Keywords
Islets of Langerhans Transplantation; Pancreatectomy; Pancreatitis, Chronic
INTRODUCTION
Affecting approximately 0.2 – 0.6% of the population, chronic pancreatitis (CP) is an inflammatory condition characterized by irreversible, permanent and progressive fibrotic destruction of the pancreatic parenchyma which can result in chronic pain as well as endocrine and exocrine dysfunction. Total pancreatectomy with islet cell auto transplantation (TP-IAT) is an effective option in selected CP patients refractory to other treatments. In the following review, we highlight traditional and controversial indications for TP-IAT, its published outcomes to date, as well as important aspects of the surgical technique including the advent of minimally invasive approaches.
ETIOLOGY OF CHRONIC PANCREATITIS
A large number of predisposing factors and conditions can lead to CP. This list includes pancreas divisum, recurrent acute pancreatitis, autoimmune disease, congenital small pancreatic duct, trauma, hypertriglyceridemia and gallstones. Despite these many associations, alcohol abuse remains the most identifiable cause of CP in the United States. In a report by Coté et al, 45% of 539 patients with CP enrolled in the North American Pancreatitis Study-2 were found to have alcohol as the identifiable etiology [1]. These results have been corroborated by a multicenter prospective Italian report published in 2009; Frulloni et al examined 893 patients and found that heavy alcohol consumption (more than 80g of alcohol/day for more than 5 years) was the most important risk factor for CP [2]. Consequently, alcohol induced CP remains a common indication for TP [3]. Interestingly, despite alcohol’s dominant pathogenic role, less than 10% of alcohol dependent patients will develop CP, implying the interplay of other factors in disease development [4]. Currently, these susceptibility factors remain elusive, though many are postulated to be genetic in nature, and some of them have also been linked to hereditary pancreatitis [5, 6].
Hereditary pancreatitis is an uncommon cause of CP, but a frequent indication for TP-IAT. It is defined as two or more individuals with pancreatitis in two or more generations of a family, or pancreatitis associated with a known disease-causing germline mutation [7]. The latter is characterized by one of three mutations. Protease, serine, 1 (trypsin 1), also known as PRSS1, encodes the major pancreatic digestive enzyme trypsin. Gain of function mutations in this gene are responsible for most of the autosomal dominant causes of hereditary pancreatitis [8,9]. Autosomal recessive hereditary pancreatitis is associated with mutations in SPINK1 and CFTR. SPINK1 (Serine Protease Inhibitory Kazel-type 1) encodes a trypsin inhibitor that is expressed as an acute phase reactant in acinar cells during an inflammatory process. Loss of function mutations in SPINK1 predispose patients to CP and it is thought that approximately 2% of healthy individuals carry a heterozygous mutation in SPINK1 with less than 1% of those carriers developing disease [10,11]. Finally, mutations in CFTR (cystic fibrosis trans membrane regulator protein) are associated with both recurrent acute and chronic pancreatitis. CFTR is responsible for fluid secretion in the pancreatic duct cells and functions to “wash” the ductal environment of zymogens that are then carried into the duodenum where they are activated. Disruption of this process leads to retention of zymogens in the pancreas leading to acute and chronic pancreatitis [9,12]. Interestingly, although hereditary pancreatitis presents relatively early, most causes of pancreatitis in children and young adults are idiopathic [13].
TREATMENT OF CHRONIC PANCREATITIS
Regardless of the cause, CP results in multiple chronic medical problems that have a significant impact on a patient’s quality of life. Sequelae include chronic pain, increased risk for developing pancreatic ductal adenocarcinoma, malabsorption/steatorrhea that leads to multiple nutritional deficiencies (exocrine dysfunction), and endocrine dysfunction leading to diabetes mellitus [14]. The most debilitating aspect of the disease is the chronic, intractable pain that is typically very difficult to manage and is multifactorial in origin [15]. Treatment often occurs in a stepwise progression; initially with dietary modification, pancreatic enzyme supplementation and non-narcotic analgesia. This usually progresses to narcotic analgesia often requiring the guidance of a pain specialist. Refractory pain results in the need for more aggressive procedures such as endoscopic pancreatic decompression [16], celiac plexus nerve blocks [17], and extracorporeal shock wave lithotripsy [18]; all of which have been met with varying success.
Surgical therapy for CP was pioneered in the 1950’s and focuses on resection of the distal pancreas and decompression of the remnant pancreatic duct. The distal pancreatectomy and splenectomy, with an end-to-end pancreaticojejunostomy was initially reported by Duval in 1954 and has since undergone multiple iterations [19]. Puestow and Gillesby modified it in 1958 by performing a longitudinal pancreaticojejunostomy, splenectomy, and distal pancreatectomy to obtain better ductal drainage [20]. However since both procedures neglected to adequately drain the pancreatic head, a purely drainage procedure was developed by Partington and Rochelle (also known as the modified Puestow-Gillesby procedure) in which the anterior surface of the pancreas and duct are incised and anastomosed from head to tail with a Roux-en-Y jejunal loop. This procedure is still the most commonly performed pancreatic decompressive operation [21, 22]. While effective pain relief can be obtained, a patient must have a dilated pancreatic duct and no evidence of a pancreatic head mass [23]. When these stipulations are not met, a high quality preoperative workup including MRI with MRCP and endoscopic ultrasound can often localize abnormal areas within a diseased pancreas, allowing for one of the subtotal pancreatectomy procedures to be performed: A duodenum-preserving pancreatic head resection (Beger procedure) [24], Frey procedure [25], or a pancreaticoduodenectomy [26-29]. These procedures allow for good pain relief for head dominant disease; however, recurrence of pain is common and occurs in up to 50% of patients [23]. If preoperative imaging reveals diffuse small duct disease, or if any of the above procedures ultimately fail, a total pancreatectomy with or without islet cell auto transplantation becomes a reasonable option.
TOTAL PANCREATECTOMY WITH ISLET CELL AUTOTRANSPLANTATION
First reported at the University of Minnesota in 1977, the rational for performing TP-IAT is removal of the inflammatory source (and future cancer risk) while simultaneously harvesting and reintroducing the islet cells to maintain endocrine function. Directed resection (Whipple vs. subtotal pancreatectomy) is clearly the preferred method of treatment for disease that can be localized to the head or body/tail of the pancreas; however, TP-IAT has become a feasible option for patients with diffuse small duct disease who are not yet insulin dependent [30, 31]. TP-IAT has the distinct advantage of allowing patients the ability to avoid the significant postoperative complication of surgically induced brittle diabetes [30]. The severity of brittle diabetes, a condition in which a patient experiences both severe hyper and hypoglycemic episodes, should not be underestimated; in one early series, 50% of late deaths after TP were secondary to iatrogenic hypoglycemic episodes [32]. Although total pancreatectomy in the era of modern endocrine and exocrine replacement therapy has witnessed improvements in long-term morbidity and mortality, it remains one of the most morbid abdominal operations performed today [33-38].
