Kakou Charles1*, Kasse Raoul1, Garba Idrissa2, Gondo Diomande1 and Boni Serge1
1Department of Obstetrics and Gynecology, UH-C (Cocody University Hospital), Abidjan, Côte d’Ivoire, Ivory Coast
2Department of Radiology, UH-Y (Yopougon University Hospital), Abidjan, Côte d’Ivoire, Ivory Coast
*Corresponding Author:
Kakou Charles
Department of Obstetrics and Gynecology
Cocody University Hospital (UH-C)
06 Po Box 296 Abidjan 06
Côte d’Ivoire
Ivory Coast
Tel: 00 (225) 22 48 10 50
Fax: 00 (225) 22 44 23 79
E-mail: kakoucharles@yahoo.fr
Received date: July 10, 2017; Accepted date: October 10, 2017; Published date: October 13, 2017
Citation: Charles K, Raoul K, Idrissa G, Diomande G, Serge B (2017) Torsion of Uterine Fibroid: A Rare Cause of Acute Pelvic Pain: About One Case. Gynecol Obstet Case Rep Vol.3: No.3: 56.
Keywords
Uterine fibroid; Complications; Torsion; Surgery
Introduction
Uterine fibroids represent the most common benign tumors of the uterus. They are most often asymptomatic [1]. Uterine fibroids can become complicated and to become a real gynecological emergency outside classic emergencies bleeding [2]. The torsion of a pediculated subserosal uterine fibroid is a rare complication that should be diagnosed otherwise it can progress to other more serious complications [3,4]. We report one case about torsion of pediculated subserosal fibroid diagnosed in a context of pelvic mass painful acute.
Clinical Presentation
Madam Y.S.O., 34-year-old, housewife, has been received at gynecological emergencies of Cocody University Hospital (Abidjan) in June 2016 for pelvic pain of sudden occurrence of strong intensity, radiating in the pelvis causing a stir and with nausea. There was no vomiting nor stop materials and gases. There was no bleeding and urinary symptom. Menstruations were back ten days before. In the medical history, the patient was not a chronic medical condition known. She had never been previously operated. She had a gestity to 4 and four deliveries. The patient was carrying a known non-symptomatic uterine fibroid five year before these four deliveries. The clinical examination in the emergency room was a normal condition with constant hemodynamic normal. Palpation of the abdomen, there was a mass suprapubic and under umbilical mobile median of firm and painful consistency that can measured about 15 cm. The cervix and vaginal walls were of normal appearance to the speculum. Vaginal touch included an increased uterus size and whose movements were transmitted to the suprapubic mass. There is no palpable latero-uterine mass. A urinary pregnancy test conducted immediately at the end of our clinical examination was negative. A pelvic ultrasound through the suprapubic had highlighted an echogenic image rounded fundic subserosal to depend of the uterus without signs of necrobiosis measuring 133 mm × 100 mm (Figures 1 and 2) in relation of a pediculated mass. The uterus was empty (Figure 3). Ovaries were normal. There is no pelvic effusion. A plasmatic dosage of Bhcg was negative. Diagnosis of pediculated subserosal uterine fibroid in torsion has been chosen. An emergency laparotomy was performed. Per-operative, was actually of a pediculated subserosal fibroids in torsion (Figures 4 and 5). We realized a section at the base of the peduncle of the fibroid with a suture with absorbable gauge wire n°0. The postoperative were simple with returning home to the patient on the 3rd day postsurgery. The histological exam confirmed that it was a leiomyoma.
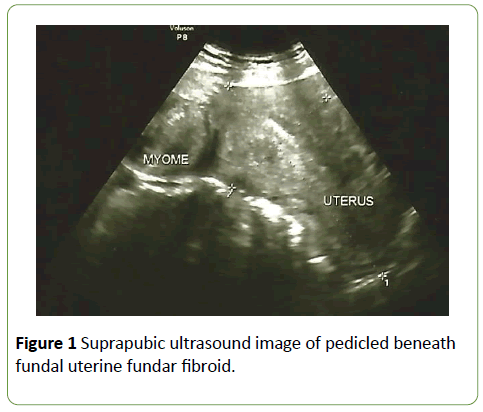
Figure 1: Suprapubic ultrasound image of pedicled beneath fundal uterine fundar fibroid.
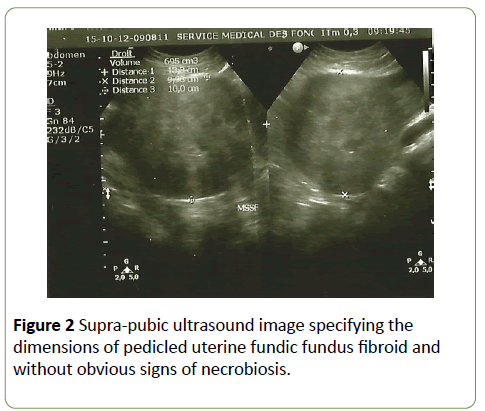
Figure 2: Supra-pubic ultrasound image specifying the dimensions of pedicled uterine fundic fundus fibroid and without obvious signs of necrobiosis.
