Keywords
Acute Pancreatitis; Adverse effect; Vildagliptin, Dipeptidylpeptidase
4 inhibitors
Abbreviations
AP Acute Pancreatitis; IBT incretin-based therapies
INTRODUCTION
Dipeptidyl-peptidase 4 inhibitors (DPP-4i) are wellestablished
and widely popular incretin-based agents.
Their popularity is owed mainly to their tolerability and
low risk of hypoglycemia [1, 2]. The risk of pancreatic
complications of DPP-4i as well as glucagon-like peptide
analogs (GLP-1a), has not reached an agreement since
some observational studies and meta-analysis underlies
the risk might be evident [3, 4]; however, opposing views
regarding pancreatic events have been supported by some
other trials [5, 6, 7]. Incretin-based therapies (IBT) has
been issued alerts against the potential pancreatic adverse
effects by the US Food and Drug Administration, following
post-marketing reports of pancreatic complications [8].
A non-interventional safety study showed that there is
no increased pancreatitis risk with vildagliptin use [9]. It
can be assumed that vildagliptin associated pancreatitis
is an infrequent entity or can be due to drug class-effect.
Reported cases shall be inspected with their individualistic
characteristics. Hereby we present two probable associated
cases.
Case 1#: A 31-year-old diabetic woman (BMI 27.65)
presented with severe abdominal pain radiating back,
and vomiting was diagnosed as acute pancreatitis (AP) in December 2018. Her last diabetic therapy consisted of
insulin plus oral antidiabetics, including vildagliptin. The
distinguishing point from other reports, in this case, was
a history of diabetic ketoacidosis induced by acute biliary
pancreatitis eight months ago. The previous episode
was treated by papillotomy by ERCP, and the source was
eliminated by cholecystectomy. During this period, oral
hypoglycemic drugs were discontinued, and her diabetic
regimen was switched to insulin detemir and insulin aspart
for bolus before meals. Since keto-acidosis was noted at
the first presentation, autoantibodies were checked and
found negative, with a quantified serum C-peptide. After
complete resolution of pancreatitis, metformin 1000
milligram BID was re-started with basal-bolus insulin
treatment. Vildagliptin was added-on the metformin as
a combined preparation (Galvus-met ® 50mg /1000mg),
with a detailed explanation and discussion of risks and
benefits of the DPP-4i with the patient. She started to
experience mild hypoglycemic attacks with even low doses
of insulin aspart. Therefore, bolus insulin injections were
discontinued, and basal insulin detemir was titrated to
a lower dose. HbA1c was dropped to 6.8, with a lifestyle
modification and reduction of insulin dosage, and weight
control was achieved more easily.
She described her pain radiating toward bilaterally
flank areas and also emphasized the similarity with the
first pancreatitis episode. Her initial laboratory studies
revealed: normal blood glucose: 134 mg/dL (74-106),
elevated CRP 100.01 mg/L (<5), increased level serum
amylase of 1 814 mg/dL (30-118). Renal function tests
and liver biomarkers were unremarkable (presented in Table 1). Abdominal computed tomography revealed
an irregularly enlarged pancreatic head with increased
infiltration around the pancreas along mesentery,
consistent with a diagnosis of acute interstitial pancreatitis (Figure 1a). Besides cholecystectomy clips, there was no
evidence of biliary tree abnormalities. Ultrasonography
also confirmed the intrahepatic and extrahepatic biliary
tree were completely normal in size. Her BISAP score
was 1. The patient was, therefore, admitted to the general
medicine ward. There was no history of illicit drugs,
alcohol, or antibiotics. Her drug history had consisted of
vildagliptin-metformin combination (50/1000mg twice
daily), insulin detemir (16 units s.c daily), and ibuprofen
400mg for headache (when needed-latest pill was taken
six days ago). All oral medications were discontinued,
crystalloid fluid resuscitation and petidin for paincontrol
were ordered. With a conservative approach, the
patient’s symptoms were resolved entirely by the third
in-hospital day, and she was discharged with a basal-bolus
insulin regimen. Vildagliptin was suspected as a possible
cause of the recurrence, so only metformin added on the
control visit, two weeks after discharge. There has been no
recurrence of acute pancreatitis for 23 months.
