Keywords
Endoscopic Ultrasound-Guided Fine Needle Aspiration; Endosonography; Pancreas; Pancreatic Cyst; Pancreatic Neoplasms
Abbreviations
AUC: area under the receiver operator characteristic curves; IAP: International Association of Pancreatology; MCN: mucinous cystic neoplasm
INTRODUCTION
With increased use and improvements in radiologic imaging, pancreatic cystic lesions have been identified with ever increasing frequency. Pancreatic cystic lesions have been identified in up to 20% of MRI studies [1, 2]. These lesions raise concern because of their potential for prevalent or incident malignancy. The most common pancreatic cysts are broadly classified into mucinous cystic lesions including mucinous cystic neoplasm (MCN) and intraductal papillary mucinous neoplasm (IPMN) versus nonmucinous lesions such as serous cystadenomas. Mucinous cysts are premalignant while nonmucinous cystic lesions have low or no malignant potential.
Traditional methods used to classify pancreatic cysts include cross-sectional imaging, EUS, measurement of cyst fluid tumor marker CEA, and cytology [3, 4]. Despite advances in imaging, refinement of clinical criteria, and the proven safety of EUS-FNA [5], detection of malignancy in asymptomatic pancreatic cystic lesions remains a challenge [6, 7, 8, 9, 10, 11]. DNA analysis has been advanced as an additional tool that may improve the accuracy of identifying malignancy [12, 13]. In the prospective, multicenter PANDA study, the presence of a high amplitude k-ras mutation followed by loss of heterozygosity in pancreatic cyst fluid was highly specific (96%) though insensitive (37%) for detection of malignancy [12].
The aims of this study were to assess the accuracy of commercial DNA analysis for detecting malignancy at the time of EUS in pancreatic cysts presenting for EUS-FNA, and to determine whether DNA analysis offers additional predictive power compared to the widely applied International Association of Pancreatology (IAP) guidelines for resection of pancreatic cysts concerning for malignancy [14, 15].
METHODS
Study Design
This is a retrospective cohort study conducted at a tertiary care academic medical center for pancreatic disorders.
Participants
Patients undergoing EUS-FNA of a pancreatic cystic lesion with DNA analysis sent at the time of EUS from June 2006 to January 2012 were eligible for study inclusion. Further inclusion criteria consisted of availability of either pathology from surgical resection or at least one year of clinical follow-up from the time of initial EUS. Duration of follow-up was measured as the time from initial EUS-FNA to the most recent imaging study (CT, MRI, and/or EUS). Patients were excluded from the study if they only had a solid mass based on radiographic imaging or a history of acute pancreatitis within the previous six months.
Endoscopic Technique
EUS was performed using a curvilinear echoendoscope (Olympus GF-UCT140P-OL5; Olympus America Inc., Center Valley, PA, USA), and a 19-, 22-, or 25-gauge adjustable needle (Echotip Ultra 19 and 25 gauge, Cook, Winston-Salem, NC, USA; EZ Shot, Olympus, Center Valley, PA, USA) was used for FNA. Cyst fluid studies including cytology and DNA analysis were performed. It was standard practice at our institution during the time period of this study to send cyst fluid routinely for DNA analysis in addition to the other standard testing. If the cyst fluid and tissue were completely used for other testing, cytology was not obtained. Antibiotic prophylaxis was administered at the discretion of each endosonographer.
Commercial DNA Analysis
Details of the technique of commercial DNA analysis (RedPath Integrated Pathology, Inc., Pittsburgh, PA, USA): are previously described [12]. In brief, the cyst fluid (10-200 μL) underwent measurement of 1) DNA quantity (optical density; NanoDrop, Thermo Fisher Scientific, Waltham, MA, USA), 2) DNA quality (extent of degradation by quantitative PCR), 3) k-ras point mutation (first coding exon) (dideoxy sequencing), 4) allelic imbalance or loss of heterozygosity for a panel of 16 markers (GeneScan fragment length analysis; Applied Biosystems, Foster City, CA, USA) and 5) degree of clonal expansion of DNA alterations when present (ratio of peak heights).
