Keywords
CA-19-9 Antigen; Pancreatic Neoplasms; Prognosis
What Did We Know Before the American Society of Clinical Oncology (ASCO) Annual Meeting?
The American Cancer Society’s publication cancer facts and figures has chosen to dedicate a special section to pancreatic cancer this year due to the lack of progress in primary prevention and screening of this deadly disease. They estimate that in 2013 about 45,220 new cases will be diagnosed in the US and about 38,460 patients will die of this cancer. In the US only 15-20% patients are diagnosed early enough to be eligible for surgery the rest are diagnosed with advanced disease. If diagnosed at the earliest stage they have a median survival of 24.1 months and at the most advanced stage a median survival of 4.5 months [1]. Presently high risk individuals are screened with endoscopic ultrasound, magnetic resonance imaging, endoscopic retrograde cholangiopancreatography or helical computerized tomography [2]. Multiple tumor markers have been described for detecting pancreatic cancer. They are CEA, carcinoembryonic antigen-related cell adhesion molecule-1 (CEACAM- 1), CA 19-9, SPan-1, DUPAN-2, macrophage inhibitory cytokine 1 (MIC-1), alpha4GnT, PAM4, pancreatic juice DNA methylation, and fecal K-ras; however none of them has proved superior enough to be used as a widespread screening test [3]. Research in the field of tumor markers has been constantly evolving and as yet a breakthrough test that can be used to screen high risk patients is to be discovered. However, there has been much progress in using tumor markers as predictors of prognosis and to guide further management.
In this paper, we will focus on carbohydrate antigen 19-9 (CA 19-9) which has been researched and used most extensively as a tumor marker in pancreatic cancer. CA 19-9 was first isolated in 1979 [4] and is a sialylated Lewis blood group antigen (Le)a [5]. As a screening test CA 19-9 has a sensitivity of about 79-81% and a specificity of about 82-90%. However, it has a positive predictive value of only 0.5-0.9% which renders it not useful as a screening test. False positives are seen in multiple conditions most often obstructive jaundice as CA 19-9 is partly excreted through bile. Pancreatic diseases such as acute and chronic pancreatitis, abscesses, pseudocysts can also have elevated CA 19-9 levels and hence it is sometimes difficult to differentiate benign versus malignant pancreatic etiologies. Hepatobiliary diseases such as infection, inflammation, cysts and malignancy, gastrointestinal malignancies such as colorectal, esophageal and gastric cancer, as well as other conditions such as bronchitis, congestive heart failure, cystic fibrosis, diverticulitis, Hashimoto’s thyroiditis, lung cancer, ovarian cyst, pleural effusion, renal cyst and rheumatoid arthritis can all cause false positive elevations [6]. False negative values are seen in patients with genetic absence of the sialylated Lewis blood group antigen Lea-b- as they will hence have undetectable levels of CA 19-9 [5]. However it has been used as a predictor of prognosis, overall survival, predicting response to surgery and chemotherapy.
Preoperative CA 19-9 levels correlate with cancer stage and hence can indirectly be used as a marker for tumor resectability. A recent study showed that preoperative CA 19-9 levels equal to, or greater than, 100 U/mL predicted early recurrence and these patients did not derive significant benefit from surgical resection. The 1-, 3- and 5-year disease free survival rates in patients with CA 19-9 less than 100 U/mL were 67.9%, 41.5% and 41.5% whereas in patients with CA 19-9 equal to, or greater than, 100 U/mL they were 27.4%, 6.5% and 6.5%. Median survival was 22 months versus 6 months in these two patient subgroups, respectively [7]. Multiple such studies were done previously and have shown to have similar outcomes; however, this should not be used as the sole criteria for determining resectability and other factors such as imaging and staging laparoscopy should be used. These studies have also shown that preoperative CA 19-9 levels are a predictor of overall survival and prognosis [6]. A recent study done in Korea has contradicting results. They measured pretreatment CA 19-9 levels in 187 patients irrespective of stage and treatment modality to assess utility in determining prognosis and found that the median overall survival of the normal CA 19-9 group (12.4 months) was not significantly different from the elevated CA 19-9 group (13.5 months) [8]. Most other studies that were assessing its utility in determining prognosis included patients with specific stages or treatments.
Measuring CA 19-9 levels prior to therapy with neoadjuvant or adjuvant chemotherapy and demonstrating a treatment related decline in its levels post chemotherapy is associated with prolonged survival and is an independent predictor of overall survival as it has been evidenced in multiple studies that have assessed response to chemotherapy [6]. A recent study showed patients with post resection CA 19-9 levels less than 90 U/mL appeared to benefit from adjuvant chemotherapy and normalization of CA 19-9 levels maybe associated with an excellent outcome. They recommended checking CA 19-9 levels at multiple time points pre-operatively, post-operatively, preadjuvant, during chemotherapy, post adjuvant therapy and as surveillance [9]. Another study that looked at patients receiving palliative chemotherapy found that a CA 19-9 decline of 25% or less during the first two chemotherapy cycles was predictive for time to progression and overall survival. Checking baseline CA 19-9 and CA 19-9 kinetics with advanced pancreatic cancer during first-line chemotherapy have prognostic value [10].