Indications for TP-IAT
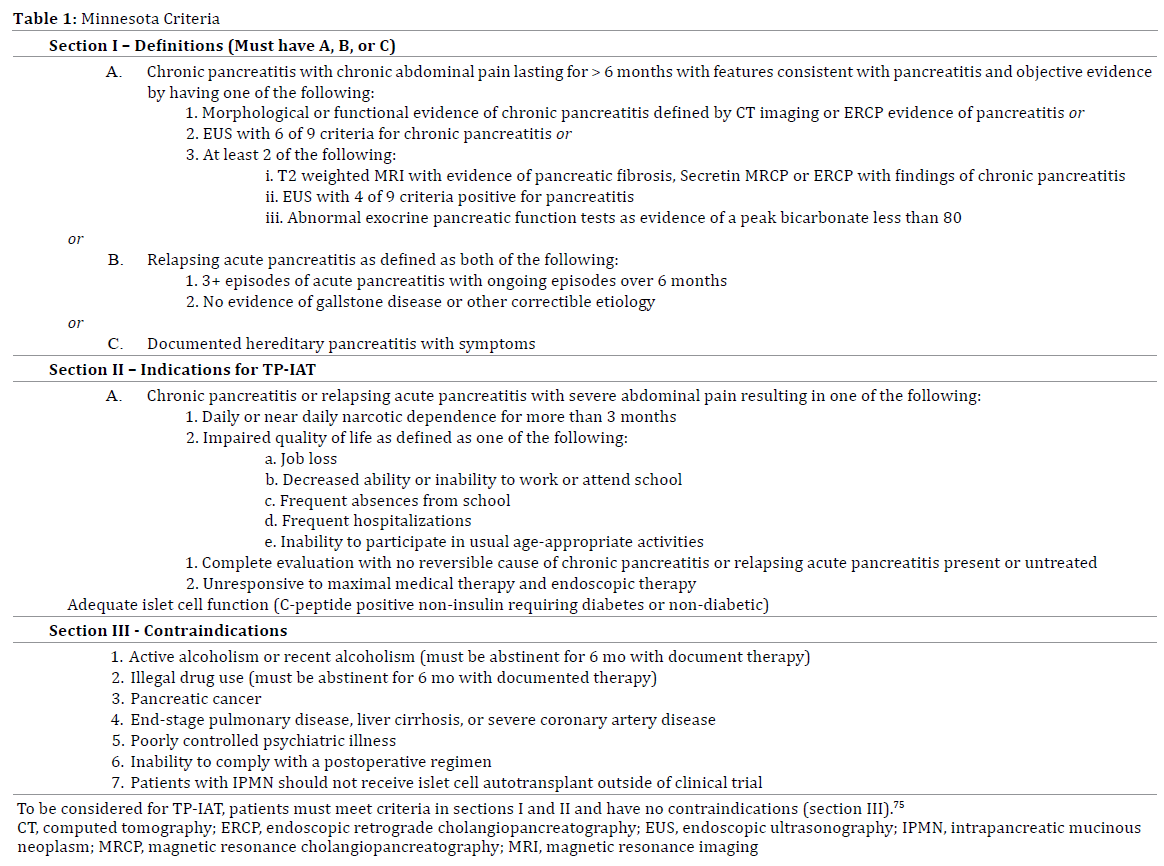
The classical indication for TP-IAT is CP leading to intractable abdominal pain that leads to an impaired quality of life. Patients must have failed other treatment strategies, and have preserved islet cell function. Preoperative considerations that warrant extensive patient discussion include the irreversibility of the operation, possible pain recurrence (10-20%), incomplete or variable diabetic protection, risk of serious life threatening complications and potential for gastric motility dysfunction [39]. Importantly, a multidisciplinary approach utilizing the expertise of surgeons, pain specialists, gastroenterologists, endocrinologists, psychologists, and social workers must be utilized. Patients should preferably have a strong support network as they must be able to adhere to strict postoperative medical management; consequently, any active psychosocial issues such as alcohol use represent a contraindication to the procedure.
Although IAT is performed for a number of etiologies, patients with hereditary pancreatitis will likely derive the most benefit since their pain is unlikely to abate without intervention, their symptoms are more severe, and disease onset occurs at an earlier age. Furthermore, this subset of patient’s harbors an elevated risk of pancreatic ductal adenocarcinoma, is usually healthier with less comorbidities, and lacks the psychosocial disturbances and malnutrition seen with CP secondary to alcoholism.
In patients with alcoholic CP, TP-IAT has been met with varying success. Based on their analysis of 30 cases, Dunderdale et al argue that the procedure should not be performed in this subset of CP patients. In their study, TPIAT was associated with a 23% islet cell isolation failure rate, a lower islet cell yield (1,265 vs 2,189 IEQ/kg), reduced quality of life (SF-36 and McGill Pain Questionnaire) scores at 2 years, and an increased postoperative insulin requirement when compared to patients undergoing TPIAT for nonalcoholic CP [40]. Consequently, enthusiasm for performing such a complex and costly procedure for this patient population has diminished.
Currently, the indications and contraindications for TPIAT are defined by the Minnesota Criteria (Table 1). It should be noted however that TP-IAT has also been reported in patients without CP, leading some to call for the expansion of those indications. For instance, TP-IAT has been performed for autoimmune pancreatitis resistant to steroid therapy [41], patients with cystic and benign neoplasms [42, 43], those with ampullary adenocarcinoma [44], and in the setting of pancreatic trauma [45, 46].
Of special interest is the use of TP-IAT for the treatment of pancreatic neoplasms. While strongly contraindicated by the Minnesota Criteria due to the fear of iatrogenic dissemination of neoplasia, a recent study by Balzano et al in which 31 malignant cases underwent TP-IAT is provocative. Of the 31 patients, 14 had neoplasms with no or low malignant potential (serous cystoadenomas, adenoma of the ampulla of Vater, low grade neuroendocrine tumors, mucinous cystic neoplasms with moderate dysplasia, intraductal papillary mucinous neoplasm with moderate dysplasia, and solid pseudopapillary neoplasm) and all were alive and disease free at a median followup of 491 days. Seventeen patients had adenocarcinoma (9 of which were pancreatic); at a median follow-up of >2 years, 13 were disease-free, 2 already had liver metastasis at time of surgery, and 2 developed recurrence (however these recurrences were not in the liver- the site of islet cell engrafment) [47]. Despite this study, current recommendations advise against the use of islet cell auto transplantation in patients with known pancreatic or periampullary malignancy.
