What Did We Know Before 2010 ASCO Annual Meeting?
The American Cancer Society estimated that approximately 42,470 new cases of pancreatic cancer were diagnosed in the United States in 2009 with 35,240 deaths [1]. Of the new cases, only approximately 20% would be considered resectable and would be given adjuvant chemotherapy. Results from the Charité Onkologie (CONKO-001) trial have shown that compared to placebo, adjuvant chemotherapy with gemcitabine demonstrated a median recurrence-free survival of 14 months, median overall survival of 22 months, and a survival rate of 20% at 5 years [2]. This landmark paper established the cornerstone of resected pancreatic cancer treatment.
What Did We Learn from 2010 ASCO Annual Meeting?
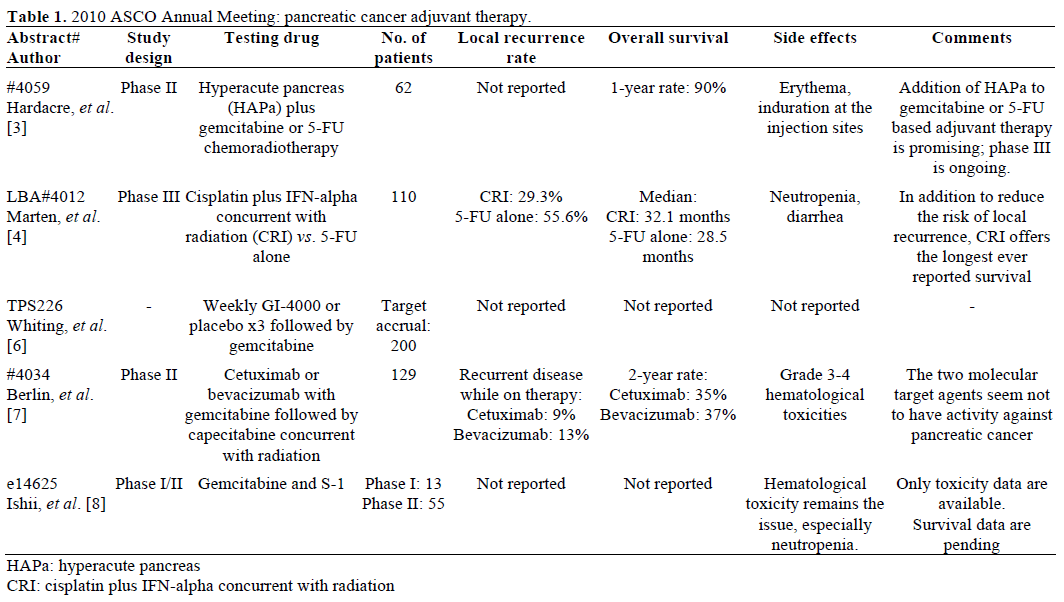
This review article will update you with the material presented at the 2010 ASCO Annual Meeting (Table 1) regarding adjuvant therapy of pancreatic carcinoma.
Incorporation of Immunotherapy into Conventional Chemotherapy or Chemoradiation
Completely resected pancreatic cancer represents a compelling model of minimal residual disease for which many investigators believe immunotherapy may be the treatment choice.
Hardacre et al. (Abstract #4059) presented the data of an allogeneic immunotherapy in addition to standard therapies such as gemcitabine based chemotherapy or 5-fluorouracil (5-FU) based chemoradiation in patients with resected pancreatic cancers [3]. A total of 62 patients were enrolled; the majority (81%) had lymph node positive disease. The current median progression free survival is 17 months, and one year overall survival rate reaches 96%. The survival benefit of adding hyperacute pancreas to standard therapy is very promising. A phase III multi-institutional (more than 50), open-label, randomized trial has been initiated.
Another pancreatic adjuvant trial (CapRi; Abstract LBA4012) tested chemoimmunoradiotherapy vs. 5- FU/leucovorin alone [4]. The former includes cisplatin, IFN-alpha concurrent with radiation (CRI); this regimen was developed by Picozzi et al. and tested in the ACOSOG trial [5]. There was no significant survival difference between the two arms (32.1 and 28.5 months, respectively); however, unplanned subset analyses favored CRI for R1 and N1 disease. In addition, the CRI treatment, as expected, significantly reduced the local recurrence rate from 55.6% to 29.3% (P=0.014). The chemoimmunoradiotherapy arm demonstrated much lower incidence of severe toxicity compared to the historical data from ACOSOG Z05031 trial [5], which was closed early because of toxicity. More importantly, this trial demonstrated a positive correlation between response to single IFN-alpha treatment and longer survival. Whether the response to IFN is a prognostic or predictive marker needs to be investigated. Several concerns about this trial were brought up during the meeting. Lack of stratification may have biased these results and masked a positive effect of chemoradioimmunotherapy. Differences in the toxicity profile compared to the ACOSOG Z05031 trial [5] need to be explained.