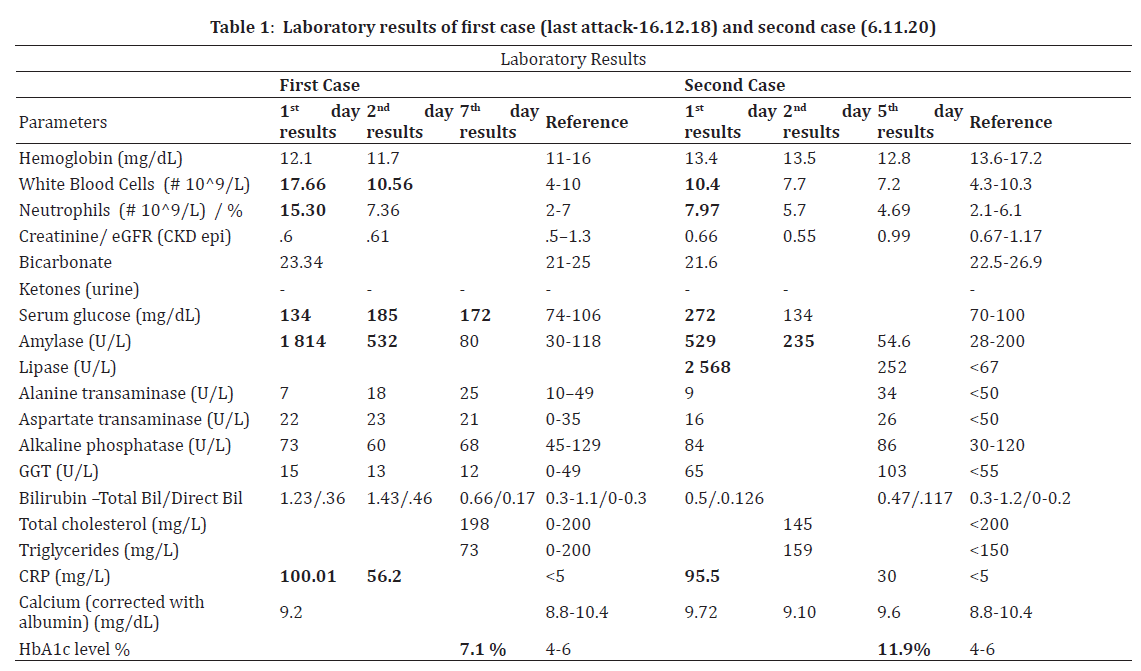
Figure 1. (a). First case: Computed Tomography at the present attack considered as drug-induced pancreatitis at December 2018; Acute interstitial pancreatitis with irregularly oedematous body. (b). Second case: Contrast enhanced CT scan at the present attack at November 2020; consistent with edema and inflammation in the surrounding adipose tissue. Arrow indicates linear edema and increased density extending to the left perirenal area in the tail part of the pancreas.
Case #2: A 41-year-old Caucasian male (BMI 28.89) with
a history of uncontrolled type II diabetes, presented to the
emergency department with an abrupt onset of epigastric
pain radiating back after a meal in November 2020. His
previous history was remarkable with atherosclerotic
heart disease, quintuple bypass surgery, and ICD
implantation due to ventricular arrhythmia two years ago.
He was on regular treatment with metformin-vildagliptin
(50/1000) BID and low-dose salicylates for two years. He
does not follow any dietitian recommendation and drinks
alcohol once or twice a month, but he admits he can rarely
binge a large number of spirits. Fourteen days prior to his
symptoms, he had five units of drink. He has no history of
gall-stone disease or pancreatitis.
On examination, he was in pain, sweaty, and pale, with a
pulse rate of 105 per minute. There was tenderness in the
peri-umbilical and right upper quadrant region, without
guarding. Other physical signs were not remarkable. His
initial workup revealed: serum glucose 272 mg/dl (70-
100), amylase 520 U/L (28-200); lipase 2 568 U/L (<67),
CRP 95.5 mg/L (<5), transaminases, gamma-glutamyl
transferase, alkaline phosphatase, bilirubin profile, renal
function tests, and blood gases were normal (Table 2). No
ketone was found in urinalysis. Corrected calcium was 9.72
mg/dl at admission, serum triglyceride level was checked
a day after and recorded as 159 mg/dl (<150).
Computerized tomography of the abdomen showed
increased density in the pancreatic head, trunk, and
tail, consistent with edema and inflammation in the
surrounding adipose tissue (Figure 1b). Necrosis was
not visualized. There were linear edema and increased
density extending to the left perirenal area in the tail
part of the pancreas. His BISAP score was 0. He was
admitted to the general medicine ward and treated with
IV crystalloids and pain-killers. Vildagliptin and metformin
were discontinued, and basal-bolus insulin treatment was
started. HbA1c was checked on the fourth day of admission
and 11.9. On the fifth day of admission serum amylase was
returned to normal, and he was free of pain. After dietary
and lifestyle recommendations, he was discharged with
pre-meal insulin aspart (3 x 10 units) and basal insulin
glargine (22 units).
