Keywords
gemcitabine; irinotecan; Pancreatic Neoplasms; Treatment Failure
Abbreviations
ASCO: American Society of Clinical Oncology; FOLFIRI: irinotecan with 5-FU and folinic acid; FOLFOX: folinic acid plus 5-FU plus oxaliplatin; PEP02: liposome irinotecan
INTRODUCTION
Pancreatic cancer remains the fourth leading cause of cancer-related mortality with an estimated total of 43,100 new cases and 36,800 deaths in 2010 in the USA alone [1]. Overall survival remains poor despite advances in therapeutics. Gemcitabine-based regimens represent the standard systemic first-line treatment in patients with advanced pancreatic cancer, offering a better quality of life as well as a small survival benefit [2]. Only a small percentage of patients who exhibit disease progression after first-line treatment continue to receive second-line therapy, mainly because of poor performance status. Therefore, few randomized trials have been conducted and there is currently no consensus on the standard of care for refractory pancreatic cancer [3].
What Did We Know Prior to the 2011 ASCO GI Cancer Symposium?
Oettle et al. [4] evaluated folinic acid plus 5-FU plus oxaliplatin (FOLFOX) as second-line treatment in advanced pancreatic cancer and they were the first to establish that chemotherapy offers better overall survival to refractory patients as compared to best supportive care (21 vs. 10 weeks, P=0.007). According to the final results of the Charité Onkologie trial (CONKO-003), the addition of oxaliplatin to 5-FU and leucovorin improves overall survival and progressionfree survival when compared to 5-FU and leucovorin [5]. Based on the above, it has been suggested that FOLFOX become a standard second-line regimen [6]. Some studies have demonstrated that the doublet of gemcitabine and oxaliplatin can be used as second-line treatment in patients refractory to standard gemcitabine regimen [7, 8]. Activity of oxaliplatin has also been shown in combination with capecitabine after gemcitabine failure [9]. These results were confirmed in a phase II study by Dr. Mane et al., presented at the 2011 ASCO GI Cancer Symposium (Abstract #308) [10], but it should be noted that the latter trial enrolled patients with pancreatic or biliary adenocarcinoma and that results were reported on the total of patients.
Regarding taxanes, paclitaxel monotherapy has been suggested as an additional therapeutic option with considerable efficacy and low toxicity in second-line treatment [11]. A recent retrospective study evaluated docetaxel monotherapy as well as docetaxel-based doublets in the treatment of refractory pancreatic cancer and mild activity was shown with no grade 3 or 4 toxicity [12].
Irinotecan has been evaluated in combination with oxaliplatin in patients with advanced pretreated pancreatic cancer exhibiting modest activity and manageable toxicity [13] and offering median overall survival of 4.1 months [14].
Irinotecan with 5-FU and folinic acid (FOLFIRI) showed notable activity and a good toxicity profile after gemcitabine failure [15, 6].
S-1, an oral fluoropyrimidin, has also been investigated in Japanese populations after failure of gemcitabinebased treatment. It seems that this agent is tolerable and marginally effective, offering median overall survival of 5.8 months [16, 17].
Targeted therapies are also being studied in refractory pancreatic cancer. The combination of bevacizumab and erlotinib was recently evaluated in this setting but despite good tolerability, the results were poor [18], as were the results of the use of everolimus [19] and sunitinib [20] as single agents. Bevacizumab monotherapy or its administration in combination with docetaxel did not show any antitumor activity after gemcitabine failure [21].
What Did We Learn at the 2011 ASCO GI Cancer Symposium?
With regard to treatment of refractory pancreatic cancer after failure of at least one line of therapy, two important abstracts were presented at the 2011 ASCO GI Cancer Symposium (Table 1). Both evaluated the use of irinotecan-based regimens in this treatment setting.
