got
multiple organ failure producing unfavorable effect on
the results of treatment. Besides vascular, there were 7
cases of pulmonary, 4 – renal, 3 – neurological, 2 – hepatic
failures. In patients with renal failure concentration of
presepsin increased not significantly: 1084 (1061-1164)
pg/ml, p=0.254 - in case of sepsis and 2033 (1851-2398),
p=0.722 – in persons with septic shock, respectively.
Direct correlation between presepsin level and the score
evidencing severity of patients’ condition by APACHE
II scale was found (Figure 2), correlation coefficient
between presepsin concentration and the score according
to APACHE II scale was 0,798 (p=0.001).
Figure 2: between presepsin level in blood and APACHE II score.
12 patients out of 70 being examined died (17.1%):
3 patients out of 22 with sepsis, and 9 out of 12 – with
septic shock. Presepsin level and the APACHE II score in
those who died at time of intervention were significantly
higher than in those patients who survived (Table 1).
High presepsin level and the APACHE II score were equally
indicative of the lethal outcome development: AUC ROC
for presepsin was 0.896 ± 0.37 and 0.962 ± 0.28 – for
APACHE ІІ scale, p=0.01. Presepsin level higher than 1032 pg/ml was considered to have unfavourable prognosis for
patients to survive, and it corresponded to 16 points by
APACHE II scale (sensitivity 82.24 %, specificity 88.12 %).
DISCUSSION
Infection of pancreatic necrosis is a common occurrence
with overall rates of infection ranging from 30% to 70%.
Early diagnosis and early treatment are essential to
improving the results of treatment of infected ANP [4, 5].
Compared with patients with sterile pancreatic necrosis,
those with infected necrosis had significantly higher
morbidity and mortality [1, 2, 3]. At the same time,
infectious complications at ANP do not have specific
symptoms and clinical features that distinguish sterile
from infected pancreatic necrosis whereas modern
imaging methods can only suggest the presence of
infection [6, 7].
Taking in account insufficient specificity of imaging
methods for early diagnosis of infected ANP some
laboratorial markers were evaluated. C-reactive protein
was one of the first studied biomarker but its elevation
was related mostly to grade of SIRS than infection alone
[15]. Same problem were found with other promising
markers – interleukin-6 and procalcitonin. Both of them
showed good specificity for sepsis diagnosis, especially
procalcitonin, but their cut-off levels were too high for
discrimination infected necrosis cases from ANP patients
presented by SIRS without infection thus lowering their
accuracy [16, 17, 18].
In our research we evaluated efficacy of new sepsis
biomarker presepsin for early diagnosis of infected ANP.
Presepsin was identified as a protein whose levels are
elevated specifically in the blood of patients with sepsis.
One of the production mechanisms of presepsin is related
to bacterial phagocytosis, and the cleavage of membrane
CD14 by lysosomal enzymes of granulocytes are involved
in its secretion. The measurement of presepsin levels is
useful for the diagnosis of sepsis, evaluating the severity
of sepsis, and monitoring clinical responses to therapeutic
interventions.
In our study presepsin level was considerably higher
both in patients with infected ANP comparing those
having SIRS without infection. A clear dependence of
presepsin concentration on the activity and severity of
infectious process was found. At the same time, in addition
to increased presepsin level only 11 out of 15 patients
with local infection developed the signs of infection
such as leukocytosis (>12000) and immature forms of
granulocytes >10%. Although, further bacteriological
examination found pathological microorganisms in all
the cases. It is explained by the fact that the mechanism
of presepsin increase differs radically from other proinflammatory
markers. Presepsin is formed by means of
enzymatic splitting of the circulating soluble receptor СD-
14 by proteases with bacterial phagocytosis at the earliest
stage of inflammation before the increase of interleukin-6
level and laboratory signs of systemic inflammatory response syndrome. Contrary to other markers of sepsis
the time of presepsin half-life in the blood plasma is very
short – from 30 minutes to 4 hours, and for procalcitonin
– 25-30 hours. Presepsin concentration increased
progressively with sepsis to 948 (817-1130) pg/ml and in
case of septic shock – to 1906 (1697-2621) pg/ml, which
is almost three and six times as much respectively from
the parameters of patients with SIRS without infection.
Elevation of presepsin concentration in patients with renal
failure was not significant in comparison with appropriate
group, but amount of persons with it was nonsufficient in
our study to make any conclusion.
Severity of condition of the examined patients
with sepsis and severe sepsis was determined by the
development of organ failure. An expected relation was
found between presepsin level and the score evidencing
severity of patients’ condition by APACHE II scale (Figure
2). Presepsin level and the score according to APACHE II
scale in those who died were twice and 1, 8 times as much
as respectively than in those patients who survived. High
presepsin level and the score according to APACHE II scale
reliably (p<0.01) were equally indicative of the lethal
outcome development when patients with acute necrotic
pancreatitis were admitted.