Other contraindications to IAT include C-peptide negative diabetes, type 1 diabetes, portal vein thrombosis (if the portal vein is the intended site of islet cell auto transplantation), liver disease, or high-risk cardiopulmonary disease [39].
Optimal Timing of TP-IAT
The optimal timing for performing TP-IAT is less controversial, with most investigators supporting earlier treatment when possible [39]. The ideal timing should result in resolution of symptoms prior to the development of central sensitization and opioid-induced hyperalgesia, which can otherwise lead to chronic pain recurrence after TP. Residual islet function and islet cell yield should also be factored in when considering timing of TP-IAT; both presumed to be superior earlier in disease [39]. In a study of 18 pediatric TP-IAT patients, Kobayashi found that fibrosis and acinar atrophy, previous ductal drainage surgeries, and longer duration of CP negatively affected islet cell yield. These findings were reaffirmed with a recent large report from the same institution [48, 49]. Recently published data evaluating TP-IAT in 75 children also found that younger children (less than 12 years of age) had reduced post op complications and a higher chance of insulin independence compared to their older counterparts [49]. New preoperative MRI imaging techniques that aim to specifically assess the viability of islet cells and predict islet cell yield may help guide optimal operative timing in the near future [50].
Surgical Considerations
The surgical approach to TP-IAT has gradually evolved over the past decade, but the core tenets of the procedure still hold true; minimization of pancreatic trauma during dissection and preservation of the arterial blood supply until extirpation of the organ. Both principles minimize warm ischemic time and are believed to result in higher islet cell yields. Some notable differences in technique include: performance of a splenectomy, approach to the biliary reconstruction (choledocoduodenostomy vs Rouxen- Y hepaticojejunostomy), and pyloric preservation vs resection. Recently, TP-IAT has been performed in minimally invasive fashion [43, 49, 51-54].
One notable difference in technique is preservation versus transection of the pancreatic neck during operative dissection. Transecting the neck may facilitate an easier dissection, but disrupting the pancreatic parenchyma may unnecessarily decrease islet cell yield [55]. Another difference is the location and route of islet cell infusion. Most published reports favor cannulation of the splenic vein stump or portal vein at the time of operation; indeed, the first case of successful islet cell infusion in a patient with type 1 diabetes utilized this route [49, 53, 56-58]. However, a postoperative infusion of cultured islet cells within 48 hours by cannulation of the portal vein via a transhepatic percutaneous route under fluoroscopic guidance, and delivery of islet cells to the pelvic bone marrow have also been reported [47, 59].