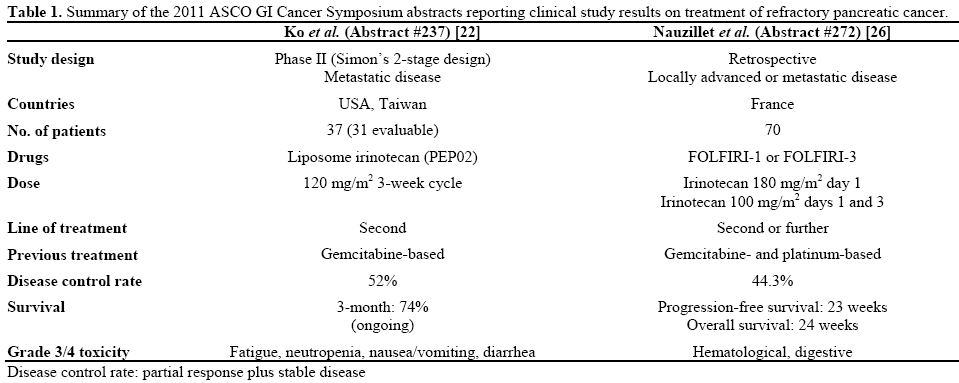
Dr. Ko et al. presented a phase II trial conducted in three centers in the USA and Taiwan (Abstract #237) [22]. They studied the use of single-agent PEP02, a novel nanoparticle liposome formulation of irinotecan, in refractory pancreatic cancer. It is characterized by improved pharmacokinetics and better tumor localization of irinotecan and of its active metabolite SN38, as compared to the free form of the drug. Favorable safety and efficacy of PEP02 were shown in previous phase I studies of patients with refractory solid tumors, such as pancreatic cancer [23, 24]. PEP02 has been studied as monotherapy [23] as well as in combination with 5-FU and leucovorin [24] and tumor response was reported. In the 2011 Ko et al. study [22], 37 patients with metastatic pancreatic cancer received triweekly PEP02 at a dose of 120 mg/m2 as second-line treatment after gemcitabine failure. According to results based on the first 31 evaluable patients, a 52% disease control rate was achieved. CA 19-9 levels decreased more than 50% in one third of patients whose baseline levels were originally elevated. The study met its primary endpoint of 3-month overall survival as the latter reached 74%, with one patient surviving for more than one year. Toxicity was considered acceptable, with fatigue (31%) and neutropenia (25%) being the two most common grade equal to, or greater than, 3 adverse events.
Regimens combining irinotecan with 5-FU and folinic acid (FOLFIRI) have been administered to patients with advanced pancreatic cancer in the first- [25] and second-line setting [15] and data from phase II studies have shown modest efficacy with tolerable toxicity. Gebbia et al. [6] conducted a relevant retrospective study in 40 patients with refractory pancreatic cancer. A new larger retrospective study, conducted in two French institutions, was presented by Dr. Neuzillet et al. at the 2011 ASCO GI Cancer Symposium reporting on the use of FOLFIRI after one or more lines of treatment (Abstract #272) [26]. It included 70 patients with unresectable, locally advanced or metastatic, pancreatic cancer with an overall maspin score less than 3. These patients had previously received gemcitabine and platinum-based chemotherapies. Approximately one third of patients had been administered one prior regimen, 57% had received two lines of treatment and only 8.8% had received three or more lines. Sixty of 70 patients (85.7%) received FOLFIRI-1 (irinotecan 180 mg/m2 day 1) and the rest were administered FOLFIRI-3 (irinotecan 100 mg/m2 days 1 and 3). Disease control rate was 44.3%. Oneyear and two-year progression-free survival was 17% and 3%, respectively, whereas overall survival rates were 24% and 9%, respectively. Dosage adjustment was necessary in 21 patients (30%) and adverse events were considered tolerable with no toxic deaths reported.
