Marialuigia Spinelli*, Di Meglio Lavinia, Luigi Raio, Francesco Di Fabrizio, De Ville De Goyet Jean and Daniel Surbek
Department of Clinical Research, Prenatal Medicine, University of Bern, Switzerland
*Corresponding Author:
Marialuigia Spinelli
Department of Clinical Research, Prenatal Medicine, University of Bern, Switzerland
Tel: +41(0)316318111
E-mail: marialuigiaspinelli@live.it
Received date: April 02, 2016; Accepted date: May 24, 2016; Published date: May 26, 2016
Citation: Spinelli M, Lavinia DM, Raio L, et al. Two-Dimensional Ultrasonographic Prenatal Diagnosis of Choledochal Cyst: Our Experience and Literature Review, Gynecol Obstet Case Rep. 2016, 2:2.
Keywords
Ultrasonographic; Prenatal diagnosis; Choledochal cyst; Trimester
Introduction
Choledochal cysts (CC) are defined as a “pseudo-cystic dilatation” of the extra- or intrahepatic biliary tree or both [1]. The Todani classification lists 5 types of CC: type 1, a pseudocystic dilatation of the extrahepatic bile duct (type 1A: fusiform, sac-like dilatation of the common bile duct; type 1-B: a diverticular dilatation of the common bile duct); type 2, a true cyst of the bile duct (lateral); type 3, a dilatation of the distal, intramural portion of the common bile duct (choledochocele); type 4, dilatation of both the extrahepatic and intrahepatic bile ducts; type 5, saccular dilatation(s) of the intrahepatic bile ducts. The overall incidence is very low with approximately one-third of reported cases been reported in Japanese population [2]. CC type 1 is the most commonly clinical presentation (70-90%), and results in most cases from a malformation of the common junction between the bile duct and the pancreatic duct (at the level of the duodenal wall where they join to form a (usually very short) common channel) [1].
Because of the advance and widespread use of ultrasonography (US), CC is nowadays diagnosed frequently in infancy or early childhood before symptoms appear, and even can be recognized in the antenatal period with maternal US. Prenatal detection of CC is crucial since the newborn can be scheduled to a pre-emptive surgical treatment, and avoiding the occurrence of complications [3]. Nevertheless, diagnosis of CC at prenatal ultrasound is still challenging.
Our Experience
A 32-yr-old, gravida 2, para 1 woman was referred to our obstetric ultrasound facility at 22 weeks of gestation due to a suspected fetal anechoic mass at the level of the abdomen. The previous course of pregnancy had been uneventful. Maternal medical and family histories were unremarkable. US examination was performed through standard Aloka (Aloka Co., Ltd, Tokyo, Japan) equipped with a curved linear array trans-abdominal transducer (2-5 MHz) as well as with a transvaginal 4-8 MHz probe.
Detailed US imaging revealed a single fetus, of a size corresponding to 22 weeks of gestation, which was consistent with her estimated date of delivery. The only abnormality seen on ultrasound scan was a 15 × 16 mm anechoic cyst in the right upper quadrant abdomen (Figure 1).The mass was negative to Color-Doppler and was completely separate from the stomach, bowel, and gall bladder. Kidneys and adrenal glands were normal. A continuity between the gallbladder, the cyst and the dilated lower portion of the choledocus was clearly demonstrated (Figure 1).The latter observations confirmed with no doubt the diagnosis of a CC type I.
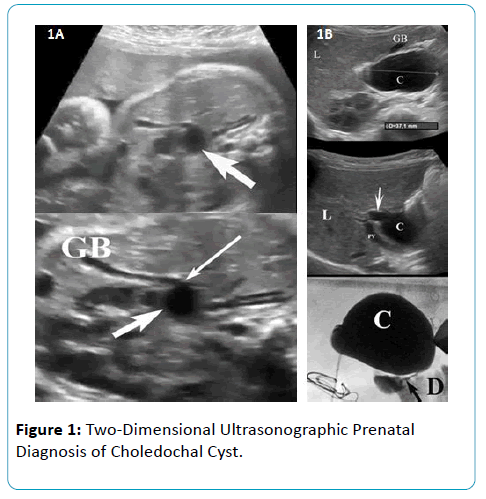
Figure 1: Two-Dimensional Ultrasonographic Prenatal Diagnosis of Choledochal Cyst.
Serial US examinations every 2 weeks showed only a slight increase through gestation, measuring 16 × 19 cm at 35 weeks of gestation; at no moment was noticed a dilatation of the intrahepatic biliary system. At 38 weeks of gestation, a 3450 g female infant was delivered vaginally after spontaneous labour, with an Apgar score of 8 and 10 at 1 and 5 minutes, respectively.
Postnatal US examination confirmed the diagnosis of type I CC: the diameter of the cyst was unchanged compared to the antenatal scan, and the intrahepatic bile ducts were not dilated; also the levels of direct bilirubin, alkaline phosphatase and gamma-glutamyl-transferase were normal. For these reasons, it was proposed to observe and postpone surgery.