CONCLUSIONS
Determination of presepsin in the blood allows
confirming with high sensitivity and clinical specificity
both local and systemic infected complications during
acute necrotizing pancreatitis. High levels of presepsin
(over 1032 pg/ml) have negative prognostic utility for
patients surviving.
Acknowledgments
The authors are grateful to all contributors to this
research especially the director of the private unitary
enterprise “ARGOMEDA”, Minsk, Belarus, Dr. Yaraslau
Latushka and staff of surgical and intensive care
departments of Chernivtsi Emergency Regional Hospital,
Ukraine, for helping of performing research.
Competing and conflicting Interests
There are no competing and conflicting interests.
References
- Werge M, Novovic S, Schmidt PN, Gluud LL. Infection increases mortality in necrotizing pancreatitis: A systematic review and metaanalysis. Pancreatology 2016; 16:698-707. [PMID: 27449605]
- Ji L, Lv JC, Song ZF, Jiang MT, Li L, Sun B. Risk factors of infected pancreatic necrosis secondary to severe acute pancreatitis. Hepatobiliary Pancreat Dis Int 2016; 15:428-33. [PMID: 27498584]
- Jain S, Mahapatra SJ, Gupta S, Shalimar, Garg PK. Infected Pancreatic Necrosis due to Multidrug-Resistant Organisms and Persistent Organ failure Predict Mortality in Acute Pancreatitis. Clin Transl Gastroenterol 2018; 9:190-5. [PMID: 30287818]
- Zerem E. Treatment of severe acute pancreatitis and its complications. World J Gastroenterol 2014; 20:13879–92. [PMID: 25320523]
- Aparna D, Kumar S, Kamalkumar S. Mortality and morbidity in necrotizing pancreatitis managed on principles of step-up approach: 7 years’ experience from a single surgical unit. World J Gastrointest Surg 2017; 9:200-8. [PMID: 29109852]
- Triantopoulou C, Delis S, Dervenis C. Imaging evaluation of postpancreatitis infection. Infect Disord Drug Targets 2010; 10:15-20. [PMID: 20180754]
- Heiss P, Bruennler T, Salzberger B, Lang S, Langgartner J, Feuerbach S, et al. Severe acute pancreatitis requiring drainage therapy: findings on computed tomography as predictor of patient outcome. Pancreatology 2010; 10:726-33. [PMID: 21242714]
- van Baal MC, Bollen TL, Bakker OJ, van Goor H, Boermeester MA, Dejong CH, et al. Dutch Pancreatitis Study Group. The role of routine fineneedle aspiration in the diagnosis of infected necrotizing pancreatitis. Surgery 2014; 155:442-8. [PMID: 24287142]
- Perner A, Gordon AC, De Backer D, Dimopoulos G, Russell JA, Lipman J, et al. Sepsis: frontiers in diagnosis,resuscitation and antibiotic therapy. Intensive Care Med 2016; 42:1958-69. [PMID: 27695884]
- Liu Y, Hou JH, Li Q, Chen KJ, Wang SN, Wang JM. Biomarkers for diagnosis of sepsis in patients with systemic inflammatory response syndrome: a systematic review and meta-analysis. Springerplus 2016; 5:2091. [PMID: 28028489]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62:102-11. [PMID: 23100216]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/ APA evidence-based guidelines for the management of acute pancreatitis. Pancreatology 2013; 13:e1–15. [PMID: 24054878]
- Yokoe M, Takada T, Mayumi T, Yoshida M, Isaji S, Wada K, et al. Japanese guidelines for the management of acute pancreatitis: Japanese Guidelines 2015. J Hepatobiliary Pancreat Sci 2015; 22:405-32. [PMID: 25973947]
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016; 315:801-10. [PMID: 26903338]
- Yang CJ, Chen J, Phillips AR, Windsor JA, Petrov MS. Predictors of severe and critical acute pancreatitis: a systematic review. Dig Liver Dis 2014; 46:446-51. [PMID: 24646880]
- Chen HZ, Ji L, Li L, Wang G, Bai XW, Cheng CD, Sun B. Early prediction of infected pancreatic necrosis secondary to necrotizing pancreatitis. Medicine (Baltimore) 2017; 96:e7487. [PMID: 28746189]
- Dias BH, Rozario AP, Olakkengil SA, Anirudh V. Procalcitonin Strip Test as an Independent Predictor in Acute Pancreatitis. Indian J Surg 2015; 77(Suppl3):1012-7. [PMID: 27011501]
- Adachi T, Kishihara Y, Okano H, Honzawa H, Hirayama M, Higashi H, et al. The utility of procalcitonin for the patients with infected pancreatic necrotic and pancreatic abscess. Intensive Care Med Exp 2015; 3:2197- 425. [PMCID: PMC4796962]