Primary Outcome
Cysts with histologic or cytologic evidence of malignancy were defined as malignant in accordance with World Health Organization guidelines [16]. In surgical pathology specimens, invasive adenocarcinomas, including those arising in association with an IPMN or MCN, and high grade dysplasia were considered malignant. Malignant cytology was defined as positive for adenocarcinoma. All other cysts were defined as nonmalignant. In addition, cysts that were unchanged after at least 1-year follow-up were considered nonmalignant. All available glass slides from surgical pathology specimens were re-reviewed by a gastrointestinal pathologist blinded to the original diagnosis.
ETHICS
The protocol was approved by the Institutional Review Board of Brigham and Women’s Hospital, Boston, MA, USA. The study protocol conforms to the ethical guidelines of the “World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008. Data were collected retrospectively and patient informed consent was waived by the Institutional Review Board.
STATISTICS
Test Performance
Test characteristics including sensitivity, specificity, PPV, and NPV for the diagnosis of malignancy were calculated for the following: suspicious or malignant cytology, the 2006 and 2012 IAP guidelines, high amplitude k-ras mutation, high amplitude loss of heterozygosity, and combined high amplitude k-ras mutation with loss of heterozygosity.
Diagnostic Value of DNA Analysis
To quantify the added diagnostic value of DNA analysis beyond that from traditional clinical, imaging, and pathologic data, we constructed 4 models for the detection of malignancy. Each of the variables in the 2006 and 2012 IAP models were considered high-risk features. The first model, based on the 2006 IAP guideline, included symptoms, cyst size on EUS imaging (dichotomous, ≥3 cm), nodularity, and main duct dilatation (dichotomous, main pancreatic duct size ≥10 mm) [14]. The second model was based on the 2012 IAP guideline where surgical resection is recommended in the presence of one of the following: obstructive jaundice with cyst present in head of pancreas, solid component, main pancreatic duct size ≥1 cm, nodularity, thick wall, intraductal mucin, and/or suspicious or malignant cytology [15]. The third DNA analysis model included high amplitude k-ras mutation, loss of heterozygosity, and high DNA quantity. The final model combined DNA analysis with the 2012 IAP guideline. Diagnostic utility was determined by comparing the area under the receiver operator characteristic curves (AUC) of the two IAP models, DNA analysis model, and the combined DNA/2012 IAP model.
Descriptive Statistics
Medians, interquartile ranges (IQR), as well as absolute and relative frequencies, were reported. The 95% confidence intervals (95% CI) of the relative frequencies were also computed.
Tests
Fisher exact, the linear-by-linear chi-squared and the Mann-Whitney tests were used for comparison of dichotomous, ordinal discrete and scale data, respectively. The method described by DeLong et al. was used for comparison of AUC among the 4 models [17].
Package
Statistical programming was performed in SAS version 9.2 (Cary, NC, USA).
Significance
All reported P values are two-sided with alpha value of 0.05 used as threshold for significance.
RESULTS
Study Population
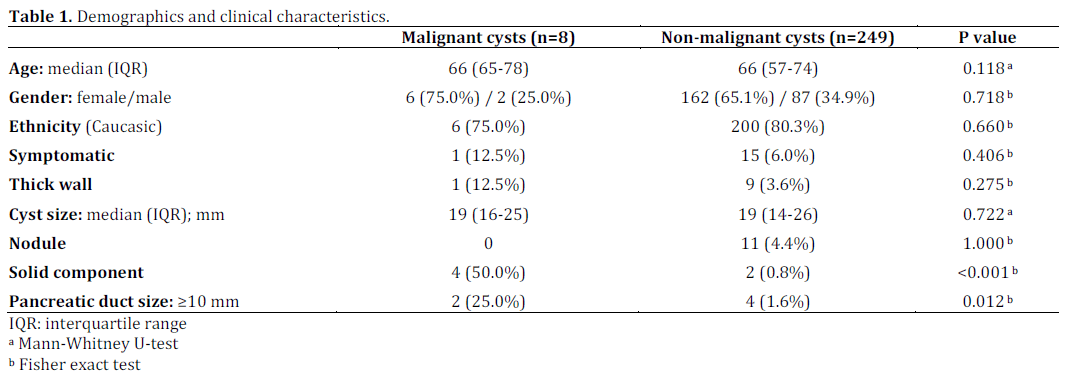
During the study period, 284 patients underwent EUS-FNA with DNA analysis sent for a pancreatic cyst at our institution. Twenty-seven of these cases were excluded due to lack of histology, inadequate DNA sample, or insufficient follow-up. The final study cohort consisted of 257 cases. Baseline demographic, clinical and imaging characteristics of the study population are presented in Table 1. Median age at the time of evaluation was 66 years (IQR: 57-74 years) and 168 patients (65.4%) were women. The majority of cysts (n=241, 93.8%) were detected incidentally. Median duration of follow-up was 19 months (IQR: 12-33 months).