Portal vein infusion of auto transplanted islet cells may be complicated by increased rates of transaminitis, portal vein thrombosis, and bleeding, as well as acute portal pressure elevations likely due to the non-purified nature of the cells (as compared with allogeneic islet cell transfusions) [60- 62]. The tissue volume being infused, and more likely the transient change in portal pressure, are associated with increased rates of complications [61]. Since the tissue volume per kilogram body weight (TV/kg) is a predictor of change in portal pressure (Figure 1), a TV/kg of less than 0.25 mL has been proposed as a safe volume to infuse. Patients receiving greater volumes are more likely to have a change in portal pressure of greater than 25 cm H2O, which is associated with a higher risk of portal venous thrombosis [61]. Due to these challenges, other alternative sites for islet cell engraftment have been proposed, however their clinical use has been limited [59, 63]. At this time, no convincing data exists to support many of these differences in surgical techniques, and technical decisions are usually based on the preference and experience of the operating surgeon.
Figure 1. Formula for estimating change in portal pressure with a given tissue volume (X) to be infused [54].
Outcomes of TP-IAT
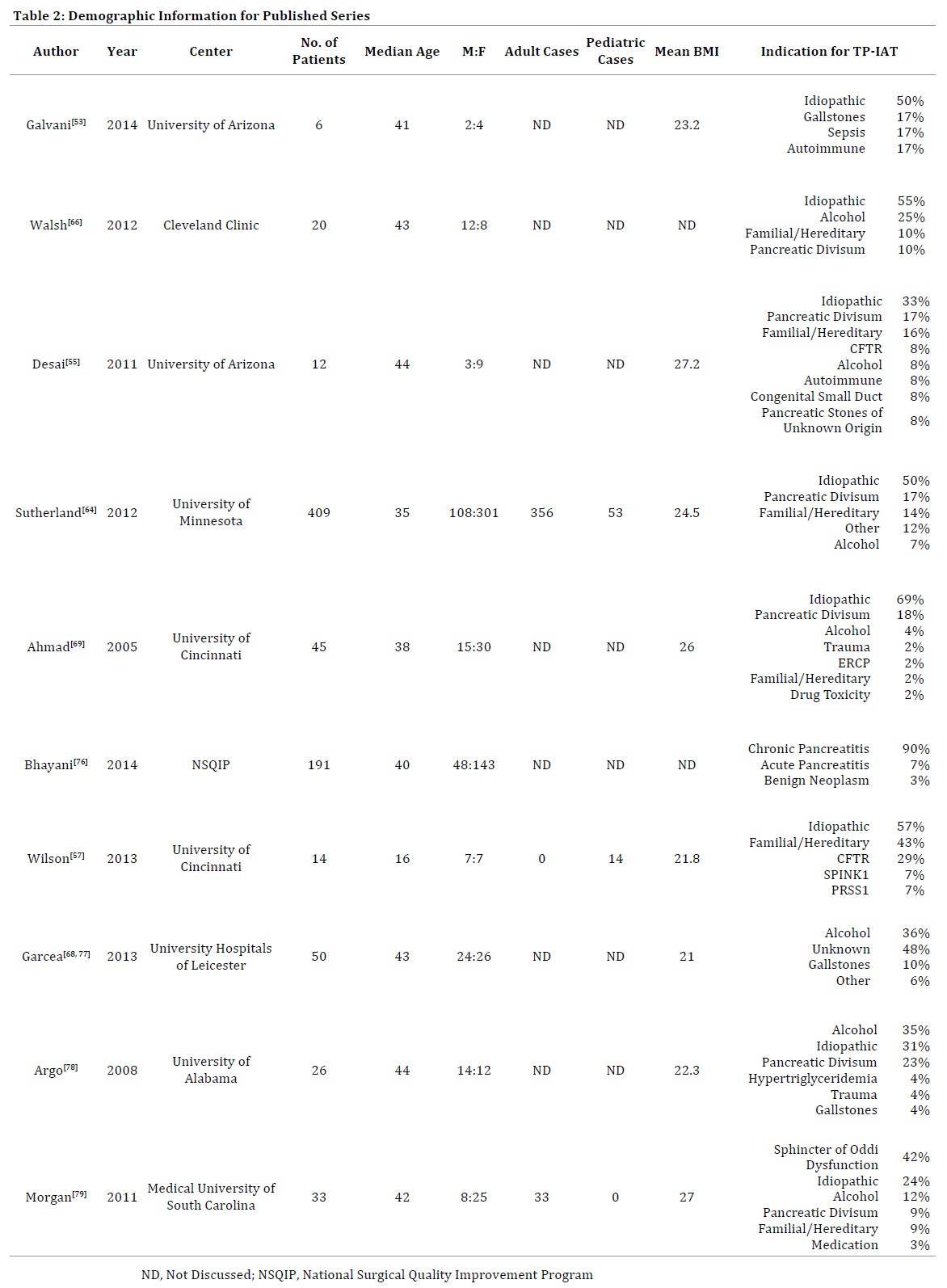
Multiple reports have now confirmed the safety and feasibility of TP-IAT [64, 65]. Additionally, the beneficial impact of the procedure on the quality of life for CP patients is well documented (Tables 2-4) [56, 64, 66-68]. The largest series of open TP-IATs to date has been reported by Sutherland et al at the University of Minnesota, analyzing 412 TP- IATs (355 adults and 53 children) from 1977 until 2011 [64]. The authors found insulin independence and partial islet cell function to be highly dependent upon the islet equivalents per kilogram transplanted. Impressively, at 3 years, patients who received > 5.000 IE/kg had an insulin independence rate of 72%, a partial function rate of 24%, with only 4% being insulin dependent. SF-36 survey scores, which report the health status profile of a patient along 8 separate categories, were analyzed for cases performed after 2007. At 2 years post TP-IAT, scores across all categories were significantly higher, Additionally, patient’s perceptions of their health status was improved in 84% of cases at 1 year, and in 57% of patients at 2 years. Furthermore, at 2 years post TP-IAT, 59% of patients were narcotic independent.
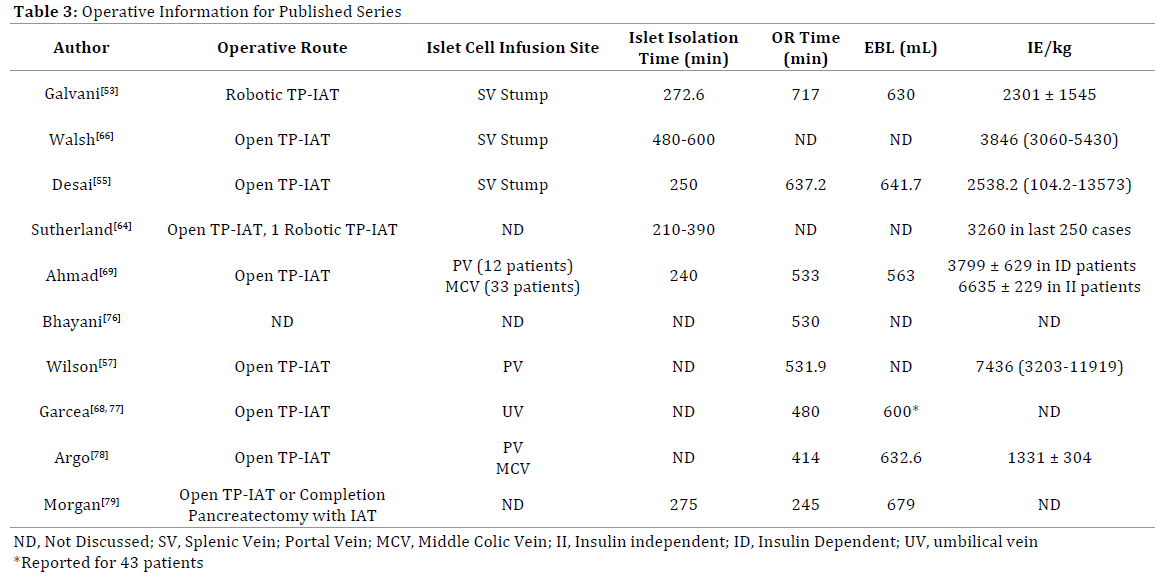
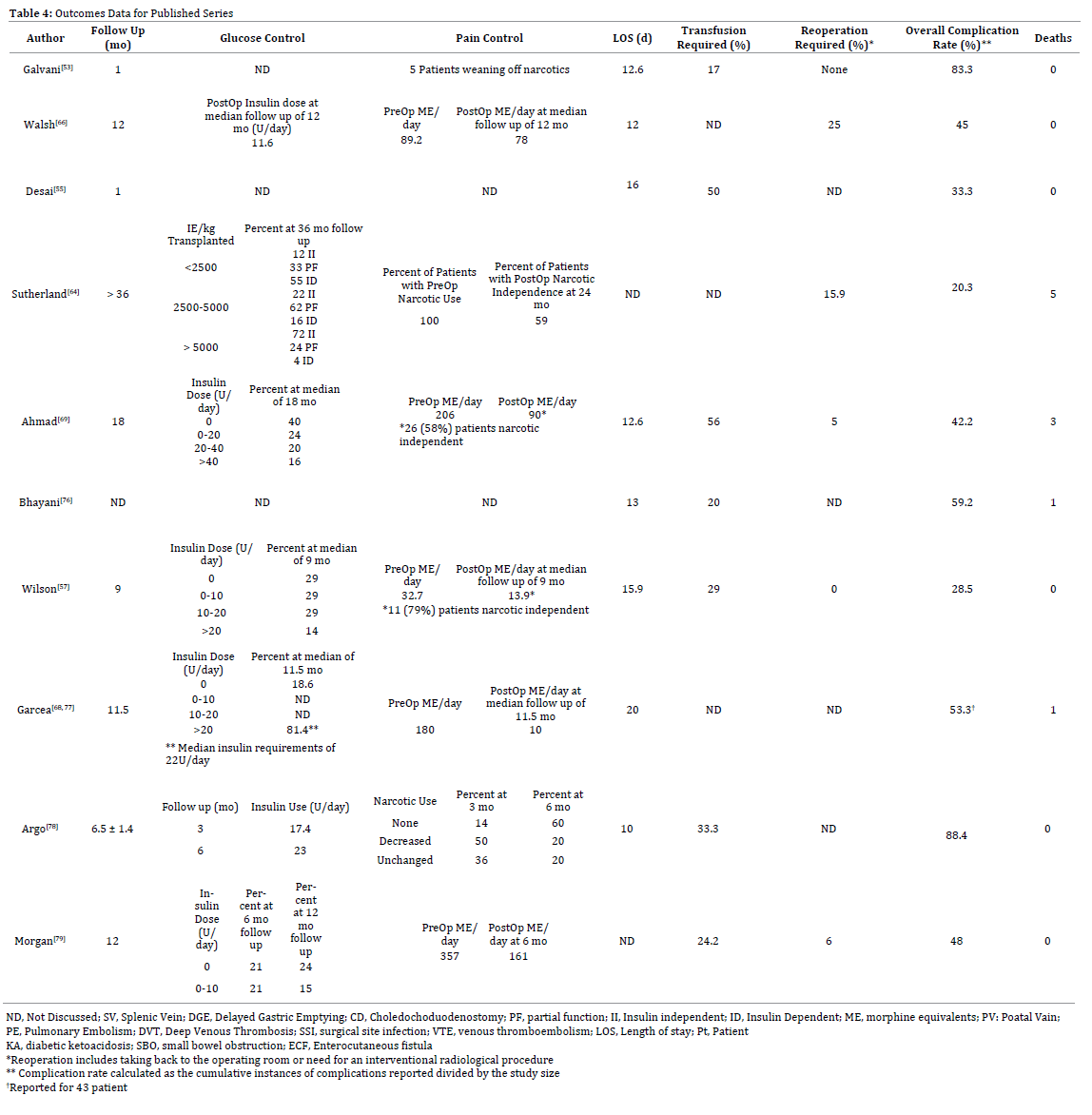
Another large series from the University of Cincinnati by Ahmad and colleagues reporting on 45 TP-IAT’s over 4 years, also found that insulin independence correlated with IE/kg infused on univariate analysis (p=0.04) [69]. Patients that were insulin independent (40% at 18 months) received a mean IE/kg of 6635 compared to 3799 in the insulin dependent group. Regarding pain control, the results of the Cincinnati series correlate strikingly with the Minnesota series in that 58% of patients were narcotic independent post TP-IAT. In a recent follow up study from the same institution, Wilson et al analyzed the results of TP-IAT in 14 children, and found 79% of them to be narcotic independent at follow up. Only 29% of patients however were insulin independent at the same time [57]. Tables 3 and 4 illustrate outcomes associated with the largest reported TP-IAT series to date.
Minimally Invasive TP-IAT
The aim of applying minimally invasive techniques to TP-IAT is to replicate the benefits seen with laparoscopic and robotic pancreatic resections: namely reduced blood loss, shorter recovery, quicker return to function, and improved quality of life. Various reports of laparoscopic TP have recently surfaced, indicating that the operation can be done with equivalent outcomes to historic controls in carefully selected patients [51, 52, 70-74]. Laparoscopic TP-IAT however, has yet to be reported.
