Huseyin Avni Solgun1* and Isa Ozyilmaz2
1Department of Pediatrics, Alt?nbas University Medical Park Bahcelievler Hospital, Istanbul, Turkey
2Department of Pediatrics Cardiology, Istinye University Medical Park Gaziosmanpasa Hospital, Istanbul, Turkey
*Corresponding Author:
Huseyin Avni Solgun
Department of Pediatrics
Alt?nbas University Medical Park Bahcelievler Hospital
Istanbul, Turkey
Tel: +902129793000
E-mail: hsynavn@gmail.com
Received date: December 10, 2018; Accepted date: January 09, 2019; Published date: January 17, 2019
Citation: Solgun HA, Ozyilmaz I (2019) Transient Coronary Vasospasm in a Newborn Due to Maternal Cannabis Use during Pregnancy. J Intensive Crit Care Vol.5 No.1:18
Copyright: © 2018 Solgun HA. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Cannabis; Neonatal; Coronary vasospasm; Pregnancy
Introduction
Cannabis is widely used around the world for their euphoric effects and generally identified a drug of low toxicity [1]. Cannabis is one of the most commonly used illicit drugs in pregnancy. It accounts prevalence of cannabis use at up to 5% of all pregnant women with generally self-reporting [2]. It has been documented variety of cardiovascular complications as coronary ischemia or Myocardial Infarction (MI), cardiomyopathy, sudden cardiac death [3,4]. Previously studies, there is no literature presented acute coronary ischemia in a new born of maternal use cannabis during pregnancy.
Here we showed transient coronary vasospasm in a new born due to maternal cannabis use during pregnancy.
Case Report
The new born patient was born at gestational age of 38 weeks via normal vaginal delivery at another hospital referred to our hospital because of transient tachypnea of neonate. The body weight was 3450 grams and height was 51 cm, respectively. On physical examination the general situation was severe, more reflex was hypoactive, respiratory rate was 55/per minute, cardiac rate was 168/per minute, in auscultation of heart there was 2-3/6 systolic murmur; blood pressure was 78/ 37 mm/Hg, capillary refill was 2 seconds. In history of family, maternal use of cannabis in full trimesters of pregnancy for every day have been note from mother, father and other relatives. Mother declared no other medications or illicit drugs use or labor complications during pregnancy. In follow ups of the patient, the ECG (electrocardiogram) showed ST segment elevation of 2 mm in VII and aVF leads (Figure 1).
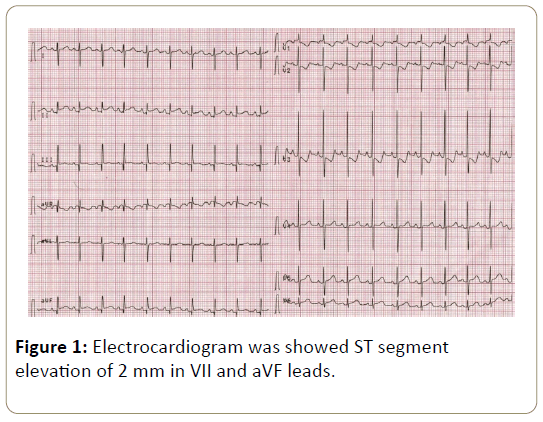
Figure 1: Electrocardiogram was showed ST segment elevation of 2 mm in VII and aVF leads.
Concurrently the blood level of high sensitive cardiac troponin (hs-cTnT) was 404 nanogram/mililiter [Normal: 0-139.36 (95° percentile)] [4], Creatine Kinase (CK) was: 296 microgram/litre (Normal: 26-192) and CK-MB was 50 milligram/litre (Normal: 7-25), respectively. The urine sample of patient’s analysis for cannabis was positive. The Acetylsalicylic Acid (ASA) treatment initiated as antiaggregant effect for acute coronary ischemia. An echocardiogram and coronary angiography (Figure 2) were performed and noted normally. Holter screening showed sinus tachycardia and clinical follow up also referred intermittent tachycardia. The follow up of ECG findings and cardiac troponin (hs-cTnT) levels returned to normal ranges at seventh day of treatment. At eleventh day after delivery the patient exchanged absolutely with normal findings of ECG (Figure 3) and cardiac troponin (hs-cTnT).
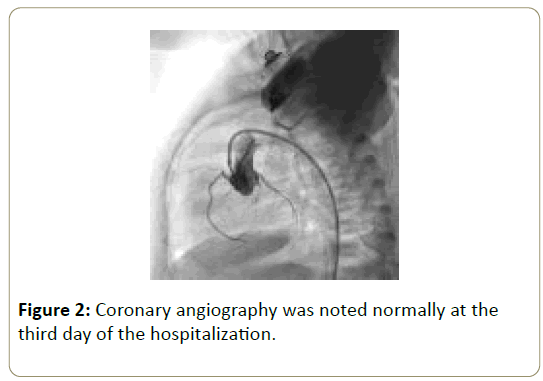
Figure 2: Coronary angiography was noted normally at the third day of the hospitalization.
