Natália Noronha*, Maria Emanuel Amaral, Helena Andrade, António Pires, António Marinho, and Eduardo Castela
Department of Pediatric Cardiology, CHUC Coimbra, Portugal
*Corresponding Author:
Natália Noronha
Department of Pediatric Cardiology, CHUC Coimbra, Portugal.
Tel: 239 800 100
Fax: 239 717 216
E-mail: natalianoronhaf@gmail.com
Received Date: May 23, 2017; Accepted Date: June 07, 2017; Published Date: June 14, 2017
Citation: Noronha N, Amaral ME, Andrade H, et al. There is more to Wolff-Parkinson- White than meets the Eye. Interv Cardiol J 2017, 3:2. DOI: 10.21767/2471-8157.100056
Keywords
Wolff-Parkinson-White syndrome; Supraventricular tachycardia; Wide complex tachycardia; Narrow complex tachycardia
Case Report
Supraventricular tachycardia (SVT) is the most common dysrhythmia in the paediatric population [1]. Clinical manifestations usually vary according to the patient’s age, haemodynamic status and ability to recognize and communicate symptoms.
A previously healthy 9-month-old infant was admitted to the emergency department with a bronchiolitis. On admission, his heart rate was 300 bpm, with no previous medication having been administered. but he was haemodynamically stable and the electrocardiogram (ECG) showed a wide complex tachycardia (Figure 1-upper panel], with a cycle length of 200 ms. He failed to respond to vagal manoeuvres and adenosine and was transferred to our centre.
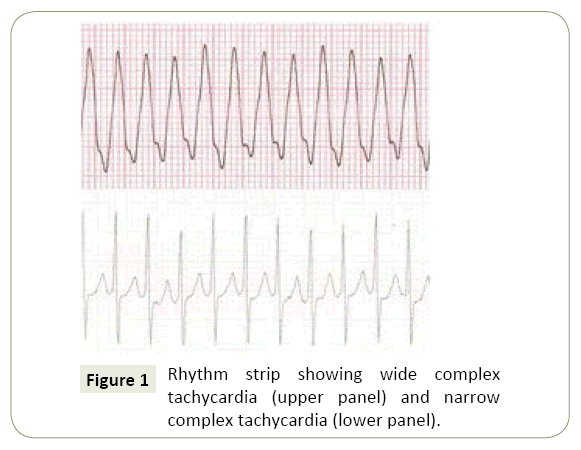
Figure 1: Rhythm strip showing wide complex tachycardia (upper panel) and narrow complex tachycardia (lower panel).
During transfer, he reverted spontaneously to sinus rhythm. On admission he was irritable, with heart rate of 150 bpm. The 12-lead surface ECG revealed sinus rhythm, a short PR, a wide QRS interval with a delta wave, suggestive of Wolff-Parkinson- White (WPW) pattern (Figure 2). The echocardiogram showed a structurally normal heart with good biventricular function. The laboratory investigation was also normal and he was started on propranolol (0.5 mg/kg/dose 8 hourly). A few hours post admission he developed a narrow complex tachycardia (Figure 1-lower panel] with a cycle length of 230ms, which failed to respond to vagal manoeuvres, adenosine and four electrical cardioversions. Continuous intravenous amiodarone was started and he eventually returned to sinus rhythm. He was later discharged on oral amiodarone and propranolol and is currently in sinus rhythm.
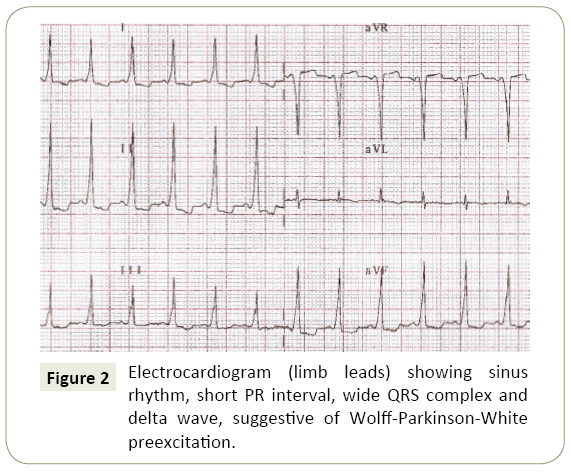
Figure 2: Electrocardiogram (limb leads) showing sinus rhythm, short PR interval, wide QRS complex and delta wave, suggestive of Wolff-Parkinson-White preexcitation.
