Keywords
Severe congenital heart disease; Hypoplastic left heart syndrome; Bilateral pulmonary artery banding; Balloon angioplasty; Interventional cardiology
Introduction
Although the surgical outcomes of hypoplastic left heart syndrome and its variants have improved in recent years, bilateral pulmonary artery banding is generally performed as a less invasive hybrid first-stage palliation in high-risk neonates [1,2]. Despite a significant improvement in mortality and morbidity rates associated with neonatal operations involving cardiopulmonary bypass, morbidity continues to occur to some extent owing to the immaturity and fragility of neonatal organs. Neonatal cardiopulmonary bypass can cause brain injury, which can result in severely impaired motor and cognitive neurodevelopmental outcomes, although notable advances and innovations have been made in cardiopulmonary bypass, surgical techniques, and instruments [3,4]. Moreover, patients with severe coronary heart disease (CHD) have significantly impaired early neurodevelopmental outcomes, although the mortality rate after a hybrid procedure is similar to that after the Norwood procedure [5].
At our institution, to avoid neonatal cardiopulmonary bypass, we perform a modified version of bilateral pulmonary artery banding combined with planned percutaneous pulmonary artery balloon dilatation at the banding sites approximately 1-2 months after banding [termed as flow-adjustable bilateral pulmonary artery banding (FABPAB)] as first-stage palliation for patients with severe ductus-dependent congenital heart disease, including hypoplastic left heart syndrome variants. Subsequently, between 4 and 5 months of life, when the infants have a body weight between 4 kg and 5 kg, we typically perform the Norwood procedure for biventricular conversion or the Norwood and bidirectional Glenn procedures for univentricular palliation as a second-stage operation, as previously reported [6- 8]. However, some patients exhibit progressive stenosis of the bilateral pulmonary artery banding sites even after debanding and surgical reconstruction of the bilateral pulmonary artery banding sites because of the thickness of vessel endothelial cells, and this worsens the prognosis of these patients [9]. In this study, we aimed to evaluate the efficacy of balloon dilatation after bilateral pulmonary artery banding for the treatment of severe congenital heart disease that depends on patent ductus arteriosus for systemic circulation.
Materials and Methods
Patients
We performed a retrospective review of 27 patients (15 boys and 12 girls) with congenital heart disease that dependent on patent ductus arteriosus for systemic circulation, who underwent bilateral pulmonary artery banding and received ductal stents or maintenance with prostaglandin E1 at our institution between October 2007 and December 2013. Of these 27 patients, 16 underwent pulmonary artery balloon dilatation after bilateral pulmonary artery banding. Clinical perioperative and outcome data were obtained from the patient medical records. All patients or their representatives provided written informed consent to participate in this study. We analysed the patient clinical course and data of the patients, including body weight, peripheral oxygen saturation, brain natriuretic peptide levels, peripheral pulmonary arterial growth, and the necessity of surgical intervention after pulmonary artery balloon dilatation at bilateral pulmonary artery banding sites.
Bilateral pulmonary artery banding technique
Bilateral pulmonary artery banding was performed in the operating room under general anesthesia. Preoperatively, we prepared banding tapes, which consisted of 0.1 mm expanded polytetrafluoroethylene sheets. Each patch was doubled and trimmed to a width of 2 mm to 3 mm. After a standard median sternotomy and minimal mobilization of branches of the pulmonary artery, the right and left pulmonary arteries were individually encircled with the banding tapes. Then, the banding tapes were adjusted to the appropriate tightness by placing Weck Hemoclips (Teleflex Inc., Wayne, PA, USA) horizontally in order to achieve a partial pressure of oxygen in arterial blood of around 45 mm Hg at 40% to 50% of the fraction of inspired oxygen during surgery. First, a Hemoclip was placed on the mattress suture, and then, the bands were tightened by adding Hemoclips in sequence until the target oxygen level was reached.
Pacing wires and pericardial drain tubes were placed. The sternum was closed, unless the patient had considerable intraoperative dysrhythmia or anasarca.
