Keywords
Biological Markers; Neoplastic Cells, Circulating; Neuroendocrine Tumors; Pancreatic Neoplasms; placenta growth factor
Abbreviations
CgA: chromogranin A; mTOR: mammalian target of rapamycin; NCCN: National Comprehensive Cancer Network; NET: neuroendocrine tumor; pNET: pancreatic neuroendocrine tumor; PlGF: placental growth factor
What Did We Know Before the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting?
Neuroendocrine tumors (NETs) consist of a diverse group of tumors composed of cells showing neuroendocrine cell differentiation (secretory granules), a subset of which can be further classified by their dominant secretory products. Although it was thought that the neuroendocrine cells that give rise to NETs migrated from the neural crest to the gut endoderm, it is now apparent that enteropancreatic neuroendocrine cells originate from multipotent stem cells that give rise to all epithelial cell types in the gastrointestinal tract and pancreas [1]. NETs show heterogeneity in morphologic, functional and clinical features [2]. Due to the non-uniform nature of this disease reflected by large differences in survival rates with regard to primary tumor site, histologic degree of differentiation and cell type of tumor, it has been challenging to understand the true natural history of NETs. Ongoing efforts [3], to establish large registries will help improve our understanding of the incidence and natural history of this disease. A subset of NETs involving the pancreas previously termed islet cell tumors or islet cell carcinomas are designated pancreatic NETs (pNETs) Although pNET represent a small percentage of all pancreatic tumors (1.3%), the prevalence of these tumors is significant (9.9% of all pancreatic tumors) and the incidence is increasing [4]. It is important to note that the incidence of pNETs is significantly underestimated in tumor registries including the Surveillance, Epidemiology and End Results (SEER) program which include only malignant neoplasms. In tertiary oncology centers, the majority of patients with malignant pNETs represent advanced stage tumors with approximately 65% of patients presenting with unresectable or metastatic disease [5]. There is substantial variability in progression and survival among patients with NET, in one large series tumor necrosis and metastasis were associated with poorer disease free survival but the role of other features was not significant [6]. Similar to NETs, pNETs can be “functional” and associated with significant symptoms including through the secretion of insulin (thus reflecting a former name- insulinomas) but also other hormones. Traditionally, pNETs were thought to be associated with higher rates of functionality than other NETs; however, the limited data available has made it difficult to generalize and more recent experience suggests that more of these tumors are non-functioning [7]. In addition to characteristics of the tumor and levels of functional markers, there are molecular markers that may have additional prognostic significance. Several inherited syndromes associated with pNETs, including multiple endocrine neoplasia type 1 (MEN1), von Hippel- Lindau disease (vHL), neurofibromatosis 1 (NF1), and the tuberous sclerosis complex, are associated with mutations in well-studied oncogenes and tumor suppressor genes [8]. Although these syndromes account for only a subset of pNETs, some of these genetic abnormalities are also seen in sporadic pNETs [9] and they have helped in the quest to develop novel therapies. Besides the role of mammalian target of rapamycin (mTOR) in many of the above syndromes, there is evidence that aberrant expression of several tyrosine kinase receptors and overexpression of vascular endothelial growth factor (VEGF) are important in the development of pNET [10, 11].
At the 2012 ASCO Annual Meeting, several abstracts were presented addressing the role of established and novel biomarkers on predictive and prognostic parameters of pNET. These reports are reviewed and summarized here.
What We Learned at the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting
Multi-Institutional Cohorts
As previously noted there is a large effort through seven National Comprehensive Cancer Network (NCCN) sites to develop a comprehensive set of data about patients with NET. In this data set [3], 53% of NETs were classified as carcinoid while 26% were classified as pNET.