What Have We Learnt from the American Society of Clinical Oncology (ASCO) Annual Meeting?
Early CA 19-9 Progression in Salvage Chemotherapy for Refractory Pancreatic Cancer (Abstract #e15146 [11])
Nakai et al. described the importance of early CA 19-9 progression in salvage chemotherapy for refractory pancreatic cancer [11]. Table 1 reveals the data.

The authors concluded that the early progression of CA 19-9 (prior to second course), in spite of the first course of salvage chemotherapy, is a negative prognostic factor of progression free survival and overall survival in refractory pancreatic cancer and consideration for discontinuation of further salvage chemotherapy should be made as they may not derive additional benefit.
CA 19-9 Decrease at 8 Weeks is a Predictor of Overall Survival in Patients with Metastatic Pancreatic Cancer (Abstract #4058 [12])
Chiorean et al. described that the CA 19-9 decrease at 8 weeks is a predictor of overall survival in a randomized phase III trial of weekly nabpaclitaxel plus gemcitabine versus gemcitabine alone in patients with metastatic pancreatic cancer as shown in Table 2 [12].

The authors concluded that a greater reduction in CA 19-9 post chemotherapy correlates with better overall survival. Patients treated with nabpaclitaxel plus gemcitabine also had a greater percent decrease in CA 19-9 than the patients treated only with gemcitabine.
Decline in Serum CA 19-9 After Neoadjuvant Therapy with Improved Survival Among Borderline Resectable Pancreatic Cancer Patients (Abstract #e15082 [13])
Tsai et al. discussed the association of decline in serum CA 19-9 after neoadjuvant therapy with improved survival among borderline resectable pancreatic cancer patients [13].
Figure 1 describes the sequence of therapeutic interventions undertaken in this study and the subsequent mean CA19-9 levels in these patients.
Figure 1. Sequence of therapeutic interventions and subsequent mean CA19-9 measurements.
The relative change in CA 19-9 was evaluated as:

The results are showed in Table 3.
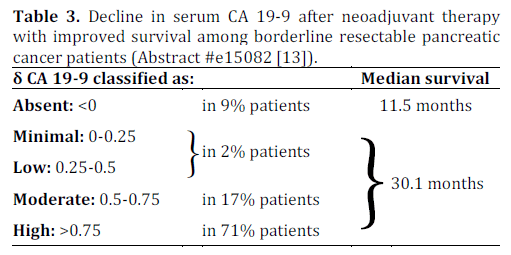
The authors concluded that an increased δ CA 19-9 was associated with increased odds (5.4-fold) of completing all neoadjuvant therapy including surgery as compared with no change and increased overall survival.
Role of Circulating Cytokines and Angiogenic Factors as Markers of Clinical Response in Patients with Untreated Metastatic Adenocarcinoma (Abstract #4042 [14])
Heymach et al. described the role of circulating cytokines and angiogenic factors as markers of clinical response in the study of trametinib plus gemcitabine versus placebo plus gemcitabine for patients with untreated metastatic adenocarcinoma [14].
Thirty cytokines and angiogenic factors were measured at baseline and day 15. Changes from baseline were assessed for association with clinical outcome. The results are summarized in Table 4.
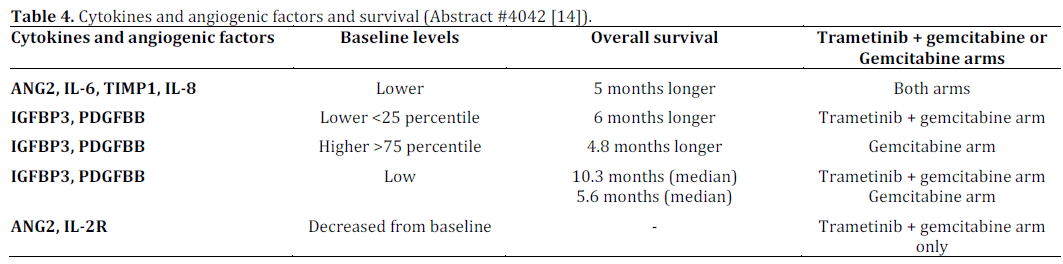
The authors concluded that the plasma cytokines and angiogenic factors profiling may be a useful aid in assessing prognosis, treatment response and pathways modulated by treatment. Patients with low baseline IGFBP3, PDGFBB may receive greater benefit from trametinib plus gemcitabine compared to gemcitabine as seen in overall survival.
