Anastasios Dimou1, Kostas N Syrigos2, Muhammad Wasif Saif3
1Department of Medicine, Albert Einstein Medical Center. Philadelphia, PA, USA.
2Oncology Unit, Third Department of Medicine, University of Athens. Athens, Greece.
3Section of GI Cancers and Experimental Therapeutics, Tufts University School of Medicine. Boston, MA, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Section of GI Cancers and Experimental Therapeutics
Tufts University School of Medicine and Tufts Cancer Center
800 Washington Street, #245
Boston, MA 02111; USA
Phone: +1-617.636.5627
Fax: +1-617.636.8538
E-mail: wsaif@tuftsmedicalcenter.org
Keywords
bevacizumab; MK 2206; Neuroendocrine Tumors; pasireotide; temsirolimus
What Did We Know Before the 2012 American Society of Clinical Oncology (ASCO) Annual Meeting?
Tumors with neuroendocrine differentiation comprise of a diverse set of malignant neoplasms that share common pathogenic, morphologic and clinical features. Neuroendocrine neoplastic cells are believed to originate from pluripotent stem cells, they contain secretory granules and they often present with syndromes that are linked to secreted hormones [1]. Pancreatic neuroendocrine tumors (pNETs), formerly known as islet cell tumors, account for 1% of the newly diagnosed pancreatic cancers and are further classified as functional or non-functional on the basis of hormone secretion [2]. Most of the tumors in the former group are insulinomas which are usually benign, followed by glucagonomas, gastrinomas, somatostatinomas, VIPomas, polypeptidomas and cholecystokininomas. Based on histology they are divided in three categories, well differentiated/low grade, well differentiated/intermediate grade and poorly differentiated/high grade. Most of pNETs are sporadic, but they can be associated with germline missense and nonsense mutations in the context of multiple endocrine neoplasia type 1 (MEN1) syndrome [3].
Treatment is largely dependent on the functional status and the stage. For resectable disease, surgery is generally recommended. In the case of locoregional unresectable and metastatic disease, recent trials indicate that sunitinib [4], everolimus [5] and somatostatin analogs [6] offer a progression free survival benefit. Preclinical data support the effect of these drugs on the natural history of pNETs: the vascular endothelial growth factor (VEGF) pathway which is targeted by sunitinib, the mammalian target of rapamycin (mTOR) which is inhibited by everolimus and the somatostatin receptors are often aberrantly expressed in pNETs [7, 8, 9]. In addition to the biologically targeted therapies, conventional chemotherapy with combinations of 5-FU, doxorubicin and streptozocin, capecitabine and oxaliplatin or temozolomide have been reported to cause objective responses in 23% to 70% of the patients with pNETs in phase II studies [10, 11].
In this review we summarize the data about the novel agents in pNETs presented in the recent 2013 ASCO Annual Meeting.
What We Learned at the American Society of Clinical Oncology (ASCO) Annual Meeting
MK-2206 in Metastatic Neuroendocrine Tumors (Abstract #e15133 [12])
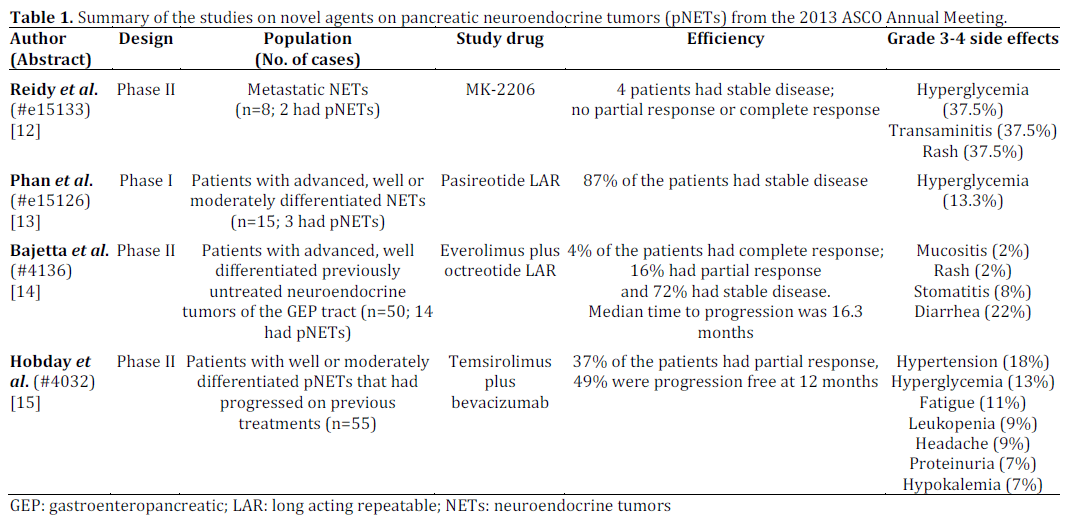
The AKT inhibitor MK-2206 was used in a phase II study for the treatment of metastatic well differentiated neuroendocrine tumors that had progressed on other treatments [12]. The investigators recruited eight patients two of whom had pNETs. In addition they studied archived tissue from the tumors for biomarker analysis. Overall, one durable response in a patient with thymic carcinoid was noted whereas three patients experienced transient stabilization of their disease. The most common side effects were hyperglycemia, transaminitis and rash. Translational analysis with next generation sequencing in the patient who responded to treatment did not reveal any relevant biomarker with the potential to serve as a companion diagnostic.