Pulmonary artery balloon dilatation
Representative images from cardiac angiography during balloon dilatation are presented in Figure 1. At approximately 1-2 months after bilateral pulmonary artery banding, we performed pulmonary artery balloon dilatation. For balloon dilatation, we first used a Judkins right-type catheter and guidewire to insert the catheter into the bilateral peripheral pulmonary artery. Then, balloon dilatation was performed using high-pressure, noncompliant balloon catheters at each bilateral pulmonary artery banding site to increase pulmonary blood flow without exerting unnecessary artery tension on adjacent tissues. The pulmonary artery was dilated by approximately 50% in diameter, and oxygen saturation was elevated by approximately 10% and reached around 75% to 85%.
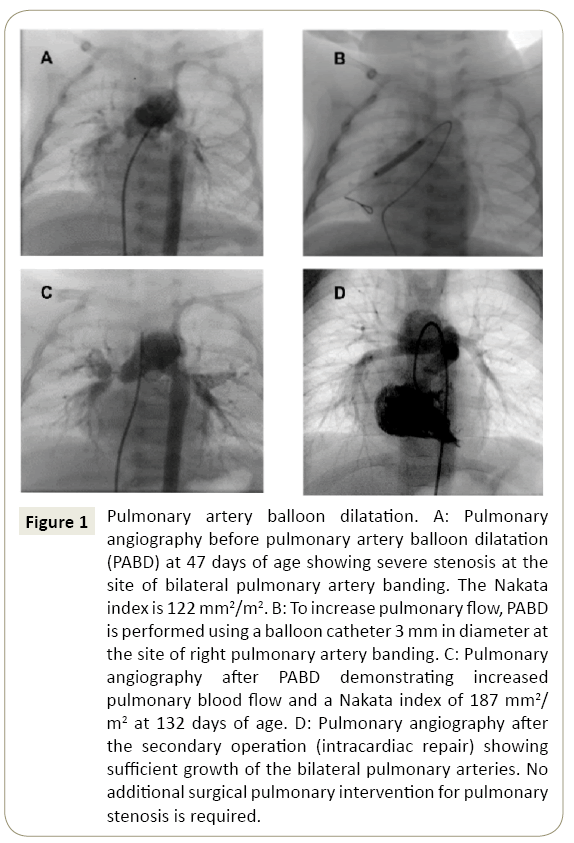
Figure 1: Pulmonary artery balloon dilatation. A: Pulmonary angiography before pulmonary artery balloon dilatation (PABD) at 47 days of age showing severe stenosis at the site of bilateral pulmonary artery banding. The Nakata index is 122 mm2/m2. B: To increase pulmonary flow, PABD is performed using a balloon catheter 3 mm in diameter at the site of right pulmonary artery banding. C: Pulmonary angiography after PABD demonstrating increased pulmonary blood flow and a Nakata index of 187 mm2/ m2 at 132 days of age. D: Pulmonary angiography after the secondary operation (intracardiac repair) showing sufficient growth of the bilateral pulmonary arteries. No additional surgical pulmonary intervention for pulmonary stenosis is required.
Statistical analysis
Data are presented as number and percentage, mean ± standard deviation, or median (range). Dichotomous variables were analyzed using Fisher’s exact test, and continuous variables were analyzed using the Student’s t-test. All statistical analyses were performed using EZR (Division of Hematology, Saitama Medical Center, Jichi Medical University, Saitama, Japan), a graphic user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) designed to add statistical functions frequently used in biostatistics. A p-value of <0.05 was considered statistically significant.