Outcomes
During the study period, 33 (12.8%) patients underwent surgical resection with histologic diagnoses including IPMN with invasive adenocarcinoma (n=4), IPMN with high grade dysplasia (n=1), IPMN with low or intermediate grade dysplasia (n=15), MCN with low grade dysplasia (n=1), serous cystadenoma (n=2), pseudocyst (n=3), lymphoepithelial cyst (n=1), chronic pancreatitis (n=4), autoimmune pancreatitis (n=1), and neuroendocrine tumor (n=1). At least one high-risk feature was present in 17 patients who underwent resection. Overall, 8 cases (3.1%) met criteria for a malignant lesion (5 from surgical pathology and 3 from cytology). Diagnoses included 7 IPMN with invasive adenocarcinoma and 1 IPMN with high grade dysplasia. No additional patients developed a malignant cyst during the study period. Presence of symptoms was not associated with malignancy (data not shown).
Endoscopic Ultrasound Imaging Features
One or more high-risk cyst features were present in 77 patients on EUS (30.0%): 58 (22.6%) with cyst size ≥3 cm (12 resected), 6 (2.3%) with main pancreatic duct dilation (size ≥1 cm) (2 resected, 1 main duct IPMN not surgical candidate, 3 with chronic pancreatitis), 10 (3.9%) with thick wall (2 resected), 11 (4.3%) with mural nodules (4 resected), and 6 (2.3%) with solid component (4 resected, 2 malignant but not surgical candidates). Six of the 8 malignant cysts (75.0%) had high-risk features of cyst size ≥3 cm, main pancreatic duct dilation, thick wall, and/or solid component. Median cyst size among malignant lesions was 19 mm (IQR: 16-25 mm) which did not differ significantly from non-malignant cysts (median=19 mm, IQR: 14-26 mm; P=0.722). Thick wall (P=0.275), and nodularity (P=1.000) were not significantly associated with malignancy while solid component (P<0.001) and main pancreatic duct dilation (P=0.012) predicted malignancy (Table 1).
Cytology
Cytology was sent in 228 (88.7%) cases. In 123 cases (53.9%) cytology was nondiagnostic due to insufficient material. Among 105 cases with a cytologic diagnosis, 78 were benign (74.3%), 23 atypical (21.9%), 3 suspicious (2.9%), and 1 malignant (1.0%). Three of the 8 malignant cysts had suspicious (n=2) or malignant (n=1) cytologic diagnoses, which would have met criteria for surgical resection; cytology was associated with malignancy, which included suspicious and malignant diagnoses (P=0.001).
