Amit Javed1, Sujoy Pal1, Gaurav Nitin Chaubal1, Nihar Ranjan Dash1, Pramod Kumar Garg2, Peush Sahni1, Tushar Kanti Chattopadhyay1
Departments of 1Gastrointestinal Surgery and 2Gastroenterology,
All India Institute of Medical Sciences. New Delhi, India
- *Corresponding Author:
- Amit Javed
Department of Gastrointestinal Surgery, All India Institute of
Medical Sciences, Ansari Nagar, New Delhi, 110029 India
Phone: +91-11.2658.8500 Ext 3461; +91-99.9905.2393
Fax: +91-11.2658.8663
E-mail: javedamitdr@gmail.com
Received April 9th, 2010 - Accepted May 25th, 2010
Keywords
Cysts; Echinococcosis; Pancreas; Pancreatic Cyst
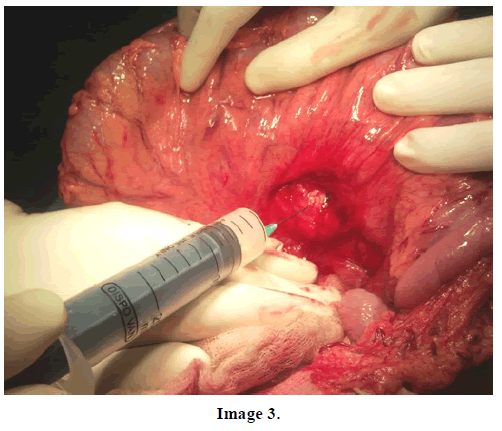
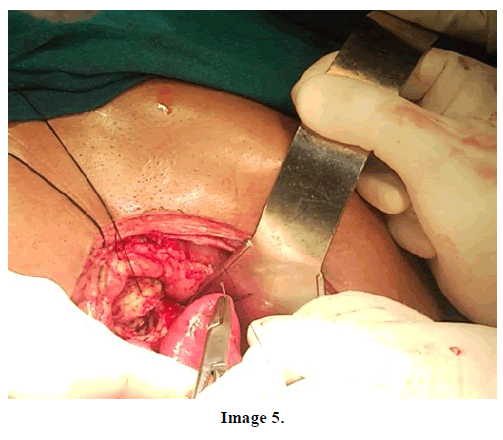
A 20-year-old male presented to the Department of Gastrointestinal Surgery at the All India Institute of Medical Sciences, New Delhi complaining of intermittent fever of two-month duration. There was no history of abdominal pain, jaundice, anorexia or weight loss. Physical examination revealed an ill-defined epigastric lump. The patient was evaluated with an ultrasound and CT scan of the abdomen which revealed a cystic lesion in the region of the pancreas with a bit of calcification (Image 1). There were no other sites of pancreatic calcification either intraductal or parenchymal, and, in addition, there was no ductal dilatation or parenchymal atrophy. On imaging no other cysts could be identified in the abdomen. Hydatid serology of the patient by ELISA was positive. A provisional diagnosis of pancreatic pseudocyst and a differential diagnosis of isolated hydatid cyst of the pancreas were made and the patient underwent surgery. On laparotomy, a bulge (due to the cyst) was seen in the root of the transverse mesocolon (Image 2). The cyst was decompressed by aspiration to decrease the intracystic pressure (Image 3). The lesser sac was opened by dividing the gastrocolic ligament, and the cyst contents (hydatid membranes) were evacuated (Image 4). The deep residual cavity in the region of the neck and proximal body of the pancreas could have been a source of subsequent pancreatic leak/fistula; therefore, it was drained into a Roux loop of the jejunum (Image 5). The patient had an uneventful postoperative course. He was started on albendazole postoperatively for a period of six weeks. At the last follow-up (at one year), the patient was symptom-free and without any evidence of recurrence.



Source of funding for research and publication
None
Conflict of interest
None