Ras mutations occur commonly in the development of pancreas cancer. GI-4000 is an immunotherapy using targeted molecular immunogens (Tarmogens) to specifically activate immune response and attack cells expressing ras mutations. Whiting et al. (Abstract TPS226) are conducting a trial to evaluate the efficacy of gemcitabine with or without GI-4000 in the adjuvant setting [6]. The trial is designed for patients to receive weekly GI-4000 or placebo x3 followed by gemcitabine weekly x3 every 28 days for a total of 6 cycles. All patients are maintained on monthly GI-4000 or placebo for up to 5 years. This trial is ongoing with no results reported at this meeting. It would be interesting to see any additional benefit of an immunotherapy beyond gemcitabine alone.
Incorporation of Molecular Target Agents with Cytotoxic Agents
Combining molecular target agents with conventional cytotoxic agents remain a popular thought. Berlin et al. (ECOG 2204; Abstract #4034) presented an interesting randomized phase II trial to investigate the feasibility of cetuximab or bevacizumab in combination with standard adjuvant chemotherapy followed by capecitabine-based concurrent chemoradiation [7]. Molecular agents were given throughout therapy. Onehundred and twenty-nine eligible patients were randomized to either arm (cetuximab or bevacizumab plus gemcitabine followed by capecitabine-based chemoradiation). Primary endpoint was toxicity; secondary endpoints were disease free survival and overall survival. No severe toxicities were observed in the study; however, more than 10% patients recurred during the adjuvant treatment period. Disease free survival or overall survival was not superior to historical data derived from gemcitabine monotherapy. Neither arm demonstrated enough clinical activity to warrant further study. Therefore, the investigators believe there is no role for cetuximab or bevacizumab as part of adjuvant therapy. Development of novel agents may be necessary to make a change.
Combination of Conventional Cytotoxic Agents
S-1 has been proved to be highly active in advanced or metastatic pancreatic cancer. A Japanese study group (Abstract e14625) presented a phase I/II trial of gemcitabine plus S-1 in the adjuvant setting [8]. All enrolled patients received i.v. gemcitabine (mg/m2/week) on day 1 and oral S-1 (mg/m2/day) twice daily from days 1 to 7 every 14 days for 12 cycles at the following dose levels of gemcitabine/S-1: 800/60 (level 0), 1,000/60 (level 1) and 1,000/80 (level 2). Thirteen patients were enrolled in the phase I part. Level 0 was determined to be maximal tolerated dose. A total of 55 patients were enrolled onto phase II part. Severe neutropenia is a concern in this gemcitabine/S-1 combination. Whether S-1 has similar promising antitumor effect in pancreatic cancer as in gastric cancer will have to be evaluated based on survival data.
Role of CT Scan, Symptoms And Tumor Marker CA 19-9
A retrospective review conducted by Vaccaro et al. (Abstract #4113) assessed the use of CT scan, symptoms and tumor marker CA 19-9 as surveillance tools to detect early recurrent disease [9]. Data from a total of 476 patients with pancreatic cancer resections from 1998 to 2008 were reviewed. Only 15% of recurrences were observed on CT scan in the absence of symptoms. However, 85% of recurrences were associated with symptoms and/or rising tumor marker levels. Asymptomatic patients with a normal CA 19-9 had a significantly prolonged overall survival compared to either asymptomatic or symptomatic patient with rising CA 19-9 (18 vs. 10 vs. 5 months, respectively; P<0.0001).