Results
Patient population
Of the 16 patients who underwent pulmonary artery balloon dilatation, four had classic hypoplastic left heart syndrome. The remaining 12 patients had congenital heart disease with the following diagnoses: ventricular septal defect with coarctation of the aorta (n=2), interrupted aortic arch (n=4), single ventricle with hypoplastic aortic arch (n=3), persistent truncus arteriosus (n=2), and unbalanced atrioventricular septal defect (n=1). The characteristics of these eligible patients, including those with significant extracardiac anomalies and genetic syndromes, are presented in Table 1. Nine patients required univentricular repair, and seven required biventricular repair.
| Patient Number |
Diagnosis |
Extracardiac complication |
Gestational age (weeks) |
Body weight at bPAB(g) |
Age at bPAB (d) |
Age at PAB (d) |
Balloon diameter (mm) |
| 1 |
Persistent truncus arteriosus |
|
38 |
2670 |
9 |
55 |
3 |
| 2 |
Persistent truncus arteriosus |
22q11.2 del. |
39 |
2480 |
3 |
36 |
3 |
| 3 |
IAA (type B), severe AS |
22q11.2 del. |
27 |
2400 |
4 |
61 |
4 |
| 4 |
IAA (type A), VSD, AS |
|
41 |
2820 |
6 |
51 |
3 |
| 5 |
IAA (type B), hypoplastic arch |
|
40 |
2600 |
12 |
47 |
3 |
| 6 |
IAA (type B), VSD, AS |
22q11.2 del. |
37 |
2510 |
8 |
27 |
3 |
| 7 |
CoA, severe AS, VSD |
VACTERL association |
37 |
2100 |
18 |
128 |
3 |
| 8 |
CoA, VSD |
|
38 |
2213 |
19 |
70 |
4 |
| 9 |
HLHS (MA/AA) |
|
36 |
2800 |
9 |
46 |
3 |
| 10 |
HLHS (MA/AA) |
|
41 |
2886 |
5 |
32 |
3 |
| 11 |
HLHS (MS/AA) |
|
39 |
3200 |
4 |
30 |
2.5 |
| 12 |
HLHS (MS/AS) |
|
38 |
2710 |
4 |
56 |
3.5 |
| 13 |
SV, hypoplastic arch |
Heterotaxy |
37 |
2650 |
10 |
71 |
4 |
| 14 |
SV, hypoplastic arch |
|
40 |
3400 |
2 |
67 |
4 |
| 15 |
SV, sub AS, hypoplastic arch |
|
37 |
4053 |
8 |
15 |
2.5 |
| 16 |
Unbalanced AVSD, CoA |
|
38 |
2492 |
5 |
62 |
4 |
bPAB, bilateral pulmonary artery banding; PABD, pulmonary artery banding dilatation; del., deletion; IAA, interruption of aortic arch; AS, aortic stenosis; VSD, ventricular septal defect; CoA, coarctation of aorta; HLHS, hypoplastic left heart syndrome; MA, mitral atresia; AA, aortic atresia; MS; mitral stenosis; SV, single ventricle; AVSD, atrioventricular septal defect
Table 1: Patient characteristics and clinical data at pulmonary artery balloon dilatation.
The ductus arteriosus was maintained with continuous prostaglandin E1 administration and ductal stenting, and restrictive arterial septal defects were dilated with balloon atrial septostomy.
Bilateral pulmonary artery banding
The median age at bilateral pulmonary artery banding was 6 days (range, 2-19 days), and the median body weight was 2.75 kg (range, 2.10 kg to 4.05 kg). The polytetrafluoroethylene sheet strips were cut longitudinally to a width of 2 mm to 3 mm. The median circumferences of the bands were 10 mm (range, 9 mm to 11.5 mm) for right pulmonary artery banding and 10 mm (range, 9 mm to 1 mm) for left pulmonary artery banding. None of the patients had intraoperative arrhythmia or anasarca precluding sternal closure.
After the bilateral pulmonary artery banding procedure, the mean peripheral oxygen saturation measured using an oximeter was 85.6% ± 4.5% (range, 74% to 91%), and the mean partial pressure of oxygen in arterial blood was 46.4 mmHg ± 7.8 mmHg (range, 35.0 mmHg to 62.2 mmHg) under the condition of 50% (range, 21% to 100%) oxygen concentration in the operating room.