Discussion
Very few options are available for patients with advanced pancreatic cancer after failure of gemcitabine-based regimens. Irinotecan monotherapy has already been evaluated in patients treated with first-line gemcitabine-based chemotherapy: in 2009, Yi et al. [27] reported the results of a phase II trial evaluating biweekly doses of irinotecan monotherapy (150 mg/m2) as salvage treatment in this setting. However, Ko et al. [22] presented the first phase II study of a novel liposomal irinotecan formulation in the second-line treatment of these patients. In both trials, disease control rates were comparable (48 vs. 52% in the Yi and Ko studies, respectively) as were the percentages of patients that exhibited more than 50% decrease in their CA 19-9 levels (33% in both studies). In terms of survival, three-month overall survival seems considerably higher in the liposomal irinotecan study according to the preliminary data presented at the 2011 ASCO GI Cancer Symposium (74% vs. approximately 40% in the Yi et al. trial). However, it should be noted that with regard to toxicity, the liposomal formulation of irinotecan seems to be associated with a significant greater percentage of grade 3/4 adverse events. In this study, fatigue grade equal to, or greater than, 3 is reported in 31% of patients whereas in the Yi et al. study this adverse event was not reported. This difference in toxicity needs to be taken into account as treatment in the second-line setting is often palliative and one of its main objectives is maintaining quality of life.
FOLFIRI regimens have been studied in the past in the treatment of gemcitabine refractory pancreatic cancer. The Yoo et al. [15] phase II study was the first to show favorable efficacy and toxicity profile in gemcitabine pretreated patients. Gebbia et al. [6] retrospectively examined 40 patients who received standard biweekly FOLFIRI after gemcitabine failure and suggested this regimen be used selectively in patients with good performance status or good response to first-line treatment. The 2011 Neuzillet et al. [26] study was also retrospective and showed comparable efficacy results (50% vs. 44.3% disease control rates in the Gebbia et al. and Neuzillet et al. studies, respectively). Estimated median overall survival was 6 months in both studies and toxicity was mainly hematological and gastrointestinal. The Neuzillet et al. trial is the first study to report considerable efficacy and manageable toxicity in patients receiving third- and further-line of chemotherapy. However, what needs to be noted is that patients included were of significantly better performance status (42.9% had performance status equal to 0 vs. 15% and 0.5% in the Yoo et al. and Gebbia et al. studies, respectively), despite the fact that more than 65% of patients had already received 2 or more lines of treatment. In the Neuzillet et al. trial there is also great heterogeneity in the results despite the similar median overall survival of 6 months: the range of overall survival is 0.5-36.8 months vs. 2-8.2 months in the Gebbia et al. study, respectively. Finally, the Neuzillet et al. study does not state whether results or toxicity differed between patients receiving FOLFIRI-1 or FOLFIRI-3 regimens.
In conclusion, little progress has been made in the field of second-line treatment of gemcitabine-refractory pancreatic cancer; therefore, there is no evidence-based treatment recommendation for these patients. There is need for larger randomized trials that will study novel agents as well as new treatment combinations in an effort to improve survival while maintaining quality of life.
Conflict of interest
None
References
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010; 60:277-300. [PMID 20610543] 2. Li J, Saif MW. Advancements in the management of pancreatic cancer. JOP J Pancreas (Online) 2009; 10:109-117. [PMID 19287102]
- Li J, Saif MW. Advancements in the management of pancreatic
cancer. JOP J Pancreas (Online) 2009; 10:109-117. [PMID 19287102]
- Brus C, Saif MW. Second line therapy for advanced pancreatic adenocarcinoma: where are we and where are we going? Highlights from the "2010 ASCO Annual Meeting". Chicago, IL, USA. June 4- 8, 2010. JOP J Pancreas (Online) 2010; 11:321-323. [PMID 20601802]
- Oettle H, Pelzer U, Stieler J, Hilbig A, Roll L, Schwaner I, et al. Oxaliplatin/folinic acid/5-fluorouracil [24h (OFF) plus best supportive care versus best supportive care alone (BSC) in secondline therapy of gemcitabine-refractory advanced pancreatic cancer (CONKO 003). J Clin Oncol 2005 ASCO Annual Meeting Proceedings, Vol 23, No 16S (June 1 Supplement):4031.