DISCUSSION
The possibility of pancreatitis in patients treated with
IBT should be taken into consideration during the course of treatment. Though the up-to-date data still does not signify
the actual root-cause effect of IBT and acute pancreatitis,
post-marketing reports have yet been published, since
while. Published data reporting vildagliptin-associated
pancreatitis are relatively few; the first case was reported
from Sydney, Australia, being followed by two cases
from India [10-12]. Three suspected cases were reported
through the evolution of DPP-4i induced acute pancreatitis
by reviewing reports from the Taiwanese database
[13]. The latest cases were two patients from Turkey,
in whom imaging studies were consistent with acute
pancreatitis without enzyme elevation [14]. We report
two acute pancreatitis cases confirmed by radiological and
laboratory workup, which we thought vildagliptin might
have triggered. However, we should still be cautious by
using the term –induced, since the induction of an acute
attack may not be due to one major factor in those cases,
since identifying drug-induced pancreatitis in patients
with type 2 diabetes mellitus can be highly challenging
due to several coexisting factors. First of all, patients with
diabetes have a 1.5-3-fold increase in the risk of acute
pancreatitis [15-17]. Additionally, among people with
diabetes, the incidence of gall-stone formation increases
[18]. Abnormal lipid profile, which is not rare in diabetics, can induce pancreatitis directly or cholesterol crystal
formation in the gallbladder [19]. Patients with a history of
gallstone pancreatitis are particularly at risk of recurrence
[20]. Though cholecystectomy effectively reduces the risk
of recurrence [21]. After cholecystectomy, pancreatitis
may still recur due to unrecognized bile duct microlithiasis
or hypertonic sphincter of Oddi [22, 23]. However,
papillotomy will enable biliary flow and treat the sphincter
hypertonicity.
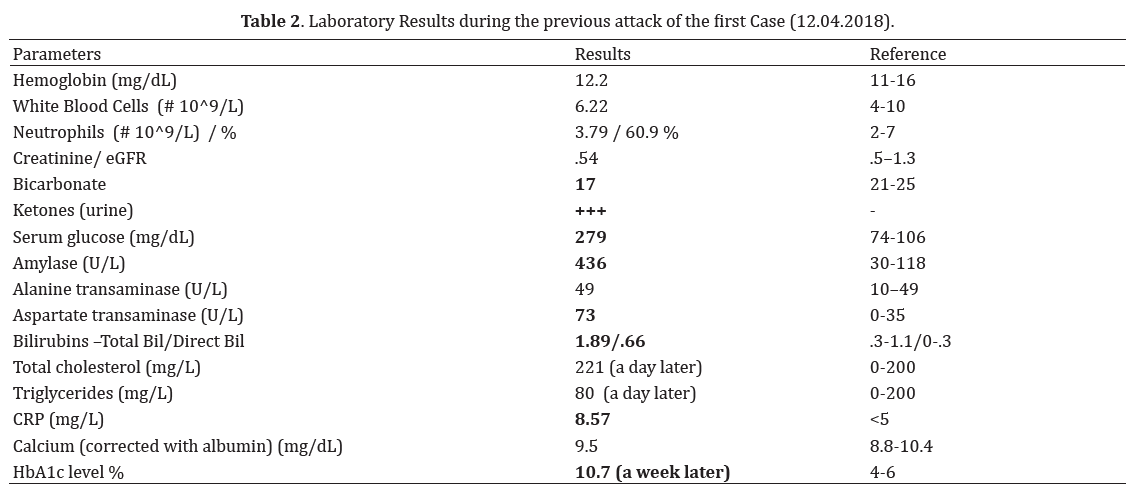
Back to our first attack of the first case, the biliary tree
was fairly normal, and the head of the pancreas was mildly
oedematous, but no fluid was seen around pancreatic
tissue, and no enflamed retroperitoneum or mesentery was
noted. Numerous stones were identified in the gallbladder
(Figure 2a, b). So the first attack might have been an early
period of obstruction of pancreatic ductus as we thought or
a non-biliary attack with a co-incidental gall-stone disease.
We admitted the case as a biliary, treated her accordingly.