Pulmonary artery balloon dilatation
After bilateral pulmonary artery banding, 16 patients underwent pulmonary artery balloon dilatation at a mean age of 53.4 ± 25.9 days after birth. The mean body weight at the time of pulmonary artery balloon dilatation was 3.5 kg ± 0.6 kg. Among all patients, 11 patients who did not undergo dilation showed difficulty with regard to expansion of the banding sites and/or apparent peripheral pulmonary over-circulation in a pulmonary artery angiogram. Pulmonary artery balloon dilatation was performed using one of four different types of angioplasty catheters for peripheral vasculature or the coronary artery, including Sterling™, SAVVY®, Jackal OTW, Maverick™. The mean balloon diameter was 3.2 mm ± 0.5 mm (range, 2.5 mm to 4.0 mm) with pressure ranging from 6 to 10 atm. Percutaneous oxygen saturation increased significantly from 74.9% ± 6.2% to 85.6% ± 4.5% (p<0.01; Figure 2A) and brain natriuretic peptide levels increased significantly from 143.8 pg/ml ± 100.7 pg/ml to 618.6 pg/ml ± 510.7 pg/ml (p<0.01) after balloon dilatation. However, the levels in patients who did not undergo balloon dilatation did not increase significantly (from 273.3 pg/ml ± 387.6 pg/ml to 277.6 pg/ml ± 334.4 pg/ml, p=0.979; Figure 3A). All of the procedures were uneventful, and the final angiography did not reveal any sign of complications, such as dissection and aneurysm. Cardiac catheterizations before the second-stage operation were performed at 126 ± 14.8 days. The Nakata index of the patients who underwent balloon dilatation significantly increased from before to after pulmonary artery balloon dilatation (from 130.6 mm2/m2 ± 51.1 mm2/m2 to 243 mm2/m2 ± 93.5 mm2/m2, p<0.01). However, that of patients who did not undergo balloon dilatation did not increase significantly (from 179.4 mm2/m2 ± 147.6 mm2/ m2 to 186.6 mm2/m2 ± 75.5 mm2/m2, p=0.902; Figure 3B).