Most recently, Galvani et al reported a case series of six patients undergoing TP-IAT using the robotic platform [53]. The authors were able to perform the procedure in pure minimally invasive fashion while simultaneously keeping warm ischemia time down to a minimum; an operative hallmark of the open approach. Operative time, blood loss, and islet cell yield were comparable to a recently published open case series of 12 patients by Desai et al [55]. The comparison of these two studies is significant since Galvani’s case series is a robotic adaptation of Desai’s technique, which was the first to describe the extirpation of the whole pancreas without dividing the pancreatic neck [53].
Authors Experience with Minimally Invasive TP-IAT
At our center, most TP-IATs are performed using the open approach. We prefer a pylorus preserving TP (no division of the pancreatic neck) with splenectomy, Rouxen- Y hepaticojejunostomy, and gastrojejunostomy. We favor islet cell infusion via a short splenic vein stump. Additionally, we are increasingly utilizing the robotic platform to perform complex pancreatic resections and reconstructions. Similar to the report by Galvani et al, we have also established the safety and feasibility of performing robotic TP with or without IAT (TP=10 patients, TP-IAT=3) [54]. All 3 IATs were performed without conversion while adhering to principles of the open approach; namely, avoiding division of the pancreatic neck and minimizing warm ischemia time. Results from the TP-IAT were encouraging, with a mean operative time (including islet cell preparation) of 600 minutes, mean EBL of 600 mL, and a mean LOS of 10.7 days (personal observation, corresponding author). Islet cell yields (mean 4563 IE/kg) were equivalent to historic controls. No mortality or major morbidity was recorded.
The addition of robotics however, may impact the cost of an already costly procedure. A cost analysis for TP-IAT in 60 patients at Leicester University revealed TP-IAT to be approximately UK £10,000 more expensive than TP without IAT [68]. This is likely to increase further when the cost of robotics is included. Despite this downfall, this cost burden may be offset if the benefits of robotic TP-IAT parallel those seen for other minimally invasive procedures in terms of post operative recovery and quality of life assessment.
CONCLUSION
Total pancreatectomy and islet cell auto transplantation has proven to be effective in improving the quality of life for patients suffering from chronic pancreatitis refractory to other treatments. However, due to the need for highly specialized infrastructure and expertise, it is only available at a small number of centers worldwide. While indications for TP-IAT continue to evolve, careful patient selection and early patient referral are important factors in optimizing outcomes. The application of newer technologies including robotics may reduce the morbidity associated with TP, however a detailed and rigorous assessment of these platforms is yet to be performed.
Conflict of Interest
Authors have no conflicts of interest
References
- Cote GA, Yadav D, Slivka A, et al. Alcohol and smoking as risk factors
in an epidemiology study of patients with chronic pancreatitis. Clinical
gastroenterology and hepatology : the official clinical practice journal of
the American Gastroenterological Association 2011; 9: 266-73; quiz e27. [PMID: 21029787]
- Frulloni L, Gabbrielli A, Pezzilli R, et al. Chronic pancreatitis: report
from a multicenter Italian survey (PanCroInfAISP) on 893 patients.