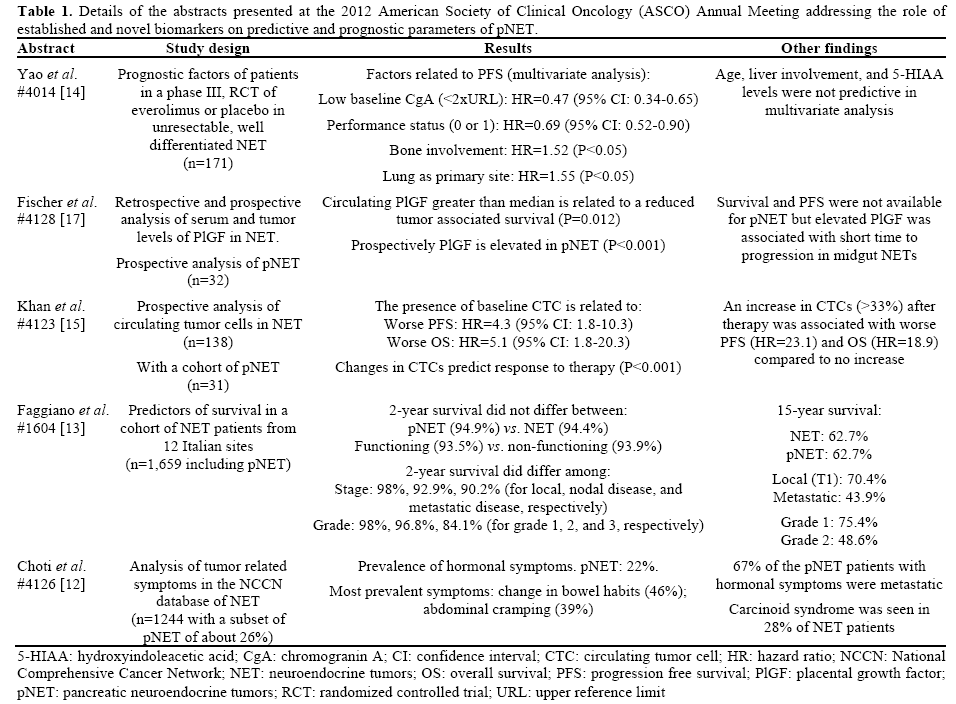
In Abstract #4126 [12], Choti et al. reported data regarding tumor related symptoms from the above mentioned NCCN database. The authors classified tumors as being pNET, NET (or carcinoid), pheochromocytoma, and NOS (not otherwise specified.) Among the patients with NET and pNET tumors the rate of symptoms due to the carcinoid syndrome (in NET) or hormonal syndrome (in pNET) was 28% and 22% respectively. In NET this is higher than expected from historical reports while in pNET the number is somewhat lower than expected. In patients with carcinoid syndromes the most common symptoms were abdominal cramping, change in bowel habits, and flushing. In patients with hormonal syndrome related to pNET the most common symptoms were change in bowel habit and abdominal cramping. Although most patients with NET and pNET who presented with symptoms had distant disease at the time of diagnosis, a substantial minority (26% in NET and 33% in pNET) did not have distant disease and the authors point out the importance of recognizing tumor related symptoms in those with localized disease.
In Abstract #1604 [13], Faggiano et al. looked at a large set of NET cases from several Italian centers. The authors found that short term survival (2-year) did not differ between various sites of origin of the NET with pancreatic (pNET), gastrointestinal, and lung showing similar survival. They did note that even at this early stage survival was poorer in patients with higher grade (grade 3) disease. They reported a similar finding for long term survival (15-year) among the different sites of origin but poorer in those with higher grade disease. Patients with higher stage disease (metastatic disease) also showed poorer short term and long term survival compared to those with more localized disease (Table 1).
RAD001 in Advanced Neuroendocrine Tumors (RADIANT)-2 Trial
In Abstract #4014 [14], Yao et al. looked at predictive biomarkers in the randomized, phase III, RADIANT-2 trial which compared the mTOR inhibitor everolimus with placebo in patients with advanced NET. Patients with chromogranin A (CgA) levels less than 2 times the upper limit of normal or hydroxyindoleacetic acid (5-HIAA) levels below the median level were found to have significantly longer progression free survival compared to patients with elevated levels of either biomarker. In multivariate analysis the prognostic benefit of lower chromogranin remained statistically significant; a patient’s functional status (as measured by the WHO performance status classification) was also associated with improved progression free survival. In this multivariate analysis the presence of bone involvement or primary disease site in the lungs predicted for worse progression free survival.
Novel Markers
In Abstract #4123 [15], Khan et al. investigated the role of circulating tumor cells as a biomarker in NETs including a sample of pNET (31 of 138; 22%). The authors enrolled patients with advanced NETs who were commencing systemic or local therapy. They found that patients with one or more circulating tumor cells (CTC) detected by the Cell Search® (Veridex LLC, Raritan, NJ, USA) technology were more likely to have worse progression free and overall survival [16]. In multivariate analysis the hazard ratio for survival in patients with one or more circulating tumor cell was 5.1 (95% confidence interval: 1.5-7.3).
Additionally they compared samples measured prior to beginning therapy and 3-5 weeks after starting therapy and found that an increase of more than 33% in the number of circulating tumor cells was a strong predictor of poor response to therapy with worse progression free survival and overall survival (Table 1).
In Abstract #4128 [17], Fischer et al. evaluated placental growth factor (PlGF) as a prognostic biomarker in NET. PlGF is a homolog of the vascular endothelial growth factor (VEGF) which is recognized to be overexpressed in NET. The VEGF pathway is an important target for drug therapy in pNET with both the approved agent sunitinib (a multi-targeted tyrosine kinase inhibitor) and experimental therapies with bevacizumab (a monoclonal antibody against the VEGF pathway) which are thought to work through this pathway. The authors measured PlGF levels in serum and in tumor samples via immunohistochemistry. They found that PlGF levels were elevated in pNET samples and serum compared to control pancreatic tissue and control serum. Prospective investigation validated this finding of elevated serum PlGF levels in both pNET and NETs. The authors also reported that there was a suggestion that elevated PlGF levels are correlated with shorter time to progression (at least in NETs) and that this warrants further prospective evaluation as a predictive biomarker.