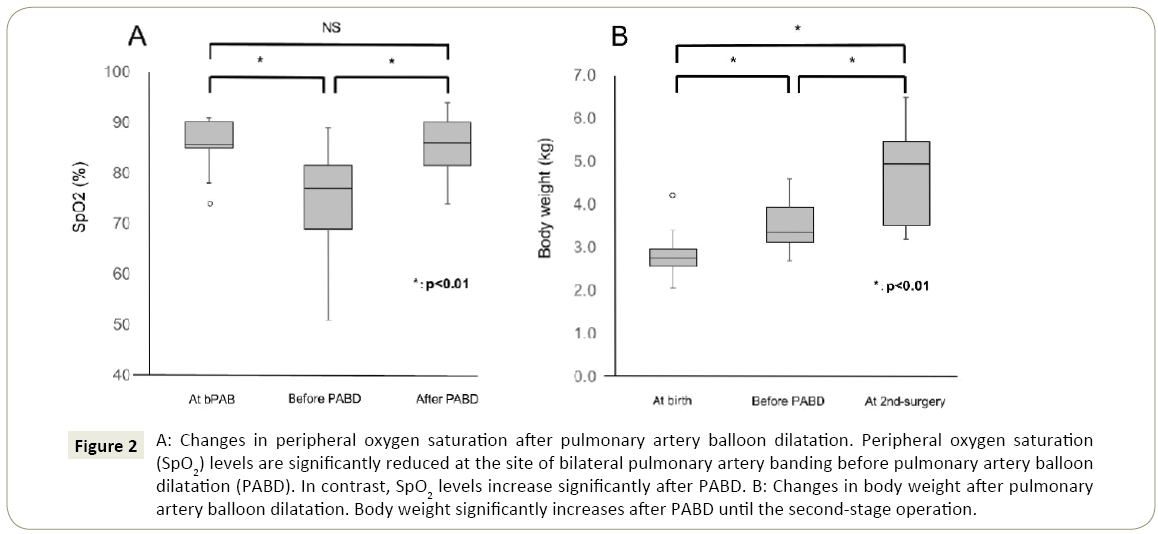
Figure 2: A: Changes in peripheral oxygen saturation after pulmonary artery balloon dilatation. Peripheral oxygen saturation (SpO2) levels are significantly reduced at the site of bilateral pulmonary artery banding before pulmonary artery balloon dilatation (PABD). In contrast, SpO2 levels increase significantly after PABD. B: Changes in body weight after pulmonary artery balloon dilatation. Body weight significantly increases after PABD until the second-stage operation. Figure
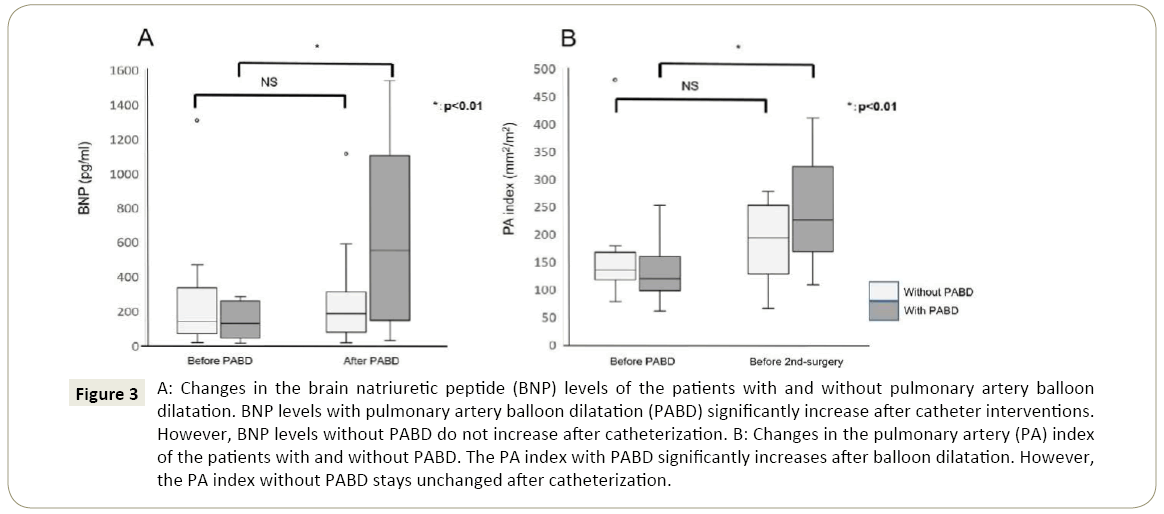
Figure 3: A: Changes in the brain natriuretic peptide (BNP) levels of the patients with and without pulmonary artery balloon dilatation. BNP levels with pulmonary artery balloon dilatation (PABD) significantly increase after catheter interventions. However, BNP levels without PABD do not increase after catheterization. B: Changes in the pulmonary artery (PA) index of the patients with and without PABD. The PA index with PABD significantly increases after balloon dilatation. However, the PA index without PABD stays unchanged after catheterization.
Follow-up
Patient data at catheterization after bilateral pulmonary artery banding and at the second-stage operation are summarized in Table 2. All patients survived until the second-stage operation. We performed biventricular repair in seven patients and univentricular repair in nine patients. The mean age at the second-stage operation was 126 ± 14.8 days, and the mean body weight was 4.8 kg ± 1.1 kg. The significant increase in body weight is shown in Figure 2B (p<0.01). After the neonatal period, we were able to perform the Norwood-Glenn procedure as a second-stage operation in three patients. Of these patients, two had a good clinical course and one died from heart failure after the Glenn procedure.