DNA Analysis
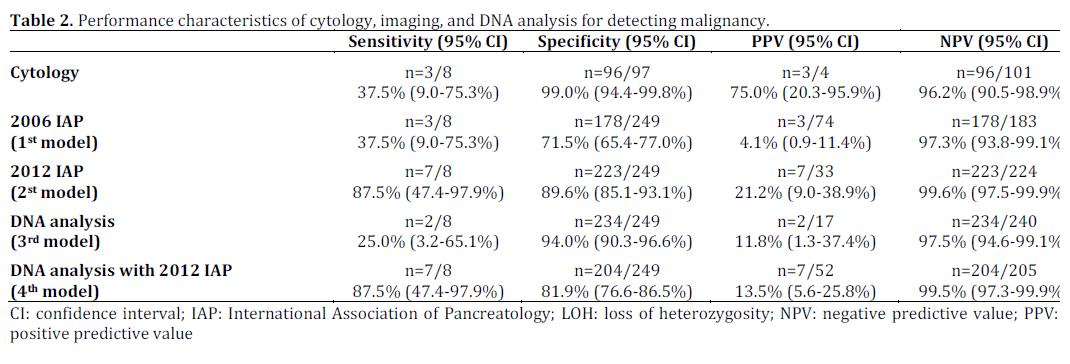
Sixty-one cases (23.7%) had evidence of k-ras mutation of which 17 (27.9%) were high amplitude; 83 (32.3%) had loss of heterozygosity with 5 of them (6.0%) high amplitude, and 6 cases (2.3%) had high amplitude k-ras followed by loss of heterozygosity mutations. The presence of a high amplitude k-ras mutation was not significantly associated with malignancy (2/8, 25.0% of malignant versus 15/249, 6.0% of non-malignant lesions; P=0.091) having 25.0% sensitivity, 94.4% specificity, 12.5% PPV, and 97.5% NPV. One malignant cyst had both high amplitude k-ras and LOH mutation to yield 12.5% sensitivity, 98.4% specificity, 20.0% PPV, and 97.2% NPV. No high amplitude loss of heterozygosity mutations were present in the malignant cysts. High DNA quantity was significantly associated with risk of malignant lesion: 1.4% (2/147) of low quantity was malignant, 2.5% (2/81) of moderate quantity, and 23.5% (4/17) of high quantity (P<0.001; Figure 1) with 12 cases without reported DNA quantity. DNA quality was not significantly associated (P=0.115) with risk of malignancy (3/168, 1.8%, for poor and borderline quality vs. 5/79, 6.3%, in good quality) Sensitivity and specificity for DNA mutations in pancreatic cyst aspirates as well as cytology, 2006 and 2012 IAP guidelines for detecting malignancy are presented in Table 2.
Figure 1. DNA quantity and malignancy.
Performance of Malignancy Prediction Models
Receiver operator curves for the 4 prediction models described in the Methods are presented in Figure 2. The AUC for the 2006 IAP guideline was 0.54 (95% CI: 0.47-0.60), 2012 IAP guideline 0.87 (95% CI: 0.82-0.91), DNA analysis alone 0.60 (95% CI: 0.53-0.66), and DNA analysis with 2012 guideline 0.84 (95% CI: 0.79-0.88). Comparisons among these 4 models demonstrated that the 2012 IAP guideline is superior to the 2006 IAP guideline and DNA analysis alone for predicting malignancy (P=0.004 and P=0.002, respectively), while comparable to the combined DNA with 2012 IAP guideline model (P=0.052). The combined DNA and 2012 IAP model was superior to both the 2006 IAP and DNA alone (P=0.001 and P=0.004, respectively). DNA analysis alone and the 2006 IAP guideline were not significantly different from each other (P=0.676).
Figure 2. Receiver operator curves for models predicting
malignancy in pancreatic cysts.
Malignant Cysts
By imaging criteria alone, 6 of the 8 (75.0%) malignant cysts met criteria for surgical resection. One additional cyst was resected because of malignant cyst cytology, and the final cyst was identified from malignant cytology of a peripancreatic lymph node. Four malignant cysts had DNA changes: 1 with both high amplitude k-ras and loss of heterozygosity mutations and high DNA quantity and 3 with only high DNA quantity. The patient with both k-ras and loss of heterozygosity mutations had a solid mass visualized on EUS with nondiagnostic cytology and would have undergone surgery based on the 2012 IAP criteria. Of the 3 patients with the only DNA finding of high DNA quantity, one patient had dilated main pancreatic duct over 1 cm, another patient had suspicious cyst fluid cytology, and the last patient had a malignant peripancreatic lymph node. Therefore, all patients with DNA changes would have been diagnosed with malignancy based on imaging and/or cytology findings.