Discussion
WPW preexcitation is caused by an accessory pathway (AP) that acts as an atrioventricular (AV) bypass. The characteristic ECG findings are attributable to the fusion of the normal sinus QRS complexes and the anterograde conduction via the AP. AV reciprocating tachycardia is not only the most common mechanism of SVT (accounting for approximately 80% of cases) [2], but also the most frequent tachyarrhythmia during childhood [3].
Our case, being rare, highlights the complexity of the underlying mechanisms responsible for concurrent tachyarrhythmias. Patients, such as our infant, with WPW preexcitation are certainly prone to paroxysmal SVT, and most likely of the narrow QRS complex type. In these cases, depolarization occurs down the AV node with retrograde conduction through the AP, leading to narrow QRS complexes (orthodromic re-entrant tachycardia) [4]. More rarely, the AP functions as the anterograde limb and the His-Purkinje system as the retrograde pathway (antidromic re-entrant tachycardia), leading to wide QRS complexes, since the depolarization wave spreads slowly across the ventricles [4]. Another possibility that might explain the two tachyarrhythmia types in our patient is the presence of additional accessory AV pathways. Approximately 10% of patients with WPW preexcitation have two or more AV bypass tracts [2], which may conduct the electrical impulse either anterogradely or retrogradely.
However, as both circuits involve the AV node, we would have expected, as it happens in the majority of cases, the pharmacological and electrical therapy instituted to terminate the dysrhythmia, which it did not.
Other possibilities include nodal AV re-entrant tachycardia and atrial tachycardia. In the former, although very rare in infants and toddlers, the anatomic substrate is a dual pathway within the AV node, with different conduction and recovery rates. These characteristics favour the establishment of a microreentrant circuit, which may allow for either anterograde or retrograde conduction. Atrial tachycardia may occur either due to increased automaticity of myocardial cells [5] in the atrium or to re-entry within the atrial myocardium. It accounts for as high as 15% of cases of SVT in infants and is often refractory to medical treatment [2].
Both nodal AV re-entrant tachycardia and atrial tachycardia result in narrow QRS complexes, as the depolarization wave spreads normally to the ventricles through the His-Purkinje network. This would not explain the wide QRS complex tachycardia presented in our case. A possible justification for the latter could be a functional bundle branch block caused by the rapid heart rates attained in both situations. The AP would only function as a bystander.
A twelve lead ECG during sinus rhythm and during the episodes of tachycardia would be important to help to establish the underlying mechanism. However, as it happened with our case, this is not always possible in the emergency context, particularly in infants.
Conclusion
To clarify the underlying mechanisms, and depending on followup, an electrophysiological study will be needed in the future.
References
- Spearman A, Williams P (2014) Supraventricular tachycardia in infancy and childhood. Pediatr Ann43: 456-460.
- Kantoch M (2005) Supraventricular tachycardia in children. Indian J Pediatr 72: 609-619.
- Park M (2014) Cardiac arrhythmias. Park's pediatric cardiology for practitioners. Philadelphia, (6thedn).Elsevier Saunders 415.
- Brembilla-Perrot B, Pauriah M, Sellal J,Yves Zinzius P, Schwartz J, et al. (2013) Incidence and prognostic significance of spontaneous and inducible antidromic tachycardia. Europace 15: 871-876.
- Brugada J, Blom N, Sarquella BG, Blomstrom-Lundqvist C, Deanfield J, et al. (2013) Pharmacological and non-pharmacological therapy for arrhytmias in the pediatric population. Europace15:1337-1382.