Digestive and liver disease : official journal of the Italian Society of
Gastroenterology and the Italian Association for the Study of the Liver
2009; 41: 311-7. [PMID: 19097829]
- Ong SL, Gravante G, Pollard CA, Webb MA, Illouz S, Dennison AR. Total
pancreatectomy with islet autotransplantation: an overview. HPB : the
official journal of the International Hepato Pancreato Biliary Association
2009; 11: 613-21. [PMC: 2799613]
- Dufour MC, Adamson MD. The epidemiology of alcohol-induced
pancreatitis. Pancreas 2003; 27: 286-90. [PMID: 14576488]
- Brock C, Nielsen LM, Lelic D, Drewes AM. Pathophysiology of chronic
pancreatitis. World journal of gastroenterology : WJG 2013; 19: 7231-40.
[PMC: 3831204]
- Vonlaufen A, Wilson JS, Pirola RC, Apte MV. Role of alcohol metabolism
in chronic pancreatitis. Alcohol research & health : the journal of the
National Institute on Alcohol Abuse and Alcoholism 2007; 30: 48-54. [PMID: 17718401]
- LaRusch J, Solomon S, Whitcomb DC. Pancreatitis Overview. In:
Pagon RA, Adam MP, Ardinger HH, et al., eds. GeneReviews(R). Seattle
(WA)2014. [NBK: 190101]
- Rebours V, Boutron-Ruault MC, Schnee M, et al. The natural history
of hereditary pancreatitis: a national series. Gut 2009; 58: 97-103. [PMID:
18755888]
- Applebaum-Shapiro SE, Finch R, Pfutzer RH, et al. Hereditary
pancreatitis in North America: the Pittsburgh-Midwest Multi-Center
Pancreatic Study Group Study. Pancreatology : official journal of the
International Association of Pancreatology 2001; 1: 439-43. [PMID:
12120221]
- Fink EN, Kant JA, Whitcomb DC. Genetic counseling for nonsyndromic
pancreatitis. Gastroenterology clinics of North America 2007; 36: 325-33,
ix. [PMID: 17533082]
- Pfutzer RH, Barmada MM, Brunskill AP, et al. SPINK1/PSTI
polymorphisms act as disease modifiers in familial and idiopathic chronic
pancreatitis. Gastroenterology 2000; 119: 615-23. [PMID: 10982753]
- Mounzer R, Whitcomb DC. Genetics of acute and chronic pancreatitis.
Current opinion in gastroenterology 2013; 29: 544-51. [PMID: 23872486]
- Chowdhury SD, Chacko A, Ramakrishna BS, et al. Clinical profile and
outcome of chronic pancreatitis in children. Indian pediatrics 2013; 50:
1016-9. [PMID: 23798627]
- Malka D, Hammel P, Sauvanet A, et al. Risk factors for diabetes
mellitus in chronic pancreatitis. Gastroenterology 2000; 119: 1324-32. [PMID: 11054391]
- Poulsen JL, Olesen SS, Malver LP, Frokjaer JB, Drewes AM. Pain and
chronic pancreatitis: a complex interplay of multiple mechanisms. World
journal of gastroenterology : WJG 2013;19:7282-91.
- Rosch T, Daniel S, Scholz M, et al. Endoscopic treatment of chronic
pancreatitis: a multicenter study of 1000 patients with long-term followup.
Endoscopy 2002; 34: 765-71. [PMID: 12244496]
- Gress F, Schmitt C, Sherman S, Ciaccia D, Ikenberry S, Lehman
G. Endoscopic ultrasound-guided celiac plexus block for managing
abdominal pain associated with chronic pancreatitis: a prospective single
center experience. The American journal of gastroenterology 2001; 96:
409-16. [PMID: 11232683]
- Parsi MA, Stevens T, Lopez R, Vargo JJ. Extracorporeal shock wave
lithotripsy for prevention of recurrent pancreatitis caused by obstructive
pancreatic stones. Pancreas 2010; 39: 153-5. [PMID: 19820418]
- Duval MK, Jr. Caudal pancreatico-jejunostomy for chronic relapsing
pancreatitis. Annals of surgery 1954; 140: 775-85. [PMC: 1609706]
- Puestow CB, Gillesby WJ. Retrograde surgical drainage of pancreas
for chronic relapsing pancreatitis. AMA archives of surgery 1958; 76:
898-907. [PMID: 13532132]
- O'Neil SJ, Aranha GV. Lateral pancreaticojejunostomy for chronic
pancreatitis. World journal of surgery 2003; 27: 1196-202. [PMID:
14534819]
- Partington PF, Rochelle RE. Modified Puestow procedure for
retrograde drainage of the pancreatic duct. Annals of surgery 1960; 152:
1037-43. [ PMC: 1613865]
- Forsmark CE. Management of chronic pancreatitis. Gastroenterology
2013; 144: 1282-91 e3. [PMID: 23622138]
- Beger HG, Krautzberger W, Bittner R, Buchler M, Limmer J.
Duodenum-preserving resection of the head of the pancreas in patients
with severe chronic pancreatitis. Surgery 1985; 97: 467-73. [PMID:
3983823]
- Frey CF, Smith GJ. Description and rationale of a new operation for
chronic pancreatitis. Pancreas 1987; 2: 701-7. [PMID: 3438308]
- Whipple AO. Radical Surgery for Certain Cases of Pancreatic Fibrosis
associated with Calcareous Deposits. Annals of surgery 1946; 124: 991-
1006. [PMID: 17858905]
- Prochorov AV, Oldhafer KJ, Tretyak SI, et al. Surgical treatment of pain
in patients with chronic
pancreatitis. Hepato-gastroenterology 2012; 59: 1265-9. [PMID:
22580679]
- Keck T, Adam U, Makowiec F, et al. Short- and long-term results of
duodenum preservation versus resection for the management of chronic
pancreatitis: a prospective, randomized study. Surgery 2012; 152:
S95-S102. [PMID: 22906892]
- Bachmann K, Tomkoetter L, Kutup A, et al. Is the Whipple procedure
harmful for long-term outcome in treatment of chronic pancreatitis?
15-years follow-up comparing the outcome after pyloruspreserving pancreatoduodenectomy and Frey procedure in chronic pancreatitis.