DISCUSSION
In our experience of primarily incidental pancreatic cysts, commercial DNA analysis in the presence of high amplitude k-ras with loss of heterozygosity mutations yielded high specificity (98.4%) with low sensitivity for detecting malignancy in any pancreatic cystic lesion undergoing EUS-FNA. From DNA analysis, only high DNA quantity was associated with malignant cysts. Furthermore, DNA analysis did not add significant information beyond the 2012 IAP guideline, and in fact, the 2012 IAP guideline was superior to DNA analysis and the 2006 IAP guideline in detecting malignancy at the time of EUS-FNA.
Our results extend the findings from the PANDA study as well as two other smaller retrospective studies evaluating commercial DNA analysis in pancreatic cysts [12, 18, 19]. While the retrospective studies demonstrated increased frequency of k-ras mutation in malignant cysts, the prospective PANDA study concluded that both high amplitude k-ras and loss of heterozygosity mutations were needed to predict malignancy. Studies that evaluated DNA quantity also concluded its association with malignancy. In contrast to a recent study examining the ability of DNA analysis to predict long-term outcome of pancreatic cysts with a nonbenign course defined as not only development of malignancy, but also the diagnosis of a mucinous cyst or increase in cyst size [20], our study focuses on the value of commercial DNA analysis in determining the presence of malignancy at the time of EUS-FNA. Our study also uniquely examines the additional value of DNA analysis beyond the current standard of care with imaging and cytology.
In clinical practice, a pre-operative pathologic diagnosis of pancreatic cystic lesions is often not possible as evidenced by the high frequency of nondiagnostic cytology results (53.9%) present in the current study, which is consistent with previous reports [7, 10, 11]. Physicians therefore rely on imaging findings (CT, MRI, EUS) and the IAP guidelines to assess malignant potential of pancreatic cysts. However, studies have exposed the weaknesses of the 2006 guideline. Firstly, the IAP guidelines apply to mucinous cysts, and therefore assume the ability to distinguish preoperatively mucinous from non-mucinous cysts. A recent study demonstrated only 68% accuracy for preoperative diagnosis compared to surgical pathology [21]. In addition, while the negative predictive value of the 2006 IAP guideline for surgical resection of branch duct-IPMN and all pancreatic cysts ranges from 86% to 100%, the positive predictive value ranged from 14% to 21% [22, 23, 24]. Therefore, while the 2006 IAP guideline enables physicians to identify most branch duct-IPMN that can be followed without surgical resection, many patients will undergo unnecessary surgery. No currently published studies have evaluated the 2012 guideline.
The 2012 IAP guideline was superior to the 2006 guideline in detecting malignancy with higher sensitivity. This may be primarily due to cyst size no longer being a mandatory indication for resection. Nodularity was not associated with malignancy; however, most of the endoscopic ultrasounds in this study were performed before a recent study defining criteria to distinguish nodules from mucus, which demonstrated improvement in diagnostic accuracy of the endosonographers from 57% to 79% after education [25]. The majority (88%) of our malignant cases did meet 2012 IAP consensus guidelines for resection. The addition of commercial DNA analysis to the 2012 IAP guideline did not add significantly useful information beyond that already available through imaging and cytology, while supporting malignancy in 50% of cases, mainly from presence of high DNA quantity. An interesting finding of our study is that only 3.1% of our pancreatic cystic lesions were malignant. Therefore, the economics of applying the costly commercial DNA analysis to all pancreatic cystic lesions, especially incidental cysts, is uncertain when most of these lesions encountered in our clinical practice are benign. commercial DNA analysis should not be routinely used in evaluating all pancreatic cysts as it did not add clinically useful information beyond standard of care for detecting malignant cysts.
