Keywords
Pancreatectomy; diabetes; Endocrine;
Pancreaticoduodenectomy
Abbreviations
TP Total Pancreatectomy; IPMN Intra-Ductal Papillary
Mucinous Neoplasms; MEN Multiple Endocrine Neoplasia; SMV
Superior Mesenteric Vein; PV Polycythemia Vera; MRCP Magnetic
Resonance Cholangiopancreatography; FBG Fasting Blood Glucose; PD
Pancreatoduodenectomy; PDAC Pancreatic Ductal Adenocarcinoma;
NET Neuroendocrine Tumor
INTRODUCTION
Total Pancreatectomy (TP), an infrequently done
surgery for pancreatic diseases, was first done in 1942 by
Eugene Rockey of Portland, Oregon [1]. Historically, TP
was considered a dreaded surgery due to its profound postoperative
complications ensuing exocrine and endocrine
pancreatic insufficiency. Later in the 1960s and 1970s, TP
was then increasingly performed for various indications,
firstly to abate the complications of anastomotic leak
following Whipples Pancreaticoduodenectomy, and also
for pancreatic cancers when it was considered that the
high recurrence rates after partial resection was due to
the multi-centric nature of the disease. Nevertheless, the
interest in elective TP waned with a clearer understanding
of the cancer biology, multidisciplinary approach to
pancreatic cancers and advanced management of postoperative
complications after partial pancreatectomy [2].
Over the decades the rates of TP have increased
with the excellent medical management of exocrine
and endocrine pancreatic insufficiency after TP. Today,
more specific indications for TP have emerged including
multifocal Intra-ductal papillary mucinous neoplasms (IPMN), multifocal neuroendocrine tumours in the setting
of Multiple Endocrine Neoplasia (MEN) syndrome, and
multifocal pancreatic metastases most commonly from
renal cell carcinoma and sometimes from melanoma,
extensive pancreatic adenocarcinoma when R0 resection
is not achieved with partial resection. It is also performed
as an emergency procedure to alleviate sepsis due to
pancreatic leak after partial resection [3].
Here we describe a case of multifocal pancreatic
adenocarcinoma who underwent total pancreatectomy
with splenectomy and the post-operative management of
the patient.
CASE REPORT
A 67 year old male, a chronic smoker and alcoholic,
presented with upper abdominal pain, dyspepsia, diabetes
and features of obstructive jaundice. Complete blood
investigations with renal and liver function tests with liver
enzymes were done and found to be within normal limits
except for poorly controlled blood sugar levels. He was
treated with subcutaneous regular and long acting insulin
and optimised for surgery. Multiphasic contrast enhanced
computed tomography and MRCP were done which showed
a mass lesion in the head of pancreas of size 2.9 × 2.9 cm and
another lesion in the body of pancreas of size 1.3 × 1.1 cm.
The second lesion was cystic lesion communicating with
main pancreatic duct and IPMN was suspected. The head
lesion was close to the SMV and SMV/PV confluence. The
remaining pancreatic parenchyma was not normal with
features of chronic pancreatitis. Hence total pancreatectomy
was planned. Intra-operatively it was found that the lesion in
the body of the pancreas was infiltrating the splenic vessels,
hence splenectomy done and removed en bloc with the
specimen. The intra-operative period was uneventful.
In the immediate post-operative period the patient was
kept nil per orally and the blood sugar was monitored and
insulin infusion was given with dextrose containing fluids,
and 40 to 50 units of Insulin were given daily. After starting
orals the insulin dose was titrated according to blood
sugar levels. For blood glucose level <180 mgs no Insulin
was given. For sugar levels of 180-220, 220-280, 280-
350 and >350 mgs, 4, 6, 8 and 10 units of regular insulin
were respectively given subcutaneously between postoperative
days 6 to 10. Later the patient was switched over
to subcutaneous insulin injections thrice a day combining regular and long acting insulin given approximately in
2:1 ratio. The blood sugar levels in the first 15 days after
surgery is shown in (Figure 1). The patient received
pancreatic enzyme supplements 20,000 units thrice daily.