Nevertheless, sphincterotomy and cholecystectomy
were supposed to eliminate the biliary risk. Metabolic
abnormalities are expected in diabetics, and the serum
level of triglycerides does not have to be higher than 1
000 as opposed to the common knowledge [19]. In our
case, it is also unlikely since triglycerides level were fairly
normal (Table 1). The history of alcohol consumption
was evident in our second case; however, social drinking
is very prevalent. The threshold levels of alcohol amount
or drinking frequencies associated with an increased risk
of alcohol-related pancreatitis have not been defined yet.
However; acute and chronic pancreatitis are common in
chronic abusers [24]; drinking a large amount may trigger
the acute attack [25]. The patient occasionally drinks and
may rarely have more than three or four units of alcohol
once a while. He denies dipsomaniac behavior, and has no
stones in gallbladder.
Figure 2. CT scan of the abdomen at the first attack of the first case, considered as biliary pancreatitis. (a). Mildly enflamed pancreatic head. (b). Gall-stones visible in gall-bladder.
The rather brave approach we took and its
consequences showed us the complex and multifactorial
nature of the disease. With the lack of knowledge about
how an attack may predispose another, we can skip some
mechanisms that might still ensue. Unfortunately, causal
oversimplification makes us ignore conjoint possibilities
as defined in a type of false dilemma, the fallacy of the single
cause. Even after complete resolution of the inflammatory
response, the pancreas may keep a vulnerability for
another attack by a wide variety of causes for a while. This
susceptible condition might be due to an improper flow of
enzymes from a mal-repaired ductal tissue, tortoise lumen,
or microarchitecture change. Even without a history of
AP, toxic substances such as ethanol may cause microinjuries,
prematurely activates proteolysis, and deplete
anti-oxidative protective factors [26].
CONCLUSION
A consensus for impeding the generalized use of DPP-4i
has not been clearly established. There seems to be a lack of
a strategy to identify and stratify the patients at increased
risk for developing DPP-4i–related pancreatitis. In general, practitioners tend to think to avoid IBT in patients with
risk factors for pancreatitis or a history of pancreatitis,
whatever the reason was before. These conservative
approaches should be appreciated, even though it does not
specify or stratify the risk groups according to subtypes of
pancreatitis. Objective identification of subjects with risk
factors for pancreatitis or recurrence who have a history
of acute pancreatitis still needs robust assessments to
determine the extent of the risk of each molecule.
Conflict of Interest
The authors state that they have no Conflict of Interest.
References
- Scheen AJ. Safety of dipeptidyl peptidase-4 inhibitors for treating type 2 diabetes. Expert Opin Drug Saf 2015; 14(4):505-24. [PMID: 25630605]
- Schwartz SL. Treatment of elderly patients with type 2 diabetes mellitus: a systematic review of the benefits and risks of dipeptidyl peptidase-4 inhibitors. Am J Geriatr Pharmacother 2010; 8(5):405-18. [PMID: 21335294]
- Knapen LM, de Jong RG, Driessen JH, Keulemans YC, van Erp NP, De Bruin ML, et al. Use of incretin agents and risk of acute and chronic pancreatitis: A population-based cohort study. Diabetes Obes Metab 2017; 19(3):401-411. [PMID: 27883260]
- Pinto LC, Rados DV, Barkan SS, Leitão CB, Gross JL. Dipeptidyl peptidase-4 inhibitors, pancreatic cancer and acute pancreatitis: A meta-analysis with trial sequential analysis. Sci Rep 2018; 8(1):782. [PMID: 29335646; PMCID: PMC5768864]
- Ahrén B. Clinical results of treating type 2 diabetic patients with sitagliptin, vildagliptin or saxagliptin--diabetes control and potential adverse events. Best Pract Res Clin Endocrinol Metab 2009; 23:487-98. [PMID: 19748066]
- Buse JB, Bethel MA, Green JB, Stevens SR, Lokhnygina Y, Aschner P, et al. Pancreatic Safety of Sitagliptin in the TECOS Study. Diabetes Care 2017; 40(2):164-170. [PMID: 27630212; PMCID: PMC5864139]
- Garg R, Chen W, Pendergrass M. Acute pancreatitis in type 2 diabetes treated with exenatide or sitagliptin: a retrospective observational pharmacy claims analysis. Diabetes Care 2010; 33(11):2349-54. [PMID: 20682680; PMCID: PMC2963493]
- The U.S. Food and Drug Administration: FDA Drug Safety Communication. 2013; Available from: FDA Drug Safety Communication: FDA investigating reports of possible increased risk of pancreatitis and pre-cancerous findings of the pancreas from incretin mimetic drugs for type 2 diabetes.