There were several limitations to the current study. First, as mentioned, not all patients had a confirmed histologic diagnosis. Our study design reflects the reality of clinical practice in which a precise preoperative classification of cysts is often not possible. We classified cysts without imaging evidence of progression after 1-year follow-up as benign lesions, which may have missed some potentially slow growing or premalignant lesions. However, the aim of our study was to evaluate the ability of DNA analysis to detect prevalent malignant (not premalignant) cysts at the time of EUS-FNA, as this would be a major determinant in the decision to pursue surgery as opposed to a surveillance strategy. Furthermore, a recent study confirmed that most asymptomatic pancreatic cysts referred for EUS do not undergo malignant transformation over 1 to 15 year follow-up with only 1 of 57 patients developing malignancy at 7 years [26]. We also applied the IAP guidelines to all pancreatic cysts and not only mucinous cysts, which again reflect the clinical reality that accurate preoperative distinction of cystic lesions is not necessarily feasible. While our number of malignant cysts is low, the fact that the 2012 IAP guidelines performed statistically significantly better than DNA analysis even with these small numbers, which reflects the clinical reality of managing primarily incidental pancreatic cysts, renders strong support for the guideline over DNA analysis.
Previous studies that have evaluated the accuracy of commercial DNA analysis for detection of malignant pancreatic cysts have primarily included only patients with histologic diagnoses confirmed by surgery [18, 19, 27]. This introduces a significant selection bias. The present study differs from previous reports by including outcomes from all patients that underwent cyst DNA analysis through use of longitudinal clinical data. A benefit of this approach is that the current study design reflects clinical practice and presents a more balanced assessment of the performance of DNA analysis.
In summary, in our large single center series of pancreatic cysts with imaging, cytology, cyst fluid, and commercial DNA analysis, we determined that while the rate of malignant cysts is low, nearly all these malignancies were diagnosed by current imaging criteria and cytology, which was superior to the older IAP guideline. Commercial DNA analysis offered confirmatory, but not additional useful information when combined with imaging and cytology as per the 2012 IAP guideline in determining presence of malignancy within pancreatic cysts.
Financial support
None
Potential conflict of interests
None
References
- Lee KS, Sekhar A, Rofsky NM, Pedrosa I. Prevalence of incidental pancreatic cysts in the adult population on MR imaging. Am J Gastroenterol 2010;105;2079-84. [PMID:20354507]
- Megibow AJ, Baker ME, Gore RM, Taylor A. The incidental pancreatic cyst. RadiolClin N Am 2011; 49: 349-59. [PMID:21333781]
- Lee LS, Clancy T, Kadiyala V, Suleiman S, Conwell DL. Interdisciplinary management of cystic neoplasms of the pancreas. Gastroenterology Research and Practice 2012;2012:513163. [PMID:23326260]
- Lee LS. Evaluation and management of pancreatic cystic lesions. J Clin Outcomes Manage 2013;20:129-42.
- Lee LS, Saltzman JR, Bounds BC, Poneros JM, Brugge WR, Thompson CC. EUS-guided fine needle aspiration of pancreatic cysts: a retrospective analysis of complications and their predictors. ClinGastroenterolHepatol 2005;3:231-6. . [PMID:15765442]
- Al-Haddad M, Schmidt MC, Sandrasegaran K, DeWitt J. Diagnosis and treatment of cystic pancreatic tumors. ClinGastroenterolHepatol2011;9:635-48. [PMID:21397725]
- Van der Waaij LA, van Dullemen HM, Porte RJ. Cyst fluid analysis in the differential diagnosis of pancreatic cystic lesions: a pooled analysis. GastrointestEndosc 2005;62:383-9. [PMID:16111956]