- Pelzer U, Kubica K, Stieler J, Schwaner I, Heil G, Gorner M, et al. A randomized trial in patients with gemcitabine refractory pancreatic cancer. Final results of the CONKO 003 study. J Clin Oncol 2008 ASCO Annual Meeting Proceedings; Vol 26, No 15S (May 20 Supplement), 2008: 4508.
- Gebbia V, Maiello E, Giuliani F, Borsellino N, Arcara C, Colucci G. Irinotecan plus bolus/infusional 5-Fluorouracil and leucovorin in patients with pretreated advanced pancreatic carcinoma: a multicenter experience of the GruppoOncologico Italia Meridionale. Am J Clin Oncol 2010; 33:461-4. [PMID 20142727]
- Demols A, Peeters M, Polus M, Marechal R, Gay F, Monsaert E, et al. Gemcitabine and oxaliplatin (GEMOX) in gemcitabine refractory advanced pancreatic adenocarcinoma: a phase II study. Br J Cancer 2006; 94:481-5. [PMID 16434988]
- Fortune BE, Li X, Kosuri KV, Weatherby LM, Thomas JP, Bekaii-Saab TS. Fixed-dose-rate gemcitabine in combination with oxaliplatin in patients with metastatic pancreatic cancer refractory to standard-dose-rate gemcitabine: a single-institute study. Oncology 2009; 76:333-7. [PMID 19307739]
- Xiong HQ, Varadhachary GR, Blais JC, Hess KR, Abbruzzese JL, Wolff RA. Phase 2 trial of oxaliplatin plus capecitabine (XELOX) as second-line therapy for patients with advanced pancreatic cancer. Cancer 2008; 113:2046-52. [PMID 18756532]
- Mane J, Iruarrizaga E, Rubio I, Fonseca E, Iza R, Casas I, et al. Second-line chemotherapy with capecitabine (CAP) and oxaliplatin (OX) in patients with pancreatic or biliary tree adenocarcinoma (ADC).2011 Gastrointestinal Cancers Symposium. J Clin Oncol 2011; 29(Suppl. 4):Abstract 308.
- Oettle H, Arnold D, Esser M, Huhn D, Riess H. Paclitaxel as weekly second-line therapy in patients with advanced pancreatic carcinoma. Anticancer Drugs 2000; 11:635-638. [PMID 11081455]
- Saif MW, Syrigos K, Penney R, Kaley K. Docetaxel second-line therapy in patients with advanced pancreatic cancer: a retrospective study. Anticancer Res 2010; 30:2905-9. [PMID 20683031]
- Cantore M, Rabbi C, Fiorentini G, Oliani C, Zamagni D, Iacono C, et al. Combined irinotecan and oxaliplatin in patients with advanced pre-treated pancreatic cancer. Oncology 2004; 67:93-7. [PMID 15539911]
- Oh SY, Kim HJ, Kim TH, Lee GW, Kim HG, Jeong CY et al. Pilot study of irinotecan/oxalipltin (IROX) combination chemotherapy for patients with gemcitabine- and 5-fluorouracil-refractory pancreatic cancer. Invest New Drugs 2010; 28:343-9. [PMID 19444385]
- Yoo C, Hwang JY, Kim JE, Kim TW, Lee JS, Park DH, et al. A randomised phase II study of modified FOLFIRI.3vs modified FOLFOX as second-line therapy in patients with gemcitabine-refractory advanced pancreatic cancer. Br J Cancer 2009; 101:1658- 63. [PMID 19826418]
- Todaka A, Fukutomi A, Boku N, Onozawa Y, Hironaka S, Yasui H, et al. S-1 monotherapy as second-line treatment for advanced pancreatic cancer after gemcitabine failure. Jpn J Clin Oncol 2010; 40:567-72. [PMID 20189975]