Serial postnatal US were performed. At 5,5 months of age, the size of the cyst was 37 × 29 mm, with no sign of any complication. At 10,5 months of age and 8.300 Kgs of weight, surgerywas electively performed (Figure 1). The extrahepatic biliary system (gallbladder, cyst and choledocus) was completely resected and a Roux-en-Y hepaticojejunostomy was performed successfully. The histopathological examination confirmed the diagnosis of CC.
Discussion
The incidental US finding of an intra-abdominal cystic lesion opens the question of its nature, and the necessity of running a differential diagnosis, with regard to both the precise nature of the cist and the organ of origin. Indeed, abdominal cystic anomalies originating from mesentery, omentum, pancreas, bile ducts, liver and ovary, and even associated to intestinal pathologies, have been reported in the literature.
Prenatal diagnosis of CCat US is rare: although this anomaly can present in any age group, most of them are diagnosed in infants and children and rarely in the fetus. In the present paper, a type I CC was diagnosed at 22-week prenatal US as based on the findings of an abdominal mass, negative to Color- Doppler, completely separated from the other intra-abdominal organs and in continuation with the gallbladder and the dilated choledochal duct.The latter observation (of a communication between the various structures) is original in that it never has been described previously in literature to our knowledge; previous reports of prenatal US diagnoses mentioneda simple, cystic mass in the upper abdomen or right upper quadrant,separated by the others intra-abdominal organs [3-7]. The US visualization of this communication between structures may be a simple, but valuable sign for addressing the correct diagnosis.
The average gestational age at time of diagnosis is 26.9 weeks, with the earliest diagnosis reported at 15 weeks (range 15 to 37 weeks) (Table 1) [4-9]. In a series of Redkar [6] the median gestational age at antenatal detection was 20 weeks. Benhidjeb [4] suggest that it is possible to make a presumptive prenatal diagnosis of CC as early as 15 weeks.
| |
Ultrasonograhic Prenatal Diagnosis |
GA (wk) at Diagnosis |
GA (wk) at Delivery |
Age (wk) at Surgery |
Size (mm) at Diagnosis |
| Benhidjeb[3] |
Choledochal cyst |
29 |
40 |
16 |
NA |
| Lugo-Vicente [4] |
Choledochal cyst |
37 |
40 |
16 |
30 |
| Redkar [5] |
Choledochal cyst/Intraabdominal cyst/Duodenal atresia (8 cases) |
16-26 |
NA |
Jan-28 |
13-35 |
| Schroeder [6] |
Choledochal cyst |
15 |
42 |
5 |
20 |
| Tongprasert [7] |
Choledochal cyst |
29 |
36 |
8 |
19 |
| Hernández Herrea [8] |
Intra-abdominal cyst |
N.A. |
39 |
8 |
50 |
| Cong [9] |
Intra-abdominal cyst/Biliary cistic malformation (16 cases) |
19-38 |
22-NA |
04-Dec |
NA |
| Our case |
Choledochal cyst |
22 |
38 |
32 |
37 |
Table 1: The earliest diagnosis reported at 15 weeks.
The differential diagnosis includes duodenal atresia, biliary atresia, enteric duplication cyst, liver cyst, pancreatic cysts, gallbladder duplication, as well as ovarian cyst in female fetuses.
Although magnetic resonance imaging (MRI) or threedimensional (3D) US with reconstructed planes may aid the prenatal diagnosis, we believe that a careful and precise twodimensional (2D) US should be encouraged, since it may be satisfactory enough, in most cases, to demonstrate the sign of the connection between the gall bladder and the cyst, like in our case [10-15]. Indeed, MRI as well as 3D technology, although can be very useful in many cases, especially those of unfavourable fetal position, are expensive tools, require expert operators and are not readily available in some clinical contexts.
Biliary atresia presenting prenatally with a sub-hepatic cyst, although very rare, merits a special attention as this would trigger early surgery on the contrary of the strategy proposed with most other diagnosis: the US changes of the liver parenchyma, and the rising direct bilirubin in presence of acholic stool rapidly after at birth help for a rapid positive diagnosis of biliary atresia.
CC, when undiagnosed, would typically grow in size progressively with age until clinical symptoms or complications develop: the classic triad consist of jaundice (69%), abdominal mass and abdominal pain (caused by complications as cholangitis, bile obstruction or pancreatitis). In rare cases with a much prolonged course, chronic biliary obstruction is associated with prolonged icterus; evolution towards a secondary biliary cirrhosis and portal hypertension has been reported in rare cases. On the contrary, an incidental diagnosis done early in infancy (or a prenatal diagnosis as in our case) before clinical symptoms appear, is much likely to be associated with the absence of any complication and in particular biliary obstruction or pancreatitis [16,17]. As in our case, asymptomatic anicteric infants should be scheduled for elective surgery even in absence of complications, as evolution towards complication is the rule. In neonates with no complications and in absence of signs of hepatic suffering (dilatation of the bile ducts at US, elevation of Gamnmaglutamyl- transferase, slight elevation of direct bilirubin) the best strategy may consists in waiting a few months and postponing surgery to when the child is 8-10 Kgs of weight: this strategy allow to do surgery in best conditions, from an anatomical, technical and anesthesiological point of view.