Somatostatin Analogs (Abstracts #e15126 [13] and #4136 [14])
Pasireotide is a novel somatostatin analog that binds more broadly to somatostatin receptors (SSTR1-3 and 5) compared to the traditional octreotide and lanreotide (SSTR2). Phan et al. [13] reported preliminary results from a phase I study of pasireotide in advanced neuroendocrine tumors. In this report, 3 patients with pNETs were recruited out of a total of 15 patients. The rest of the patients in the study suffer from either small intestinal or lung neuroendocrine tumors. Most of the patients had been treated already with other somatostatin analogs. The study was designed to escalate the dose of the study drug beginning from 80 mg up to 220 mg. At the time the preliminary results were reported, there were 6 patients who were treated with 80 mg and 9 patients treated with 120 mg. No dose limiting toxicity was noted. Most common side effects were included hyperglycemia (87%) including 2 patients with grade 3 hyperglycemia, diarrhea (53%), abdominal pain (47%), nausea (40%), anemia (33%), and fatigue (33%).
Although both everolimus and somatostatin analogs have been approved for the treatment of pNETs, the combination of the two has not been well studied. Patients with well differentiated metastatic neuroendocrine tumors who were treatment naïve, received everolimus and octreotide in the approved doses in a phase II trial performed by the Italian Trials in Medical Oncology group [14]. One third of the patients had pNETs while the rest of the neuroendocrine tumors had a small bowel, lung or unknown primary. The study enrolled 50 patients and objective response rate was the primary endpoint in the study: two patients achieved a complete response and an additional eight patients had a partial response. Disease control rate, as defined by the patients who experienced either a complete or partial response or had stable disease, was 92%. Patients progressed after a median of 16.2 months. Major side effects included one patient with grade 4 mucositis, one patient with grade 3 rash, four patients with grade 3 stomatitis and eleven patients with grade 3 diarrhea.
Combination of mTOR and VEGF Pathways in pNETs (Abstract #4032 [15])
Hobday et al. reported the updated data on a phase II study where patients with well or moderately differentiated pNETs were treated with the combination of temsirolimus and bevacizumab [15]. A total of 55 patients who had progressed on previous treatments were enrolled in the study. Primary endpoints were the objective response rate and progression free survival. In the 55 patients who were evaluated for the former endpoint, the response rate by using the Response Evaluation Criteria in Solid Tumors (RECIST) criteria was 37%. About half of the 49 patients (49%) who were evaluated for progression free survival, were progression free at 12 months. Grade 3-4 side events included hypertension, hyper
glycemia, fatigue, leukopenia, headache, proteinuria, and hypokalemia.
A summary of the reviewed studies is presented in Table 1.
Discussion
There have been a number of abstracts in the recent 2013 ASCO Annual Meeting that considered novel agents in the treatment of pancreatic neuroendocrine tumors. The frequent overexpression of the PI3K/AKT/mTOR pathway in pNETs provides rationale for the use of AKT inhibition. In addition, the approved drug everolimus abrogates mTORC2 but not mTORC1. Reidy et al. reported the effect of the AKT inhibitor MK-2206 in patients with metastatic neuroendocrine tumors [12]. Although MK-2206 was found to be well tolerated in this study, conclusion about the efficacy of the drug is limited given the small number of patients and the even smaller number of the study subjects who had a pancreatic variant.
The phase I study by Phan et al. [13] is consistent with results from earlier studies [16] about the safety of the novel somatostatin analog pasireotide that has a broader affinity for somatostatin receptors compared to octreotide or lanreotide. Interestingly, the drug was well tolerated even at the dose of 120 mg while there was a correlation between the dose and the serum levels. Bajetta et al. reported the results from a phase II study with the combination of everolimus and long acting repeatable (LAR) octreotide [14]. Data on progression free survival look promising when compared to the historical data on everolimus and are consistent with the progression free survival that was achieved with this combination in a phase III trial in patients with neuroendocrine tumors and carcinoid syndrome [17]. However, more research on this combination is required.
Conclusions
In conclusion, in the 2013 ASCO Annual Meeting we saw the updated results from the phase II study of the temsirolimus plus bevacizumab combination in pNETs [15]. Results are consistent with the preliminary interim analysis that was presented in the 2012 ASCO Annual Meeting [18]; the combination of mTOR plus VEGF inhibition arises as a promising strategy in patients with advanced non resectable pNETs. Further studies are needed to show whether the combination is superior to sequential monotherapy.