| Patient Number |
Age at second-stage operation (d) |
Body weight at second-stage operation (kg) |
Second-stage operation method |
UVR/BVR |
Outcome |
| 1 |
124 |
6.1 |
Rastelli |
BVR |
Rastelli |
| 2 |
243 |
6.5 |
Rastelli |
BVR |
Rastelli |
| 3 |
122 |
4.9 |
Norwood |
BVR |
Rastelli |
| 4 |
76 |
3.5 |
Arch repair + VSD cl. |
BVR |
ICR |
| 5 |
126 |
4.9 |
Norwood |
BVR |
Norwood |
| 6 |
81 |
3.44 |
Norwood |
BVR |
Norwood |
| 7 |
206 |
5.7 |
Norwood |
UVR |
TCPC |
| 8 |
105 |
3.5 |
CoA repair + VSD cl. |
BVR |
ICR |
| 9 |
103 |
5.1 |
Norwood |
UVR |
TCPC |
| 10 |
141 |
4.68 |
Norwood |
UVR |
Glenn |
| 11 |
50 |
3.2 |
Norwood |
UVR |
Death |
| 12 |
145 |
5 |
DKS + Glenn |
UVR |
Death |
| 13 |
160 |
5.4 |
DKS + Glenn |
UVR |
TCPC |
| 14 |
157 |
5.3 |
Arch repair + MPAB |
UVR |
TCPC |
| 15 |
108 |
6 |
DKS + Glenn |
UVR |
Glenn |
| 16 |
75 |
3.54 |
Arch repair + MPAB |
UVR |
Death |
UVR, univentricular repair; BVR, biventricular repair; VSD, ventricular septal defect; CoA, coarctation of aorta; ICR, intracardiac repair; TCPC, total cavopulmonary connection; DKS, Damus-Kaye-Stansel procedure; MPAB, main pulmonary artery banding
Table 2: Patient clinical data after pulmonary artery balloon dilatation.
With regard to surgical interventions for the pulmonary artery after the second-stage operation, we compared the patients who did and those who did not undergo pulmonary artery balloon dilatation. We needed to perform only one intrapulmonary artery septation procedure (6.3%) among the 16 patients who underwent pulmonary artery balloon dilatation. Conversely, we needed to perform five surgical interventions, including three Blalock-Taussig shunts, one intrapulmonary artery septation, and one additional pulmonary artery plasty (45%), among the 11 patients who did not undergo pulmonary artery balloon dilatation. There was a significant difference between these groups (p<0.05; Table 3).
| |
Surgical intervention for the pulmonary artery |
| + (n [%]) |
- (n) |
PABD (+)
(16 patients) |
1 (6.3)† |
15 |
| IPAS 1 |
|
PABD (-)
(11 patients) * |
5 (45.5) |
6 |
Additional BT shunt (+ LPA stent) 3
IPAS 1
Pulmonary artery plasty 1 |
|
*including six patients with interruption of the aortic aorta or coarctation of the aorta, four with hypoplastic left heart syndrome, and one with a single ventricle. †p<0.05, PABD (+) versus PABD (-). PABD, pulmonary artery banding dilatation; IPAS, intrapulmonary-artery septation; LPA, left pulmonary artery
Table 3: Surgical intervention after the second-stage operation.
Discussion
Although the surgical outcomes of the Norwood operation for hypoplastic left heart syndrome and its variants have dramatically improved in recent years, bilateral pulmonary artery banding is generally performed in high-risk neonates as a less invasive hybrid stage 1 palliation because it avoids neonatal cardiopulmonary bypass [8,10,11]. High-risk neonates undergoing the stage 1 Norwood procedure have a mortality rate of approximately 10% to 20% [12].
Our results showed that the FABPAB strategy using bilateral pulmonary artery banding followed by balloon dilatation for the management of classic hypoplastic left heart syndrome and its variants is feasible and effective, and that the application of pulmonary artery dilatation at banding sites is safe. We demonstrated successful staged treatment strategies for severe congenital heart disease involving both univentricular and biventricular defects. Our strategy achieves a significant increase in pulmonary blood flow and pulmonary artery diameter, and these result in significant elevations of brain natriuretic peptide levels and the Nakata index, and reduces pulmonary surgical interventions after the second-stage operation. There were no complications, including death, related to angioplasty using pulmonary artery balloon dilatation, although brain natriuretic peptide levels significantly increased after pulmonary artery balloon dilatation. The main merit of this strategy is that bilateral pulmonary artery banding is less invasive than a neonatal operation involving cardiopulmonary bypass in the newborn period, and it is possible to adjust pulmonary artery blood flow according to body size [6].