In cases presenting complications, surgery should be preceded by adequate management of the complication (drainage of biliary system, endoscopic shincterotomy, medical treatment of pancreatitis) [5,17].
The recommended treatment of CC is total resection of the cyst and of the extrahepatic bile ducts; resection of the cyst is important as malignant transformation of the biliary epithelium of cysts left in place has been described in young adults operated during childhood [17]. The biliary drainage is then restored by a Roux-en-Y hepaticojejunostomy reconstruction; long-term outcome of such operations is good, except for few patients presenting later in age with biliary obstruction and/or lithiasis caused by anastomotic stricture, which respond well to conventional management (radiological or surgical or both) [18]. For that reason, these patients needs a long-term follow-up consisting of US Doppler and liver tests at regular interval (annually or bi-annually).
Conclusion
Prenatal ultrasound of choledochal cyst by 2D-US is challenging but it is important for the proper prenatalpostnatal managment of the case. Currently, the improved and shared experience of operators, with an increasing number of cases reported in the literature, may be helpful for addressing such an issue.
References
- Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K (1997) Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg 134: 263-269.
- Savader SJ, Benenati JF, Venbrux AC, Mitchell SE, Widlus DM, et al. (1991) Choledochal cysts: classification and cholangiographic appearance. AJR Am J Roentgenol 156: 327-331.
- Foo DC, Wong KK, Lan LC, Tam PK (2009) Impact of prenatal diagnosis on choledochal cysts and the benefits of early excision. J Paediatr Child Health 45: 28-30.
- Benhidjeb T, Chaoui R, Kalache K, Mau H, Müller JM (1996) Prenatal diagnosis of a choledochal cyst: a case report and review of the literature. Am J Perinatol 13: 207-210.
- Lugo-Vicente HL (1995) Prenatally diagnosed choledochal cysts: observation or early surgery? J Pediatr Surg 30: 1288-1290.
- Redkar R, Davenport M, Howard ER (1998) Antenatal diagnosis of congenital anomalies of the biliary tract. J Pediatr Surg 33: 700-704.
- Schroeder D, Smith L, Prain HC (1989) Antenatal diagnosis of choledochal cyst at 15 weeksâ€Âââ€Å¾Â¢ gestation: etiologic implications and management. J PediatrSurg 24: 936-938.
- Tongprasert F, Traisrisilp K, Tongsong T (2012) Prenatal diagnosis of choledochal cyst: a case report. J Clin Ultrasound 40: 48-50.
- Hernández Herrera RJ, Flores Santos R, Hinojosa Salinas A, Ramos González R, RamÃÂÂÂrez González B (2013) (Prenatal diagnosis of choledochal cyst). Ginecol Obstet Mex 81: 115-119.
- Howell CG, Templeton JM, Weiner S, Glassman M, Betts JM, et al. (1983) Antenatal diagnosis and early surgery for choledochal cyst. J Pediatr Surg 18: 387-393.
- Chen CP, Cheng SJ, Chang TY, Yeh LY, Lin YH, et al. (2003) Prenatal diagnosis of choledochal cyst using ultrasound and magnetic resonance imaging. Ultrasound ObstetGynecol 23: 93-94.
- Chen CP, Cheng SJ, Sheu JC, Lin YH (2004) Third-trimester evaluation of choledochal cyst using magnetic resonance imaging. Prenat Diagn 24: 838-839.
- Nori M, Venkateshwarlu J, Vijaysekhar, Prasad GR (2013) Extrahepatic biliary atresia with choledochal cyst: Prenatal MRI predicted and post natally confirmed: A case report.Indian J Radiol Imaging 23: 238-42.
- Lee IH, Kim GJ (2008) Fetal choledochal cyst diagnosed at 22 weeks of gestation by three-dimensional ultrasonography: a case report. J Korean Med Sci 23: 909-911.
- Matsubara H, Oya N, Suzuki Y, Kajiura S, Suzumori K, et al. (1997) Is it possible to differentiate between choledochal cyst and congenital biliary atresia (type I cyst) by antenatal ultrasonography? FetalDiagnTher 12: 306-308.
- Stringer MD, Dhawan A, Davenport M, Mieli-Vergani G, Mowat AP, et al. (1995) Choledochal cysts: lessons from a 20 year experience. Arch Dis Child 73: 528-531.
- Cong X, Sun X, Liu S (2015) Evaluation and screening ultrasonic signs in the diagnosis of fetal biliary cystic malformation.JMaternFetal Neonatal Med 28: 2100-2105.
- Okada T, Sasaki F, Ueki S, Hirokata G, Okuyama K, et al. (2004) Postnatal management for prenatally diagnosed choledochal cysts. J Pediatr Surg 39: 1055-1058.