- De Jong K, van Hooft JE, Nio CY, Gouma DJ, Dijkgraaf MG, Bruno MJ, Fockens P. Accuracy of preoperative workup in a prospective series of surgically resected cystic pancreatic lesions. Scand J Gastroenterol 2012;47:1056-63. [PMID:22571417]
- Sainani NI, Saokar A, Desphpande V, Fernandez-del Castillo C, Hahn P, Sahani DV. Comparative performance of MDCT and MRI with MR Cholangiopancreatography in characterizing small pancreatic cysts. AJR 2009;193:722-31. [PMID:19696285]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centena BA, Szydio T, Regan S, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterol 2004;126:1330-6. [PMID:15131794]
- Maker A, Lee LS, Raut C, Clancy TE, Swanson RS. Cytology from pancreatic cysts has marginal utility in surgical decision making. Ann of SurgOnc 2008;15:3187-92. [PMID:18766406]
- Khalid A, Zahid M, Finkelstein SD, LeBlanc JK, Kaushnik N, Ahmad N, et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts: a report of the PANDA study. GastrointestEndosc 2009; 69:1095-102. [PMID:19152896]
- Garud S and Willingham F. Molecular analysis of cyst fluid aspiration in the diagnosis and risk assessment of cystic lesions of the pancreas. Clin Trans Sci 2012;5:102-7. [PMID:22376266]
- Tanaka M, Chari S, Adsay V, Fernandez-del Castillo C, Falconi M, Shimizu M, et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006;6:17-32. [PMID:16327281]
- Tanaka M, Fernandez-del Castillo C, Adsay V, Chari S, Falconi M, Jang JY, et al. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012;12:183-97. [PMID:22687371]
- Adsay NV, Fukushima N, Furukawa T, et al. Tumors of the pancreas. In: Bosman FT, Carneiro F, Hruban RH, Theise ND (eds). World Health Organization Classification of Tumours WHO Classification of Tumours of the Digestive System. WHO Press: Geneva, Switzerland, 2010, pp 279-337.
- DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988;44: 837-45. [PMID:3203132]
- Shen J, Brugge WR, DiMaio CJ, Pitman MB. Molecular analysis of pancreatic cyst fluid. Cancer Cytopathology 2009; 217-27. [PMID:19415731]
- Sreenarasimhaiah J, Lara LJ, Jazrawi SF, Barnett CC, Tang SJ. A comparative analysis of pancreas cyst fluid CEA and histology with DNA mutational analysis in the detection of mucin producing or malignant cysts. J Pancreas 2009;10:163-8. [PMID:19287110]
- Rockacy MJ, Zahid M, McGrath KM, Fasanella KE, Khalid A. Association between kras mutation, detected in pancreatic cyst fluid, and long-term outcomes of patients. ClinGastroenterolHepatol2013;11:425-9. [PMID:23267865]
- Correa-Gallego C, Ferrona CR, Thayer S, Wargo JA, Warshaw AL, Fernandez-del Castillo C. Incidental pancreatic cysts: do we really know what we are watching? Pancreatology 2010;10:144- 50. [PMID:20484954]
- Pelaez-Luna M, Chari ST, Smyrk TC, Takahashi N, Clain E, Levy MJ, et al. Do consensus indications for resection in branch duct intraductal papillary mucinous neoplasm predict malignancy? A study of 147 patients. Am J Gastroenterol 2007; 102:1759-64. [PMID:17686073]
- Tang RS, Weinberg B, Dawson DW, Reber H, Hines OJ, Tomlinson JS, et al. Evaluation of the guidelines for management of pancreatic branch-duct intraductal papillary mucinous neoplasm. Clin Gastro Hepatol 2008;6:815-9. [PMID:18602036]
- Sawhney MS, Al-Bashir S, Curry MS, Brown A, Chuttani R, Pleskow DK, et al. International consensus guidelines for surgical resection of mucinous neoplasms cannot be applied to all cystic lesions of the pancreas. ClinGastroenterolHepatol 2009;7:1373- 6. [PMID: 19577006]
- Zhong N, Zhang L, Takahashi N, Shalmiyev V, Canto MI, Clain JE, et al. Histologic and imaging features of mural nodules in mucinous pancreatic cysts. ClinGastroenterolHepatol 2012;10:192-8. [PMID: 21982970]
- Lahav M, Maor Y, Avidan B, Novis B, Bar-Meir S. Nonsurgical management of asymptomatic incidental pancreatic cysts. ClinGastroenterolHepatol2007;5:813-7. [PMID: 17544874]
- Sawhney MS, Devarajan S, O’Farrel P, Cury MS, Kundu R, Vollmer CM, et al. Comparison of carcinoembryonic antigen and molecular analysis in pancreatic cyst fluid. GastrointestEndosc 2009;69:1106-10. [PMID:19249035]