The patient had multiple episodes of loose stools in the
early post-operative period and gradually improved with
the enzyme supplements with reduction in frequency and
solid consistency of stools. There was no wound related
morbidity. The patient recovered well and discharged on
the 18th post-op day. The histopathology was pancreatic
ductal adenocarcinoma (Figures 2, 3 and 4).
Figure 1. Blood sugar levels in post-op day 1-15.
Figure 2. CECT showing multifocal lesions in head and body of pancreas (Bold arrow – mass in the head of pancreas, Light arrow – mass in the body).
Figure 3. post resection image showing tumour bed.
Figure 4. specimen with entire pancreas with spleen.
DISCUSSION
Surgeries for pancreatic malignancies include Whipples
Pancreaticoduodenectomy, central pancreatectomy, distal
pancreatectomy and total pancreatectomy with several
modifications of these procedures. The treatment of
pancreatic diseases has continuously evolved, moreover
for malignant diseases, with the advent of adjuvant and
neoadjuvant therapies, more conservative procedures
with good oncologic outcomes are advocated. Due to
the improved results, today there are different and
more specific indications than before for TP. Malignant
tumors growing from the head into the left of pancreas,
Pancreatic head cancer where it is not possible to
achieve a tumor free resection margin with conventional
pancreaticoduodenectomy or with dubious changes in the
pancreatic main duct in frozen section, Recurrent cancer
in the pancreatic remnant, Rescue pancreatectomy for a
pancreatojejunostomy leak with sepsis or bleeding after
a Whipple resection, Multifocal IPMN with potentially
malignant foci present in all parts of the gland, Multiple
metastases of renal cell carcinoma and melanoma, Multifocal
neuroendocrine tumours in the setting of multiple
endocrine neoplasia. However, TP is still not a commonly
done surgery for pancreatic cancer; rate of TP compared
to pancreaticoduodenectomy is in the range of 10% [4, 5, 6]. In the prospective observational study by Werner et
al., the primary tumor was malignant in 377(87%) and
benign in 53(13%) of cases, majority of malignant tumours
were pancreatic ductal adenocarcinoma (n=289, 76.7%),
followed by IPMN (n=31, 8.2%) and NETs (n=23, 6.1%).
Most of the benign tumours were IPMN (n=44, 77.2%)
[3]. Similarly in a study by Ricardo et al. the majority of
tumours were PDAC (52.1%) and IPMN (20.5%) [7].
The post-operative outcomes after TP are comparable
to PD. In the study by Ricardo et al. comparing the outcomes
of TP (n=73) and PD (n=184), there were no statistically
significant differences in the overall mortality, morbidity,
length of stay, reoperation rates and readmission rates.
The mean overall survival for TP was 28 months (range 3-57 months) and 27 months for PD (range 18-36 months)
and no significant difference was found. The survival
for TP at 1, 3 and 5 years was 74, 48 and 31% and for
PD was 78, 45, and 37%. The QoL was analysed for the
two procedures with standard questionnaires which
showed no significant difference [7]. Müller et al, in his
study including 147 patients of TP for both elective and
emergency indications, showed that the post-operative
mortality and morbidity for elective TP was acceptable
(mortality 4.8% and morbidity 36%), and also found that
these were no significant differences in mortality and
morbidity compared to partial pancreatic resections done
during the same period [8, 9, 10, 11, 12, 13].
The post-operative morbidity included delayed
gastric emptying, SSI, sepsis, Intra-abdominal abscess,
early anastomotic ulcer, biliary leak, haemorrhage, and
pneumonia [11]. The post-operative morbidity in various
series varied between 37%-62%. The re-operation rates
ranged from 3-17% [14, 15]. There were no statistically
significant differences when compared to the PD [9]. The
morbidity reported in various studies are listed in (Table 1).