- Nakai Y, Isayama H, Sasaki T, Sasahira N, Kogure H, Hirano K, et al. Impact of S-1 in patients with gemcitabine-refractory pancreatic cancer in Japan. Jpn J Clin Oncol 2010; 40:774-80. [PMID 20462979]
- Ko AH, Venook AP, Bergsland EK, Kelley RK, Korn WM, Dito E, et al. A phase II study of bevacizumab plus erlotinib for gemcitabine-refractory metastatic pancreatic cancer. Cancer Chemother Pharmacol 2010; 66:1051-1057. [PMID 20140876]
- Wolpin BM, Hezel AF, Abrams T, Blaszkowsky LS, Meyerhardt JA, Chan JA, et al. Oral mTOR inhibitor everolimus in patients with gemcitabine-refractory metastatic pancreatic cancer. J Clin Oncol 2009; 27:193-8. [PMID 19047305]
- O'Reilly EM, Niedzwiecki D, Hall M, Hollis D, Bekaii-Saab T, Pluard T, et al. A Cancer and Leukemia Group B phase II study of sunitinib malate in patients with previously treated metastatic pancreatic adenocarcinoma (CALGB 80603). Oncologist 2010; 15:1310-9. [PMID 21148613]
- Astsaturov IA, Meropol NJ, Alpaugh RK, Burtness BA, Cheng JD, Mc Laughlin S, et al. Phase II and Coagulation Cascade Biomarker Study of Bevacizumab With or Without Docetaxel in Patients With Previously Treated Metastatic Pancreatic Adenocarcinoma. Am J Clin Oncol 2011; 34:70-75. [PMID 20458210]
- Ko AH, Tempero MA, Shan Y, Su W, Lin Y, Dito E, et al. A multinational phase II study of liposome irinotecan (PEP02) for patients with gemcitabine-refractory metastatic pancreatic cancer. 2011 Gastrointestinal Cancers Symposium. J Clin Oncol 2011; 29(Suppl. 4):Abstract 237.
- Chen L, Chang T, Cheng A, Yang C, Shiah H, Chang J, Yeh G. Phase I study of liposome encapsulated irinotecan (PEP02) in advanced solid tumor patients. J Clin Oncol 2008 ASCO Annual Meeting Proceedings .Vol 26, No 15S (May 20 Supplement), 2008: 2565.
- Chen L, Shiah H, Chao T, Hsieh K, Chen G, Chang J, Yeh G. Phase I study of liposome irinotecan (PEP02) in combination with weekly infusion of 5-FU/LV in advanced solid tumors. J Clin Oncol 2010 ASCO Annual Meeting Proceedings, Vol 28, No 15_suppl (May 20 Supplement), 2010: e13024.
- Taieb J, Lecomte T, Aparicio T, Asnacios A, Mansourbakht T, Artru P, et al. FOLFIRI.3, a new regimen combining 5-fluorouracil, folinic acid and irinotecan, for advanced pancreatic cancer: results of an Association des Gastro-Enterologues Oncologues (Gastroenterologist Oncologist Association) multicenter phase II study. Ann Oncol 2007; 18:498-503. [PMID 17158774]
- Neuzillet C, Hentic O, Rousseau B, Rebours V, Bengrine- Lefevre L, Raymond E, et al. FOLFIRI regimen as second-/third-line chemotherapy in patients with advanced pancreatic adenocarcinoma refractory to gemcitabine and platinum salts: A retrospective series of 70 patients. 2011 Gastrointestinal Cancers Symposium. J Clin Oncol 2011; 29(Suppl. 4):Abstract 272.
- Yi SY, Park YS, Kim HS, Jun HJ, Kim KH, Chang MH, et al. Irinotecanmonotherapy as second-line treatment in advanced pancreatic cancer. Cancer Chemother Pharmacol 2009; 63:1141-5. [PMID 18839175]