Discussion
Pancreatic neuroendocrine tumors represent a unique subset of NETs with increasing incidence and distinct pattern of symptoms and dissemination. These tumors were traditionally associated with a high rate of hormonal symptoms and a relatively indolent course though they were relatively refractory to therapy. The report by Choti et al. [12] found that only 22% of pNET patients presented with hormonal symptoms. Additionally a substantial proportion of the patients with functional tumors (33%) were non-metastatic suggesting the need to expand the classic description of pNET. Faggiano et al. [13] reported that short- and long-term survival was similar between patients with NET and pNET but identified tumor stage and grade as important predictors of survival. Yao et al. [14] identified predictors of progression free survival in patients randomized on a large clinical trial. Together these observations help expand the tools available to guide patients when diagnosed with pNET. Novel biomarkers are also being explored and there is encouraging data regarding the potential role of serum levels of PlGF (Fischer et al. [17]) and circulating tumor cell count (Khan et al. [15] in predicting outcomes and potentially response to chemotherapy. These reports from the 2012 ASCO Annual Meeting summarize the progress being made in identifying prognostic and predictive biomarkers in pNET. Notably these researchers have identified biomarkers that can now be incorporated into clinical practice and illustrated the ongoing research that will help guide management of this difficult disease.
Conflict of interest
The authors have no potential conflicts of interest
References
- Barker N, van Es JH, Kuipers J, et al. Identification of stem cells in small intestine and colon by marker gene Lgr5. Nature 2007;449:1003-7.
- Jensen RT. Carcinoid tumors and the carcinoid syndrome. In: De Vita VTJ, Lawrence, T., Rosenberg, S.A., ed. Cancer: Principles and Practice of Oncology. Philadelphia: Lippincott, Williams, and Wilkins; 2008.
- Zornosa CC, Choti MA, Bobiak S, et al. Baseline demographics of neuroendocrine tumor patients presenting to seven National Comprehensive Cancer Network (NCCN) institutions: Development of a multi-institutional outcomes database. J Clin Oncol 30, 2012 (suppl; abstr e14551).
- Yao JC, Eisner MP, Leary C, et al. Population-based study of islet cell carcinoma. Ann Surg Oncol 2007;14:3492-500.
- Yao JC, Hassan M, Phan A, et al. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008;26:3063-72.
- Hochwald SN, Zee S, Conlon KC, et al. Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol 2002;20:2633-42.
- Vagefi PA, Razo O, Deshpande V, et al. Evolving patterns in the detection and outcomes of pancreatic neuroendocrine neoplasms: the Massachusetts General Hospital experience from 1977 to 2005. Arch Surg 2007;142:347-54.
- Jensen RT, Berna MJ, Bingham DB, Norton JA. Inherited pancreatic endocrine tumor syndromes: advances in molecular pathogenesis, diagnosis, management, and controversies. Cancer 2008;113:1807-43.
- Zikusoka MN, Kidd M, Eick G, Latich I, Modlin IM. The molecular genetics of gastroenteropancreatic neuroendocrine tumors. Cancer 2005;104:2292-309.
- Zhang J, Jia Z, Li Q, et al. Elevated expression of vascular endothelial growth factor correlates with increased angiogenesis and decreased progression-free survival among patients with low-grade neuroendocrine tumors. Cancer 2007;109:1478-86.
- Terris B, Scoazec JY, Rubbia L, et al. Expression of vascular endothelial growth factor in digestive neuroendocrine tumours. Histopathology 1998;32:133-8.
- Choti MA, Bobiak S, Strosberg JR, et al. Prevalence of functional tumors in neuroendocrine carcinoma: An analysis from the NCCN NET database. J Clin Oncol 30, 2012 (suppl; abstr 4126)
- Faggiano A, Grimaldi F, Manzoni M, et al. Long-term survival and prognostic factors in neuroendocrine tumors: Results from a large multicenter study. J Clin Oncol 30, 2012 (suppl; abstr 1604).
- Yao JC, Hainsworth JD, Wolin EM, et al. Multivariate analysis including biomarkers in the phase III RADIANT-2 study of octreotide LAR plus everolimus (E+O) or placebo (P+O) among patients with advanced neuroendocrine tumors (NET). J Clin Oncol 30, 2012 (suppl; abstr 4014).
- Khan MS, Tsigani T, Garcia-Hernandez J, Hartley JA, Caplin ME, Meyer T. Circulating tumor cells as prognostic and predictive markers in neuroendocrine tumors. J Clin Oncol 30, 2012 (suppl; abstr 4123)
- Riethdorf S, Fritsche H, Muller V, et al. Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: a validation study of the Cell Search system. Clin Cancer Res 2007;13:920-8.
- Fischer C, Pape U-F, Neumann T, et al. Prognostic relevance of circulating PIGF levels in patients with neuroendocrine tumors. J Clin Oncol 30, 2012 (suppl; abstr 4128)