Discussion
The optimal adjuvant approach for patients with resected pancreatic cancer remains unclear. The National Comprehensive Cancer Network (NCCN) guidelines offer a variety of approaches including systemic chemotherapy with agents such as gemcitabine, 5-fluorouracil, capecitabine or gemcitabine followed by 5-fluorouracil based chemoradiotherapy [10]. Whether one is superior to the other needs to be validated in large randomized trials. Intensive research is currently being conducted to evaluate the role of immunotherapy in the adjuvant setting. The rationale favoring immunotherapy in the adjuvant setting lies on the theory of eradicating any microscopic disease after a complete resection. The IFN-alpha containing regimen showed the longest ever reported over survival; final survival data from other groups are pending. Overall, immunotherapy represents an appealing approach. More randomized trials are certainly needed to confirm the results and further clarify the role of radiation in this setting. Several trials included radiation therapy concurrent or after chemotherapy; however, the survival benefit of radiation remains unclear.
GI-4000 approach focuses on selectively targeting pancreatic cancer cells expressing a ras mutation. It is well known that the vast majority of pancreatic cancers have mutated ras. This yeast derived immunogen induces an endogenous T-cell response which may confer a role in both the active therapeutic as well as the preventative setting.
EGFR and VEGF, two commonly used monoclonal antibodies (cetuximab and bevacizumab) with demonstrated anti-tumor effects in other solid tumors such as head, neck and colorectal, appear to have no activity in resected pancreatic cancer. These results reinforce the message that development of novel agents is critical to provide durable benefit and tolerable toxicity.
Conflict of interest The authors have no potential conflicts of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer
Statistics, 2009. CA Cancer J Clin 2009; 59:225-49. [PMID
19474385]
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K,
et al. Adjuvant chemotherapy with gemcitabine vs observation in
patients undergoing curative-intent resection of pancreatic cancer: a
randomized controlled trial. JAMA 2007; 297:267-77. [PMID
17227978]
- Hardacre JM, Mulcahy MF, Talamonti M, Obel JC, Rocha Lima
CS, Safran H, et al. Effect of hyperacute immunotherapy in addition
to standard adjuvant therapy for resected pancreatic cancer on
disease-free and overall survival: Preliminary analysis of phase II
data. J Clin Oncol 2010; 28(15 Suppl):4059.
- Marten A, Schmidt J, Debus J, Harig S, Lindel K, Klein J, et al.
CapRI: Final results of the open-label, multicenter, randomized phase
III trial of adjuvant chemoradiation plus interferon-?2b (CRI) versus
5-FU alone for patients with resected pancreatic adenocarcinoma
(PAC). J Clin Oncol 2010; 28(18 Suppl):LBA4012.
- Picozzi VJ, Abrams RA, Traverso LW, O’Reilly EM, Greeno E,
Martin RC, et al. ACOSOG Z05031: Report on a multicenter, phase
II trial for adjuvant therapy of resected pancreatic cancer using
cisplatin, 5- FU, and alpha-interferon. J Clin Oncol 2008; 26(15
Suppl):4505.
- Whiting SH, Muscarella P, Rosemurgy A, Fisher WE, Richards
DA, Harrell FE Jr, et al. A randomized, placebo-controlled,
multicenter phase II adjuvant trial of the efficacy, immunogenicity,
and safety of GI-4000 plus gemcitabine versus gemcitabine alone in
patients with resected pancreatic cancer with activating ras
mutations. J Clin Oncol 2010; 28(15 Suppl):TPS226.
- Berlin J, Catalano PJ, Feng Y, Lowy AM, Blackstock AW,
Philip PA, et al. ECOG 2204: An intergroup randomized phase II
study of cetuximab (Ce) or bevacizumab (B) in combination with
gemcitabine (G) and in combination with capecitabine (Ca) and
radiation (XRT) as adjuvant therapy (Adj Tx) for patients (pts) with
completely resected pancreatic adenocarcinoma (PC). J Clin Oncol
2010; 28(15 Suppl):4034.
- Ishii H, Ueno H, Kosuge T, Matsuyama Y, Saiura A, Nakao A,
et al. A phase I/II trial of gemcitabine and S-1 therapy in patients
with resected pancreatic cancer: Japanese Study Group of Adjuvant
Therapy for Pancreatic Cancer (JSAP-03). J Clin Oncol 2010;
28(Suppl):e14625.
- Vaccaro V, Fleming JB, Wolff RA, Evans DB, Tamm EP, Crane
CH, et al. Role of surveillance CT scans in resected PC: Correlation
with CA19-9 and symptoms. J Clin Oncol 2010; 28(15 Suppl):4113.
- National Comprehensive Cancer Network. NCCN Clinical
Practice Guidelines in Oncology (NCCN Guidelines™). Pancreatic
Adenocarcinoma. V.I.2010. Fort Washington, PA, USA.