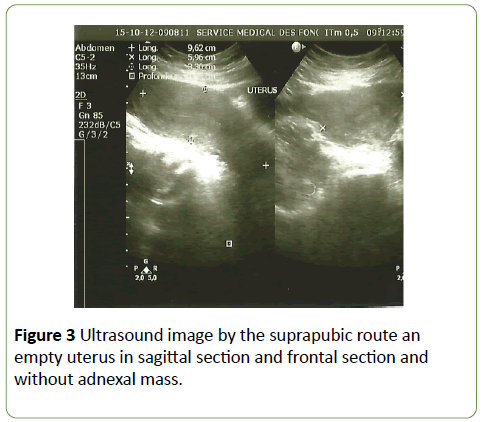
Figure 3: Ultrasound image by the suprapubic route an empty uterus in sagittal section and frontal section and without adnexal mass.
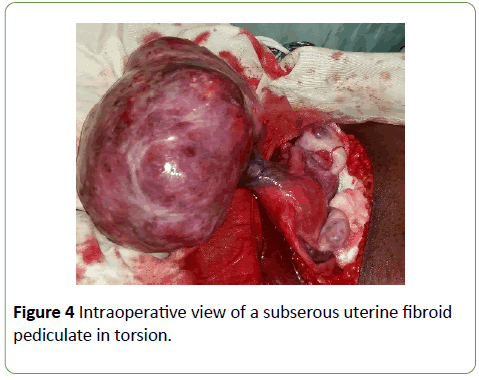
Figure 4: Intraoperative view of a subserous uterine fibroid pediculate in torsion.
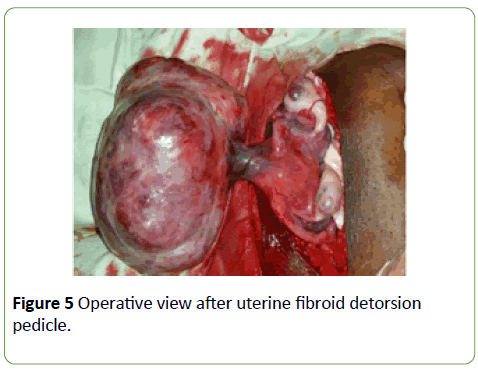
Figure 5: Operative view after uterine fibroid detorsion pedicle.
Discussion
The uterine fibroid is a frequent pathology in women of reproductive age. It is about 20% of women over the age of 35 years [4,5]. It is a more frequent pathology in the black race than in the white race [6]. Fibroids are often multiple in 70% and seat yet in more than 90% [7,8]. The torsion of pediculated subserosal fibroid is exceptional compared to the ovary’s torsion [9]. In the literature, there is no an estimated frequency of the torsion of fibroid because it’s an event of exceptional occurrence or an undiagnosed complication. But some described cases of uterine fibroid in twisting are the most observed during pregnancy, especially in the first trimester of pregnancy [2,10,11]. There are risk factors of torsion of pediculated fibroid: mentioned are: the weight of the fibroid, the length of the pedicle, the softening of the fibroid during pregnancy [3,11]. In addition, pediculated fibroid being free in the peritoneal cavity, the peristalsis of the digestive handles could participate to the torsion [12].
Uterine fibroids are often asymptomatic [1]. In the case of protest, the symptoms vary depending on the fibroid’s localization. Classically, the fibroid is not painful. In case of pain, it’s important to look for a complication of the fibroid: necrobiosis, torsion, cervical birth a pediculated perfect fibroid or degeneration [5]. In the case of torsion of pediculated subserosal fibroid, the clinical picture is noisy and brutal appearance.
It is pelvic pain intolerable, violent because original ischemic and resistant to pain, accompanied by nausea, vomiting, bloating. Abdominal palpation is very painful with a defense against torsion [5]. It's a gynecological emergency. Total clinical signs reflecting the torsion of pediculated fibroid are those of an acute abdominal pain syndrome. In our clinical case, symptoms were in relation to the signs described in the literature. The diagnosis of torsion is essentially clinical [10].
Medical history can help guide diagnosis especially when there is a notion of fibroid pre-existing in the patient. Pelvic ultrasonography, diagnostic test of reference [13] for uterine fibroids, helps to clarify the fibroid aspect of the pelvic mass. But she shows no direct signs of torsion. On the other hand, it eliminates other possible diagnoses: aseptic necrobiosis, torsion of ovarian cyst or annex, ectopic pregnancy. In addition, ultrasound precises number, seat and size of fibroids.