Conflict of interest
The authors have no potential conflict of interest
References
- Bergsland, E.K., The evolving landscape of neuroendocrinetumors. Semin Oncol, 2013. 40(1): p. 4-22.
- Yao, J.C., M.P. Eisner, C. Leary, C. Dagohoy, A. Phan, A. Rashid,et al., Population-based study of islet cell carcinoma. Ann SurgOncol, 2007. 14(12): p. 3492-500.
- Gulati, A.P., B. Krantz, R.A. Moss, W.N. Moyal, D.A. Tsushima,K.B. Mowatt, et al., Treatment of multiple endocrine neoplasia1/2 tumors: case report and review of the literature. Oncology,2013. 84(3): p. 127-34.
- Raymond, E., L. Dahan, J.L. Raoul, Y.J. Bang, I. Borbath, C.Lombard-Bohas, et al., Sunitinib malate for the treatment ofpancreatic neuroendocrine tumors. N Engl J Med, 2011. 364(6):p. 501-13.
- Yao, J.C., M.H. Shah, T. Ito, C.L. Bohas, E.M. Wolin, E. VanCutsem, et al., Everolimus for advanced pancreaticneuroendocrine tumors. N Engl J Med, 2011. 364(6): p. 514-23.
- Rinke, A., H.H. Muller, C. Schade-Brittinger, K.J. Klose, P.Barth, M. Wied, et al., Placebo-controlled, double-blind,prospective, randomized study on the effect of octreotide LAR inthe control of tumor growth in patients with metastaticneuroendocrine midgut tumors: a report from the PROMID StudyGroup. J Clin Oncol, 2009. 27(28): p. 4656-63.
- Wolin, E.M., PI3K/Akt/mTOR pathway inhibitors in thetherapy of pancreatic neuroendocrine tumors. Cancer Lett, 2013.335(1): p. 1-8.
- Chen, M., M. Van Ness, Y. Guo, and J. Gregg, Molecularpathology of pancreatic neuroendocrine tumors. J GastrointestOncol, 2012. 3(3): p. 182-8.
- Oberg, K., Genetics and molecular pathology ofneuroendocrine gastrointestinal and pancreatic tumors(gastroenteropancreatic neuroendocrine tumors). Curr OpinEndocrinol Diabetes Obes, 2009. 16(1): p. 72-8.
- Kulke, M.H., Systemic therapy for advanced pancreaticneuroendocrine tumors. Semin Oncol, 2013. 40(1): p. 75-83.
- Reidy-Lagunes, D.L., Systemic therapy for advancedpancreatic neuroendocrine tumors: an update. J Natl Compr CancNetw, 2012. 10(6): p. 777-83.
- Reidy-Lagunes, D.L., M.C. Pietanza, M. Segal, M. Capanu, andL. Saltz, A phase II clinical and translational study of MK-2206 inpatients with metastatic neuroendocrine tumors (NETs). J ClinOncol 31, 2013 (suppl; abstr #e15133).
- Phan, A., E.M. Wolin, J.A. Chan, J.M. Huang, M. Hudson, G.Hughes, et al., Phase I dose-escalation study of pasireotide LAR inpatients with advanced neuroendocrine tumors. J Clin Oncol 31,2013 (suppl; abstr #e15126).
- Bajetta, E., L. Catena, N. Fazio, S. Pusceddu, P. Biondani, G.Blanco, et al., Everolimus in combination with octreotide LAR asTable 1. Summary of the studies on novel agents on pancreatic neuroendocrine tumors (pNETs) from the 2013 ASCO Annual Meeting.
- Hobday, T.J., R. Qin, M. Moore, D.L. Reidy-Lagunes, J.R.Strosberg, H.L. Kindler, et al., Multicenter phase II trial oftemsirolimus (TEM) and bevacizumab (BEV) in pancreaticneuroendocrine tumor (pNET). J Clin Oncol 31, 2013 (suppl;abstr #4032).
- Chan, J.A., D.P. Ryan, A.X. Zhu, T.A. Abrams, B.M. Wolpin, P.Malinowski, et al., Phase I study of pasireotide (SOM 230) andeverolimus (RAD001) in advanced neuroendocrine tumors.Endocr Relat Cancer, 2012. 19(5): p. 615-23.
- Pavel, M.E., J.D. Hainsworth, E. Baudin, M. Peeters, D. Horsch,R.E. Winkler, et al., Everolimus plus octreotide long-actingrepeatable for the treatment of advanced neuroendocrinetumours associated with carcinoid syndrome (RADIANT-2): arandomised, placebo-controlled, phase 3 study. Lancet, 2011.378(9808): p. 2005-12.
- Hobday TJ, Qin R, Reidy DL, Moore MJ, Strosberg JR, KaubischA, et al. Multicenter phase II trial of temsirolimus (TEM) andbevacizumab (BEV) in pancreatic neuroendocrine tumor (PNET).J Clin Oncol 2012; 30(Suppl.): Abstract #4047.