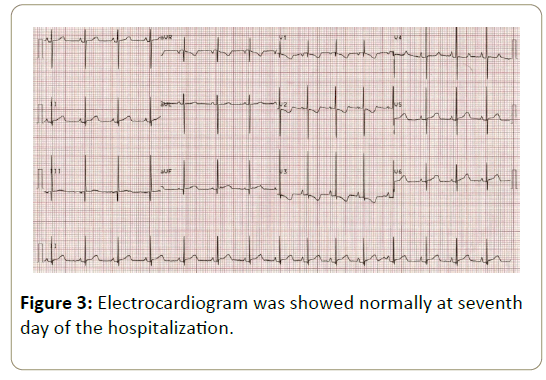
Figure 3: Electrocardiogram was showed normally at seventh day of the hospitalization.
Discussion
Cannabis use may cause various cardiovascular complications even in new born. Impaired peripheral vascular response is a substantial physiopathological mechanism in cardiac events [5]. Normally this reflex influences vasocontraction to prevent hypotension. Crescendo of preload may be effective to sustain sufficient perfusion. The blood flow of extremities ?ncreases with tachycardia, conjunctival hyperemia and postural hypotension. These effects are possible to be via b- adrenergic ?mpulse and parasympathetic nerve system blockage. Catecholamine boost may cause ischemia via arterial vasospasm and increased myocardial oxygen consumption [3]. Vasospasm is another physiopathological mechanism that can define coronary and cerebral ischemia cases which have normal conditions at effected tissues [3]. Apart from these effects; cannabis can induce side effects like angina, sinus tachycardia, bradycardia, atrioventricular blocks and atrial fibrillation either [1] besides that coronary microcirculation failure is possible after cannabis usage. Recently, either normal coronary artery in angiography the decreased coronary blood flow was shown in literature [4]. Via this decrease in coronary blood flow promote to myocardial infraction [6] especially it’s makeable that use of cannabis ?nduces MI risk 4.8 times higher and a decreased risk as time passes after usage of cannabis [7].
Diagnosis of differential in coronary ischemia should be absolutely thought congenital anomalies of the coronary arteries, coagulopathy and Coronary Artery Spasm (CAS) seconder to substance use. The echocardiography and coronary angiography of our patient referred no sign of coronary occlusion, coronary arterial anomaly or thrombus.
Recently in many studies the electrocardiographic effects of usage of cannabis was discussed. These are arrhythmias such as ventricular extra systole, ST segment and T wave alterations and P wave flattening [3]. In our patients' follow-up the ST segment elevation in ECG progressively disappeared and totally normal 24 hours rhythm Holter test accept sinus tachycardia referred the transient coronary vasospasm effect of cannabis usage.
In literature it’s shown that new born have cannabis usage ?n pregnancy tends to be low birth weight and ?ncreased ?ntens?ve care necessity [8]. Although these mark able knowledge the data for cardiac effects of cannabis usage ?n pregnancy is restricted. For this point of view our case is important to emphasize these issues.
In conclusion, cannabis use during pregnancy may induce coronary vasospasm and ischemia in new born. These patients should be followed closely in the intensive care unit. If necessary a coronary angiography should design to evaluate coronary arteries.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
None declared.
References
- Fisher BA, Ghuran A, Vadamalai V, Antonios TF (2005)Cardiovascular complications induced by cannabis smoking: a case report and review of the literature. Emerg Med J 22: 679-680.
- Jaques SC, Kingsbury A, Henshcke P, Chomchai C, Clews S, et al. (2014) Cannabis, the pregnant woman and her child: weeding out the myths. J Perinatol 34: 417-424.
- Bachs L, Mørland H (2001) Acute cardiovascular fatalities following cannabis use. Forensic Sci Int 124: 200-203.
- Thomas G, Kloner RA, Rezkalla S (2014) Adverse cardiovascular, cerebrovascular, and peripheral vascular effects of marijuana inhalation: what cardiologists need to know. Am J Cardiol 113: 187-190
- Weiss JL, Watanabe AM, Lemberger L, Tamarkin NR, Cardon PV (1972) Cardiovascular effects of delta-9-tetrahydrocannabinol in man. Clin Pharmacol Ther 13: 671-684.
- Karabulut A, Cakmak M (2010) ST segment elevation myocardial infarction due to slow coronary flow occurring after cannabis consumption. Kardiol Pol 68: 1266-1268.
- Safaa AM, Markham R, Jayasinghe R (2012) Marijuana-induced recurrent acute coronary syndrome with normal coronary angiograms. Drug Alcohol Rev 31: 91-94.
- Gunn JK, Rosales CB, Center KE, Nuñez A, Gibson SJ, et al (2016) Prenatal exposure to cannabis and maternal and child health outcomes: a systematic review and meta-analysis. BMJ Open 6: e009986.