All patients become diabetic after TP due to total
loss of endocrine function of the pancreas, new onset
diabetes after PD range from 18-39%. The insulin
deficient state after TP has been termed “Brittle Diabetes”
(Pancreatogenic diabetes or Type-3c DM), due to wide
range of fluctuations in the blood sugar level which is
excessive and unpredictable. The increase in both insulin
sensitivity and Insulin binding capacity of RBCs can
lead to severe hypoglycemia. Furthermore, the counter
regulatory hormone Glucagon is also deficient leading to
unopposed action of insulin and severe hypoglycaemia
even with marginally excess dose of insulin [11]. Diabetic
ketoacidosis is rare in these patients unlike in those with
Type-2 DM. Insulin is given as continuous infusion along
with dextrose containing fluids in the early post-operative
period. Later combinations of rapid and long acting insulins
are given through sub-cutaneous injections [13]. Insulin
can also be delivered through Insulin pumps/ continuous subcutaneous insulin infusion. Recently, treatments with
long acting insulin preparations and specialized nurse led
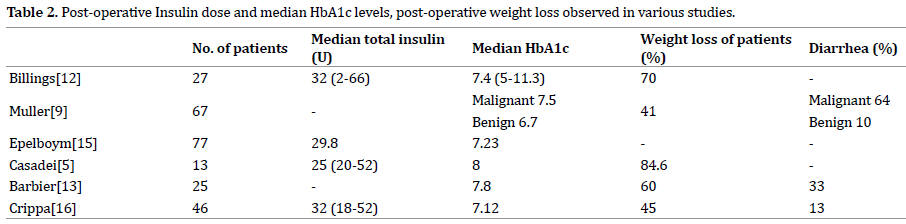
diabetic management have shown improved outcomes [14, 15]. The HbA1c levels can be maintained in an acceptable
range with effective insulin treatment. The median HbA1c
levels reported in various series are shown in (Table 2).
Pancreatic exocrine deficiency causes impairment
of fat digestion and leads to fat malabsorption, diarrhea,
steatorrhea, weight loss and hepatic steatosis. These
contribute to deficiency of fat soluble vitamins (A,D,E,K),
magnesium and trace elements, leading to malnutrition
related complications like osteopathy and osteoporosis
[16]. Treatment with pancreatic enzyme supplements and
nutritional interventions such as low fat diet can improve
the symptoms related to malnutrition. The standard
pancreatic enzyme replacement therapy is 40,000 – 50,000
units of lipase per day (range 25,000-450,000) [17, 18].
Patient education regarding the management of postoperative
diabetes and enzyme deficiency is of prime
importance. Pre-operatively, the patients should be
referred to an endocrinologist and advice regarding postoperative
use of insulin formulations and management of
diabetes should be given.
In a retrospective study evaluating the correlation
between post-operative nutritional status and the
complications, it was found that higher early postoperative
FBG levels and low early serum pre-albumin
levels were significantly associated with increased rates of
complications after TP. Post-operative HbA1c levels >7%
was associated with decreased recurrence-free survival
and was an independent risk factor for tumour recurrence
[19, 20]. Hence, good glycaemic control and nutritional
status is important in achieving optimal outcomes and
good QoL after TP.
CONCLUSION
In conclusion, TP is a feasible surgery with acceptable
mortality and morbidity and long term outcomes. The management of post-operative complications, especially
exocrine and endocrine insufficiency still poses a challenge
to the treating physician. However, optimal insulin therapy,
patient education, pancreatic enzyme supplements, change
in food habits all contribute to the maintaining quality of
life after TP.
Conflicts of Interest
All named authors hereby declare that they have no
conflicts of interest to disclose.