Discussion
Current knowledge in the field of pancreatic cancer supported by the multiple studies shows that CA 19-9 levels are a useful adjunct to guide further management and determine prognosis in patients. The recent studies that are being presented at the ASCO meeting take this knowledge one step forward. The study done by Tsai et al. delineates the role of CA 19-9 decline in response to neoadjuvant therapy in patients with localized disease and shows that this is associated with improved survival [13]. Most studies prior to this assessed the role of CA 19-9 levels prior to and after surgery. Patients treated with nab-paclitaxel along with gemcitabine were shown to have improved overall survival compared to gemcitabine alone which correlated with CA 19-9 levels which can be used as a surrogate prognostic marker to assess response to chemotherapy in these patients. Most studies measuring CA 19-9 levels and assessing its levels in response to chemotherapy were done with neoadjuvant or adjuvant chemotherapy. Nakai et al. in Japan assessed CA 19-9 as a prognostic indicator of response to salvage chemotherapy in patients with refractory pancreatic cancer and found a positive correlation with its levels and treatment response which may hence help determine that continuation of further salvage chemotherapy may not derive additional benefit [11].
Conclusion
These abstracts describe additional benefits to checking CA 19-9 levels at important therapeutic decision crossroads in patients. As more data is added to the already known benefits of CA 19-9, its use as a tumor marker will only be strengthened further.
Conflict of interest
The authors have no potential conflicts of interest
References
- Bilimoria, K.Y., et al., Validation of the 6th edition AJCC Pancreatic Cancer Staging System: report from the National Cancer Database. Cancer, 2007. 110(4): p. 738-44.
- American Cancer Society. Cancer Facts & Figures 2013. Atlanta: American Cancer Society; 2013
- Bussom, S. and M.W. Saif, Methods and rationale for the early detection of pancreatic cancer. Highlights from the "2010 ASCO Gastrointestinal Cancers Symposium". Orlando, FL, USA. January 22-24, 2010. JOP : Journal of the pancreas, 2010. 11(2): p. 128- 30.
- Koprowski, H., et al., Colorectal carcinoma antigens detected by hybridoma antibodies. Somatic cell genetics, 1979. 5(6): p. 957-71.
- Tempero, M.A., et al., Relationship of carbohydrate antigen 19-9 and Lewis antigens in pancreatic cancer. Cancer research, 1987. 47(20): p. 5501-3.
- Ballehaninna, U.K. and R.S. Chamberlain, The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. Journal of gastrointestinal oncology, 2012. 3(2): p. 105-19.
- Sugiura, T., et al., Serum CA 19-9 is a significant predictor among preoperative parameters for early recurrence after resection of pancreatic adenocarcinoma. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract, 2012. 16(5): p. 977-85.
- Lee, K.J., et al., Serum CA 19-9 and CEA levels as a prognostic factor in pancreatic adenocarcinoma. Yonsei medical journal, 2013. 54(3): p. 643-9.
- Humphris, J.L., et al., The prognostic and predictive value of serum CA 19.9 in pancreatic cancer. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO, 2012. 23(7): p. 1713-22.
- Haas, M., et al., Prognostic value of CA 19-9, CEA, CRP, LDH and bilirubin levels in locally advanced and metastatic pancreatic cancer: results from a multicenter, pooled analysis of patients receiving palliative chemotherapy. Journal of cancer research and clinical oncology, 2013. 139(4): p. 681-9.
- Nakai, Y., et al., A retrospective analysis of early CA 19-9 progression in salvage chemotherapy for refractory pancreatic cancer. Journal of Clinical Oncology 31, 2013 (suppl; abstr e15146)
- Chiorean, E. G., et al., CA 19-9 decrease at 8 weeks as a predictor of overall survival (OS) in a randomized phase III trial (MPACT) of weekly nab-paclitaxel (nab-P) plus gemcitabine (G) versus G alone in patients with metastatic pancreatic cancer (MPC.) Journal of Clinical Oncology 31, 2013 (suppl; abstr 4058)
- Tsai S., et al, Association of decline in serum CA 19-9 after neoadjuvant therapy with improved survival among borderline resectable pancreatic cancer patients. Journal of Clinical Oncology 31, 2013 (suppl; abstr e15082)
- Heymach J., et al, Circulating cytokines and angiogenic factors (CAF) as markers of clinical response in the study of trametinib (T) plus gemcitabine (G) versus placebo (P) plus gemcitabine for patients (pts) with untreated metastatic adenocarcinoma of the pancreas (MEK113487). Journal of Clinical Oncology 31, 2013 (suppl; abstr 4042)