Recently, a more refined and collaborative effort to implement a hybrid strategy, consisting of bilateral pulmonary artery banding with continuous lipo-prostaglandin E1 administration or ductal stenting, has emerged as an alternative form of palliation for hypoplastic left heart syndrome and its associated anomalies [13-15]. In addition, Akintuerk et al. [14] reported a successful combined stage-two surgical procedure, involving Fontan circulation rather than hybrid palliation, and this approach continues to gain interest. Increased awareness of patient deterioration because of inter stage morbidity, a higher risk of associated comorbidities, and technical issues associated with stage-two reconstruction, require a longitudinal and comprehensive analysis to analyze the overall success of management strategies in these patients.
At our institution, we perform bilateral pulmonary artery banding in the first week of life as a less invasive first-stage palliation to avoid cardiopulmonary bypass and hypothermic circulatory arrest in the neonatal period. We then perform cardiopulmonary bypass later in life, at an age when it is possible to establish circulation in series. In such patients, it is very important to wait for a gain in body weight facilitated by pulmonary artery balloon dilatation to reduce the risks of the second-stage operation. However, bilateral pulmonary artery banding, in which constrictive tapes encircle both pulmonary arteries, frequently entails post-debanding residual pulmonary artery stenosis, resulting from pulmonary arterial intimal proliferation. This influences the postoperative prognosis of severe CHD [8]. We performed additional pulmonary artery balloon dilatation at 1 or 2 months after banding using Sterling™ Balloon Dilatation Catheters with a median diameter of 3 mm. This contributed to the induction of significant pulmonary arterial growth before the second-stage operation. Consequently, the frequency of additional surgical interventions for the pulmonary artery after the second-stage operation significantly decreased.
Limitations
The main limitation of this strategy is the necessity of hospitalization for more than 6 months, from birth to the secondstage operation, if continuous prostaglandin E1 infusion is used rather than ductus arteriosus stenting, which in turn increases the expense of care and treatment. The present study has several limitations. As this was a retrospective study and included a small number of patients, an additional prospective trial is needed to confirm the therapeutic effectiveness of this strategy. The availability of data was also variable. Patients were not managed with a standardized approach, and therefore, we could not make an early decision on the timing of the second-stage operation in patients with risk factors reported previously [16-19], such as low birth weight, prematurity, septic condition, small ascending aorta, atrioventricular valve regurgitation of more than moderate grade, pulmonary congestion because of a restrictive foramen ovale, and dysfunction of the systemic ventricle.
Conclusions
Although further studies involving larger groups of patients are warranted, this study revealed that our FABPAB strategy is a feasible and valid clinical option for the treatment of severe CHD, particularly for the development of pulmonary artery banding sites. Moreover, our strategy, when correctly employed, not only reduces the short-term morbidity and mortality associated with the procedures required to correct CHD, but also reduces the middle-term morbidity after second-stage operation, including the need for additional surgical interventions, such as pulmonary angioplasty.
References
- BachaEA, Daves SHardin J, Abdulla RI, Anderson J, et al. (2006) Single-ventricle palliation for high-risk neonates: The emergence of an alternative hybrid stage I strategy. J Thorac Cardiovasc Surg 131: 163-171.
- Gomide M, Furci B, Mimic B, Brown KL, Hsia TY, et al. (2013) Rapid 2-stage Norwood I for high-risk hypoplastic left heart syndrome and variants. J Thorac Cardiovasc Surg 146: 1146-1151.
- Hirsch JC, Jacobs ML, Andropoulos D, Austin EH, Jacobs JP, at al. (2012) Protecting the infant brain during cardiac surgery: A systematic review. Ann Thorac Surg 94: 1365-1373.
- Hsia TY, Gruber PJ (2006) Factors influencing neurologic outcome after neonatal cardiopulmonary bypass: What we can and cannot control. Ann Thorac Surg 81: 2381-2388.