Annals of surgery 2013; 258: 815-20; discussion 20-1. [PMID: 24096767]
- Najarian JS, Sutherland DE, Matas AJ, Goetz FC. Human islet
autotransplantation following pancreatectomy. Transplantation
proceedings 1979; 11: 336-40. [PMID: 109963]
- Traverso LW, Kozarek RA. Pancreatoduodenectomy for chronic
pancreatitis: anatomic selection criteria and subsequent long-term
outcome analysis. Annals of surgery 1997; 226: 429-35; discussion 35-8. [PMID: 9351711]
- Gall FP, Muhe E, Gebhardt C. Results of partial and total
pancreaticoduodenectomy in 117 patients with chronic pancreatitis.
World journal of surgery 1981; 5: 269-75. [PMID: 7245796]
- Murphy MM, Knaus WJ, 2nd, Ng SC, et al. Total pancreatectomy: a
national study. HPB : the official journal of the International Hepato
Pancreato Biliary Association 2009; 11:476-82. [PMC: 2756634]
- Nathan H, Wolfgang CL, Edil BH, et al. Peri-operative mortality and
long-term survival after total
pancreatectomy for pancreatic adenocarcinoma: a population-based
perspective. Journal of surgical oncology 2009; 99: 87-92. [PMID:
19021191]
- Stauffer JA, Nguyen JH, Heckman MG, et al. Patient outcomes after
total pancreatectomy: a single centre contemporary experience. HPB : the
official journal of the International Hepato Pancreato Biliary Association
2009; 11: 483-92. [PMID: 19816612]
- Casadei R, Monari F, Buscemi S, et al. Total pancreatectomy: indications,
operative technique, and results: a single centre experience and review of
literature. Updates in surgery 2010; 62:41-6. [PMID: 20845100]
- Crippa S, Tamburrino D, Partelli S, et al. Total pancreatectomy:
indications, different timing, and perioperative and long-term outcomes.
Surgery 2011;149:79-86. [PMID: 20494386]
- Jamil LH, Chindris AM, Gill KR, et al. Glycemic control after total
pancreatectomy for intraductal papillary mucinous neoplasm: an
exploratory study. HPB surgery : a world journal of hepatic, pancreatic
and biliary surgery 2012; 2012: 381328. [PMID: 22966212]
- Bellin MD, Freeman ML, Gelrud A, et al. Total pancreatectomy and
islet autotransplantation in chronic pancreatitis: Recommendations
from PancreasFest. Pancreatology : official journal of theInternational
Association of Pancreatology 2014; 14: 27-35.
- Dunderdale J, McAuliffe JC, McNeal SF, et al. Should pancreatectomy
with islet cell autotransplantation in patients with chronic alcoholic
pancreatitis be abandoned? Journal of the American College of Surgeons
2013; 216: 591-6. [PMID: 23521936]
- Takita M, Itoh T, Matsumoto S, et al. Autoimmune chronic pancreatitis
with IgG4-related pancreatic pseudocyst in a patient undergoing total
pancreatectomy followed by autologous islet transplantation: a case
report. Pancreas 2013; 42: 175-7. [PMID: 23254915]
- Lee BW, Jee JH, Heo JS, et al. The favorable outcome of human islet
transplantation in Korea: experiences of 10 autologous transplantations.
Transplantation 2005;79:1568-74. [PMID: 15940047]
- Balzano G, Carvello M, Piemonti L, et al. Combined laparoscopic
spleen-preserving distal pancreatectomy and islet autotransplantation
for benign pancreatic neoplasm. World journal of gastroenterology : WJG
2014; 20: 4030-6. [PMID: 24744593]
- Iyegha UP, Asghar JA, Beilman GJ. Total pancreatectomy and islet
auto-transplantation as treatment for ampullary adenocarcinoma in the
setting of pancreatic ductal disruption secondary to acute necrotizing
pancreatitis. A case report. JOP : Journal of the pancreas 2012; 13: 239-
42. [PMID: 22406611]
- Garraway NR, Dean S, Buczkowski A, et al. Islet autotransplantation
after distal pancreatectomy for pancreatic trauma. J Trauma 2009; 67:
E187-9. [PMID: 20009652]
- Jindal RM, Ricordi C, Shriver CD. Autologous pancreatic islet
transplantation for severe trauma. The New England journal of medicine
2010; 362: 1550. [PMID: 20410526]
- Balzano G, Maffi P, Nano R, et al. Extending indications for islet
autotransplantation in pancreatic surgery. Annals of surgery 2013; 258:
210-8. [PMID: 23751451]
- Kobayashi T, Manivel JC, Bellin MD, et al. Correlation of pancreatic
histopathologic findings and islet yield in children with chronic pancreatitis
undergoing total pancreatectomy and islet autotransplantation. Pancreas
2010; 39: 57-63. [PMID: 19745778]
- Chinnakotla S, Bellin MD, Schwarzenberg SJ, et al. Total
Pancreatectomy and Islet Autotransplantation in Children for Chronic
Pancreatitis: Indication, Surgical Techniques, Postoperative Management,
and Long-term Outcomes. Annals of surgery 2014. [PMID: 24509206]
- Khan KM, Desai CS, Kalb B, et al. MRI prediction of islet yield for
autologous transplantation after total pancreatectomy for chronic
pancreatitis. Digestive diseases and sciences 2013; 58: 1116-24. [PMID:
23086123]
- Choi SH, Hwang HK, Kang CM, Yoon CI, Lee WJ. Pylorus- and spleenpreserving
total pancreatoduodenectomy with resection of both whole
splenic vessels: feasibility and laparoscopic application to intraductal
papillary mucin-producing tumors of the pancreas. Surgical endoscopy
2012; 26: 2072-7. [PMID: 22237756]
- Dokmak S, Aussilhou B, Sauvanet A, Ruszniewski P, Levy P, Belghiti J.
Hand-assisted laparoscopic total pancreatectomy: a report of two cases.
Journal of laparoendoscopic & advanced surgical techniques Part A 2013;
23: 539-44. [PMID: 23551033]
- Galvani CA, Rodriguez Rilo H, Samame J, Porubsky M, Rana A,
Gruessner RW. Fully robotic-assisted technique for total pancreatectomy
with an autologous islet transplant in chronic pancreatitis patients:
results of a first series. Journal of the American College of Surgeons 2014;
218: e73-8. [PMID: 24559970]
- Zureikat AH, Nguyen T, Boone BA, et al. Robotic total pancreatectomy
with or without autologous islet cell transplantation: replication of an
open technique through a minimal access approach. Surgical endoscopy
2014. [PMID: 25005012]
- Desai CS, Stephenson DA, Khan KM, et al. Novel technique of
total pancreatectomy before autologous islet transplants in chronic
pancreatitis patients. Journal of the American College of Surgeons 2011;
213: e29-34. [PMID: 21996486]
- Chinnakotla S, Radosevich DM, Dunn TB, et al. Long-term outcomes
of total pancreatectomy and islet auto transplantation for hereditary/
genetic pancreatitis. Journal of the American College of Surgeons 2014;
218: 530-43. [PMID: 24655839]
- Wilson GC, Sutton JM, Salehi M, et al. Surgical outcomes after total
pancreatectomy and islet cell autotransplantation in pediatric patients.