References
- Andrén-Sandberg A, Ansorge C, Yadav TD. Are There Indications for Total Pancreatectomy in 2016? Dig Surg 2016; 33:329-334. [PMID: 27215746]
- Karpoff HM, Klimstra DS, Brennan MF, Conlon KC. Results of total pancreatectomy for adenocarcinoma of the pancreas. Arch Surg 2001; 136:44-47. [PMID: 11146775]
- Hartwig W, Gluth A, Hinz U, Bergmann F, Spronk PE, Hackert T, et al. Total pancreatectomy for primary pancreatic neoplasms: renaissance of an unpopular operation. Ann Surg 2015; 261:537-546. [PMID: 24979606]
- Jethwa P, Sodergren M, Lala A, Webber J, Buckels JA, Bramhall SR, et al. Diabetic control after total pancreatectomy. Dig Liver Dis 2006; 38: 415-419. [PMID: 16527551]
- Casadei R, Monari F, Buscemi S, Laterza M, Ricci C, Rega D, et al. Total pancreatectomy: indications, operative technique, and results: a single centre experience and review of literature. Updates Surg 2010; 62:41-46. [PMID: 20845100]
- Datta J, Lewis RS Jr, Strasberg SM, Hall BL, Allendorf JD, Beane JD, et al. Quantifying the burden of complications following total pancreatectomy using the postoperative morbidity index: a multi-institutional perspective. J Gastrointest Surg 2015; 19:506-515. [PMID: 25451733]
- Casadei R, Ricci C, Taffurelli G, Guariniello A, Di Gioia A, Di Marco M, et al. Is total pancreatectomy as feasible safe efficacious and cost-effective as pancreaticoduodenectomy? A single center prospective observational study. J Gastrointest Surg 2016; 20:1595-607. [PMID: 27418262]
- Müller MW, Friess H, Kleeff J, Dahmen R, Wagner M, Hinz U, et al. Is there still a role for total pancreatectomy? Ann Surg 2007; 246:966-974. [PMID: 18043098]
- Barbier L, Jamal W, Dokmak S, Aussilhou B, Corcos O, Ruszniewski P, et al. Impact of total pancreatectomy: short- and long-term assessment. HPB (Oxford) 2013; 15:882-892. [PMID: 23458647]
- Ewald N, Hardt PD. Diagnosis and treatment of diabetes mellitus in chronic pancreatitis. World J Gastroenterol 2013; 19:7276-7281. [PMID: 24259958]
- Billings BJ, Christein JD, Harmsen WS, Harrington JR, Chari ST, Que FG, et al. Quality-of-life after total pancreatectomy: is it really that bad on long-term follow-up? J Gastrointest Surg 2005;9:1059-1067. [PMID: 16269376]
- Watanabe Y, Ohtsuka T, Matsunaga T, Kimura H, Tamura K, Ideno N, et al. Long‐term outcomes after total pancreatectomy: Special reference to survivors’ living conditions and quality of life. World J Surg 2015; 39:1231-1239. [PMID: 25582768]
- Epelboym I, Winner M, DiNorcia J, Lee MK, Lee JA, Schrope B, et al. Quality of life in patients after total pancreatectomy is comparable with quality of life in patients who undergo a partial pancreatic resection. J Surg Res 2014; 187:189-196. [PMID: 24411300]
- Crippa S, Tamburrino D, Partelli S, Salvia R, Germenia S, Bassi C, et al. Total pancreatectomy: indications, different timing, and perioperative and long-term outcomes. Surgery 2011; 149:79-86. [PMID: 20494386]
- Schmidt CM, Glant J, Winter JM, Kennard J, Dixon J, Zhao Q, et al. Total pancreatectomy (R0 resection) improves survival over subtotal pancreatectomy in isolated neck margin positive pancreatic adenocarcinoma. Surgery 142:572-580. [PMID: 17950350]
- Layer P, Holtmann G. Pancreatic enzymes in chronic pancreatitis. Int J Pancreatol 1994; 15:1-11. [PMID: 8195638]
- Hata T, Ishida M, Motoi F, Sakata N, Yoshimatsu G, Naitoh T, et al. Clinical characteristics and risk factors for the development of postoperative hepatic steatosis after total pancreatectomy. Pancreas 2016; 45:362-369. [PMID: 26495776]
- Nakajima K, Oshida H, Muneyuki T, Kakei M. Pancrelipase: an evidence‐based review of its use for treating pancreatic exocrine insufficiency. Core Evid 2012; 7:77-91. [PMID: 22936895]
- Shi HJ, Jin C, Fu DL. Impact of postoperative glycemic control and nutritional status on clinical outcomes after total pancreatectomy. World J Gastroenterol 2017; 23:265-274. [PMID: 28127200]
- Cheon YK, Koo JK, Lee YS, Lee TY, Shim CS. Elevated hemoglobin A1c levels are associated with worse survival in advanced pancreatic cancer patients with diabetes. Gut Liver 2014; 8:205-214. [PMID: 24672663]