Another method of imaging like pelvic MRI can help diagnosis, in some cases, by visualizing the pedicle of subserosal fibroid [14]. The diagnosis of torsion is essentially clinical. Confirmation is per-operative. In our developing countries, we have not usually access to the MRI because it’s too cost, and it isn’t always availability in our hospitals. So, clinical examination and pelvic ultrasound take up the first place of investigations. They are in first the diagnostic tools. The accuracy of diagnosis is capital and the management should be immediate for several reasons. It is an emergency because of acute abdominal syndrome with acute pain, often a defense and a state of shock. The torsion of pediculated subserosal fibroid is already a complication, but it can be more complicated. The complications found in the literature are a volvulus of the small intestine [12,13]; an auto-amputation of the fibroid realizing a foreign body responsible for peritonitis [3]. Once the diagnosis is established, support is essentially surgical and is made in an emergency. It consists of a myomectomy. It will be conventionally performed by laparotomy or laparoscopy in case of less than 10 cm fibroid and/or few, less than 3 fibroids [15]. A hysterectomy may be offered in a woman who is close to menopause and who want not children. Moreover, when the torsion of pediculated subserosal uterine fibroid occurs in the first trimester of pregnancy, myomectomy is possible with a good prognosis [2].
Conclusion
The torsion of uterine fibroid is a rare complication which deserves to be diagnosed because of its evolution towards other more serious complications. The diagnosis is clinical. Our clinical case shows the interest of clinical examination in the diagnosis of this complication of uterine fibroids due to poor access to technologies of imaging such scanner and MRI and their low contribution to the diagnosis.
Conflict of Interest
The authors declare non-conflict of interest.
References
- Sparic R, Mirkovic L, Malvasi A, Tinelli A (2016) Epidemiology of uterine myomas: A review. Int J Fertil Steril 9: 424-435.
- Kosmidis C, Pantos G, Efthimiadis C, Gkoutziomitrou I, Georgakoudi E, et al. (2015) Laparoscopic excision of a pedunculated uterine leiomyoma in torsion as a cause of acute abdomen at 10 weeks of pregnancy. Am J Case Rep 16: 505-508.
- Suganuma I, Mori T, Takahara T, Torii H, Fujishiro M, et al. (2015) Autoamputation of a pedunculated, subserosal uterine leiomyoma presenting as a giant peritoneal loose body. Arch Gynecol Obstet 291: 951-953.
- Sparic R (2014) Uterine myomas in pregnancy, childbirth and the puerperium. Srp Arh Celok Lek 142: 118-124.
- Courbiere B, Carcopino X (2009) Uterine fibroids. In: Courbiere B, Carcopino X (eds). Gynécologie-obstétrique. New edition 2009, Paris, Editions Vernazobres-Grego. pp. 439-447.
- Othman EE, Al-Hendy A (2008) Molecular genetics and racial disparities of uterine leiomyomas. Best Pract Res Clin Obstet Gynaecol 22: 589-601.
- Cramer SF, Patel A (1990) The frequency of uterine leiomyomas. Am J Clin Pathol 94: 435-438.
- The Society of Obstetricians and Gynaecologists of Canada (2015) The SOGC guideline. Support for uterine leiomyomas. J Obstet Gynaecol Can 37: 179-181
- Brun G, Brun JL (1998) Benign tumors of the uterus. In: Hédon B, Madélenat P, Dargent D, Frydman R (eds). Gynaecology. Paris, Ellipses. pp. 111-119.
- Currie A, Bradley E, McEwen M, Al-Shabibi N, Willson PD (2013) Laparoscopic approach to fibroid torsion presenting as an acute abdomen in pregnancy. JSLS 17: 665-667.
- Nigam A, Raghunandan C, Yadav R (2014) Twisted subserosal leiomyoma in a non-gravid uterus: A rare cause of acute abdomen. J Obstet Gynaecol 34: 657-658.
- Guglielmo N, Malgras B, Place V, Guerrache Y, Pautrat K, et al. (2016) Small bowel volvulus due to torsion of pedunculated uterine leiomyoma: CT findings. Clin Imaging 28: 11-13.
- Downes E, Sikirica V, Gilabert-Estelles J, Bolge SC, Dodd SL, et al (2010) The burden of uterine fibroids in five European countries. Eur J Obstet Gynecol Reprod Biol 152: 96-102.
- Shingo M, Takashi M, Yoshimitsu O, Tetsuya I, Miki M, et al. (2016) The relationship between torsion and of the length of the peduncle in patients with uterine subserosal leiomyoma. J Minim Invasive Gynecol 5 : 74-77.
- Dubuisson JB, O'Leary T, Feki A, Bouquet DE Jolinière J, et al. (2016) Laparoscopic myomectomy. Minerva Ginecol 68: 345-351.