Surgery 2013; 154: 777-83; discussion 83-4. [PMID: 24074415]
- Scharp DW, Lacy PE, Santiago JV, et al. Insulin independence after
islet transplantation into type I diabetic patient. Diabetes 1990; 39: 515-
8. [PMID: 2108071]
- Maffi P, Balzano G, Ponzoni M, et al. Autologous pancreatic islet
transplantation in human bone marrow. Diabetes 2013;62:3523-31. [PMID: 23733196]
- Kawahara T, Kin T, Shapiro AM. A comparison of islet
autotransplantation with allotransplantation and factors elevating acute
portal pressure in clinical islet transplantation. Journal of hepato-biliarypancreatic
sciences 2012;19:281-8. [PMID: 21879320]
- Wilhelm JJ, Bellin MD, Dunn TB, et al. Proposed thresholds for
pancreatic tissue volume for safe intraportal islet autotransplantation
after total pancreatectomy. American journal of transplantation : official
journal of the American Society of Transplantation and the American
Society of Transplant Surgeons 2013;13:3183-91. [PMID: 24148548]
- Desai CS, Khan KM, Megawa FB, et al. Influence of liver histopathology
on transaminitis following total pancreatectomy and autologous islet
transplantation. Digestive diseases and sciences 2013; 58: 1349-54. [PMID: 22688185]
- Cantarelli E, Piemonti L. Alternative transplantation sites for
pancreatic islet grafts. Current diabetes reports 2011; 11: 364-74. [PMID:
21789599]
- Sutherland DE, Radosevich DM, Bellin MD, et al. Total pancreatectomy
and islet autotransplantation for chronic pancreatitis. Journal of the
American College of Surgeons 2012; 214: 409-24; discussion 24-6. [PMID:
22397977]
- Bramis K, Gordon-Weeks AN, Friend PJ, et al. Systematic review
of total pancreatectomy and islet autotransplantation for chronic
pancreatitis. The British journal of surgery 2012; 99: 761-6. [PMID:
22434330]
- Walsh RM, Saavedra JR, Lentz G, et al. Improved quality of life
following total pancreatectomy and auto-islet transplantation for chronic
pancreatitis. Journal of gastrointestinal surgery : official journal of the
Society for Surgery of the Alimentary Tract 2012; 16: 1469-77. [PMID:
22673773]
- Dorlon M, Owczarski S, Wang H, Adams D, Morgan K. Increase in
postoperative insulin requirements does not lead to decreased quality
of life after total pancreatectomy with islet cell autotransplantation for
chronic pancreatitis. The American surgeon 2013; 79: 676-80. [PMID:
23815999]
- Garcea G, Pollard CA, Illouz S, Webb M, Metcalfe MS, Dennison AR.
Patient satisfaction and cost-effectiveness following total pancreatectomy
with islet cell transplantation for chronic pancreatitis. Pancreas 2013; 42:
322-8. [PMID: 23407482]
- Ahmad SA, Lowy AM, Wray CJ, et al. Factors associated with insulin
and narcotic independence after islet autotransplantation in patients with
severe chronic pancreatitis. Journal of the American College of Surgeons
2005; 201: 680-7. [PMID: 16256909]
- Kuesters S, Karcz WK, Hopt UT, Keck T. [Laparoscopically assisted
total pancreatectomy : Feasible minimally invasive alternative to open
resection.]. Der Chirurg; Zeitschrift fur alle Gebiete der operativen
Medizen 2014. [PMID: 24824001]
- Kim DH, Kang CM, Lee WJ. Laparoscopic-assisted spleen-preserving
and pylorus-preserving total pancreatectomy for main duct type
intraductal papillary mucinous tumors of the pancreas: a case report.
Surgical laparoscopy, endoscopy & percutaneous techniques 2011; 21:
e179-82. [PMID: 21857455]
- Kitasato A, Tajima Y, Kuroki T, Adachi T, Kanematsu T. Hand-assisted
laparoscopic total pancreatectomy for a main duct intraductal papillary
mucinous neoplasm of the pancreas. Surgery today 2011; 41: 306-10. [PMID: 21264776]
- Casadei R, Marchegiani G, Laterza M, et al. Total pancreatectomy:
doing it with a mini-invasive approach. JOP : Journal of the pancreas 2009;
10: 328-31. [PMID: 19454829]
- Dallemagne B, de Oliveira AT, Lacerda CF, D'Agostino J, Mercoli H,
Marescaux J. Full laparoscopic total pancreatectomy with and without
spleen and pylorus preservation: a feasibility report. Journal of hepatobiliary-
pancreatic sciences 2013. [PMID: 23430055]
- Daouadi M, Zureikat AH, Zenati MS, et al. Robot-assisted minimally
invasive distal pancreatectomy is superior to the laparoscopic technique.
Annals of surgery 2013; 257: 128-32. [PMID: 22868357]
- Bhayani NH, Enomoto LM, Miller JL, et al. Morbidity of total
pancreatectomy with islet cell auto-transplantation compared to total
pancreatectomy alone. HPB : the official journal of the International
Hepato Pancreato Biliary Association 2014; 16: 522-7.
- Garcea G, Weaver J, Phillips J, et al. Total pancreatectomy with and
without islet cell transplantation for chronic pancreatitis: a series of 85
consecutive patients. Pancreas 2009; 38: 1-7. [PMID: 18665009]
- Argo JL, Contreras JL, Wesley MM, Christein JD. Pancreatic resection
with islet cell autotransplant for the treatment of severe chronic pancreatitis.
The American surgeon 2008;74:530-6; discussion 6-7. [PMID: 18556996]
- Morgan K, Owczarski SM, Borckardt J, Madan A, Nishimura M,
Adams DB. Pain control and quality of life after pancreatectomy with islet
autotransplantation for chronic pancreatitis. J Gastrointest Surg. 2012;
16:129- 33; discussion 133-4. [PMID: 22042566]