- Williams R, Kothny W, Serban C, Lopez-Leon S, Schlienger R. Pancreatic safety of vildagliptin in patients with type 2 diabetes mellitus: A European, noninterventional, postauthorization safety study. Endocrinol Diabetes Metab 2019; 2(2):e00052. [PMID: 31008361; PMCID: PMC6458459]
- Girgis CM, Champion BL. Vildagliptin-induced acute pancreatitis. Endocr Pract 2011; 17(3):e48-50. [PMID: 21324812]
- Kunjathaya P, Ramaswami PK, Krishnamurthy AN, Bhat N. Acute necrotizing pancreatitis associated with vildagliptin. JOP 2013; 14(1):81-4. [PMID: 23306341]
- Saraogi R, Mallik R, Ghosh S. Mild acute pancreatitis with vildagliptin use. Indian J Endocrinol Metab 2012; 16(Suppl 2):S480-2. [PMID: 23565473; PMCID: PMC3603121]
- Yang TL, Shen MC, Yu ML, Huang YB, Chen CY. Acute pancreatitis in patients with type 2 diabetes mellitus treated with dipeptidyl peptidase-4 inhibitors. J Food Drug Anal 2016; 24(2):450-454. [PMID: 28911601]
- Mungan Z, Attila T, Ünal Kabaoğlu Z, Vural M. Vildagliptin-induced acute pancreatitis without enzyme elevation. Turk J Gastroenterol 2017; 28(6):514-517. [PMID: 29086719]
- Girman CJ, Kou TD, Cai B, Alexander CM, O'Neill EA, Williams-Herman DE, Katz L. Patients with type 2 diabetes mellitus have higher risk for acute pancreatitis compared with those without diabetes. Diabetes Obes Metab. 2010; 12(9):766-71. [PMID: 20649628]
- Lai SW, Muo CH, Liao KF, Sung FC, Chen PC. Risk of acute pancreatitis in type 2 diabetes and risk reduction on anti-diabetic drugs: a population-based cohort study in Taiwan. Am J Gastroenterol 2011; 106(9):1697-704. [PMID: 21577242]
- Noel RA, Braun DK, Patterson RE, Bloomgren GL. Increased risk of acute pancreatitis and biliary disease observed in patients with type 2 diabetes: a retrospective cohort study. Diabetes Care 2009; 32:834-8. [PMID: 19208917; PMCID: PMC2671118]
- Chen CH, Lin CL, Hsu CY, Kao CH. Association Between Type I and II Diabetes With Gallbladder Stone Disease. Front Endocrinol (Lausanne) 2018; 9:720. [PMID: 30555418; PMCID: PMC6281708]
- Lindkvist B, Appelros S, Regnér S, Manjer J. A prospective cohort study on risk of acute pancreatitis related to serum triglycerides, cholesterol and fasting glucose. Pancreatology 2012; 12(4):317-24. [PMID: 22898632]
- Hazem ZM. Acute biliary pancreatitis: diagnosis and treatment. Saudi J Gastroenterol 2009; 15(3):147-55. [PMID: 19636174; PMCID: PMC2841412]
- Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013; 144:1252-61. [PMID: 23622135; PMCID: PMC3662544]
- Chen JW, Thomas A, Woods CM, Schloithe AC, Toouli J, Saccone GT. Sphincter of Oddi dysfunction produces acute pancreatitis in the possum. Gut 2000t; 47(4):539-45. [PMID: 10986215; PMCID: PMC1728061]
- Elta GH. Sphincter of Oddi dysfunction and bile duct microlithiasis in acute idiopathic pancreatitis. World J Gastroenterol 2008; 14(7):1023-6. [PMID: 18286682; PMCID: PMC2689403]
- Gullo L, Migliori M, Oláh A, Farkas G, Levy P, Arvanitakis C, et al. Acute pancreatitis in five European countries: etiology and mortality. Pancreas 2002; 24(3):223-7. [PMID: 11893928]
- Deng L, Xue P, Huang L, Yang X, Wan M, Xia Q. Binge drinking aggravates the outcomes of first-attack severe acute pancreatitis. Pancreas 2010; 39(2):149-52. [PMID: 19820420]
- Kristiansen L, Grønbaek M, Becker U, Tolstrup JS. Risk of pancreatitis according to alcohol drinking habits: a population-based cohort study. Am J Epidemiol 2008; 168(8):932-7. [PMID: 18779386]