- Knirsch W, Liamlahi R, Hug MI, Hoop R, von Rhein M, et al. (2012) Mortality and neurodevelopmental outcome at 1 year of age comparing hybrid and Norwood procedures. Eur J Cardiothorac Surg 42: 33-39.
- Kobayashi T, Miyamoto T, Kobayashi T, Ikeda K, Okamoto H, et al. (2010) Staged repair of truncus arteriosus with interrupted aortic arch: Adjustablepulmonary artery banding. Ann Thorac Surg 89: 973-975.
- Miyamoto T, Yoshii T, Inui A, Ozaki S (2013) Staged repair for aortic arch reconstruction and intracardiac repair following bilateralpulmonary artery banding in 3 critical patients. Interact Cardiovasc Thorac Surg 16: 892-894.
- Yoshimoto A, Miyamoto T, Ozaki S, Kobayashi T, Kobayashi T (2013) Flow-adjustable bilateral pulmonary artery banding in the neonatal period for severe congenital heart diseases. Gen Thorac Cardiovasc Surg 61: 340-344.
- Achiwa I, Hirata Y, Kimura M, Nakazawa A, Nakano N, et al. (2011) New technique of bilateral pulmonary artery banding using half-closed surgical clips:An experimental study. Kyobu Geka 64: 798-802.
- Kaneko Y, Achiwa I, Morishita H, Shibata M (2014) Bilateral pulmonary artery banding with ligation clips: A novel technique resistant to residual stenosis. J Thorac Cardiovasc Surg 147: 1984-1985.
- Guleserian KJ, Barker GM, Sharma MS, Macaluso J, Huang R, et al. (2013) Bilateral pulmonary arterybanding for resuscitation in high-risk, single-ventricle neonates and infants: a single-center experience.J Thorac Cardiovasc Surg 145: 206-213
- Ghanayem NS, Allen KR, Tabbutt S, Atz AM, Clabby ML, et al. (2012) Interstage mortality after the Norwood procedure: Results of the multicenter Single Ventricle Reconstruction trial. J Thorac Cardiovasc Surg 144: 896-906.
- Pizarro C, Derby CD, Baffa JM, Murdison KA, Radtke WA. (2008) Improving the outcome of high-riskneonates with hypoplastic left heart syndrome: hybrid procedure or conventional surgical palliation? Eur J Cardiothorac Surg 33: 613-618.
- Akintuerk H, Michel-Behnke I, Valeske K, Mueller M, Thul J, et al. (2002) Stenting of the arterial duct and banding of the pulmonary arteries: basis for combined Norwood stage I and II repair in hypoplastic left heart. Circulation 105: 1099-1103.
- Caldarone CA, Benson L, Holtby H, Li J, Redington AN, et al. (2007) Initial experience with hybridpalliation for neonates with single-ventricle physiology. Ann Thorac Surg 84: 1294-1300.
- Ishii Y, Inamura N, Kayatani F, Iwai S, Kawata H, et al. (2014) Evaluation of bilateral pulmonary artery banding for initial palliation in single-ventricle neonates and infants: Risk factors for mortality before the bidirectional Glenn procedure. Interact Cardiovasc Thorac Surg 19: 807-811.
- Daebritz SH, Nollert GD, Zurakowski D, Zurakowski D, Khalil PN, et al. (2000) Results of Norwood stage I operation: Comparison of hypoplastic left heart syndrome with other malformations. J Thorac Cardiovasc Surg 119: 358-367.
- Weinstein S, Gaynor JW, Bridges ND, Wernovsky G, Nontenegro LM, et al. (1999) Early survival of infants weighing 2.5 kilograms or less undergoing first-stage reconstruction for hypoplastic left heart syndrome. Circulation 100: 167-170.
- Cortese F, Scicchitano P, Gesualdo M, Filaninno A, de Giorgi E, et al. (2016) Early and Late Infections in Newborns: Where Do We Stand? A Review. Pediatr Neonatol 57: 265-273.

