Keywords
Pancreaticoduodenectomy; Pancreaticojejunostomy;
Pancreatic Fistula
Abbreviations
PD pancreaticoduodenectomy; POPF
postoperative pancreas fistula; TPLD totally laparoscopic
pancreaticoduodenectomy
INTRODUCTION
Total laparoscopic pancreaticoduodenectomy (TLPD)
was first reported in 1994 by Gagner et al. [1]. During
the past two decades, there has been a growing interest
in minimally invasive pancreatic surgery that requires
surgeons with highly experienced laparoscopic skills.
Although minimally invasive approaches have several
advantages including short hospital stay, less scar,
decreased postoperative morbidity, there are only limited
series showing their feasibility and adequacy [2, 3, 4, 5, 6, 7]. Several advantages, including faster recovery period,
short hospital stay and advantageous for adjuvant therapy,
have been showed in comparative series and meta-analysis
[5, 8].
Despite technical advancements, postoperative
complication rate continues to be high. Postoperative
pancreatic fistula/anastomotic leakage (POPF) remains the single most important morbidity after
pancreaticoduodenectomy (PD) with a rate reaching up to
40% [9, 10] and results in prolonged hospitalization and
mortality [11]. Although the type of pancreaticoenteric
anastomosis, external pancreatic duct stenting, use of
perioperative somatostatin were investigated, none has
been found to be effective in decreasing the POPF [11, 12, 13].
There is an adaptation period for TLPD procedure for
the surgeons who perform conventional PD before. The
steep learning curve is of particular concern, because
pancreaticojejunostomy (PJ) anastomosis, which is the
key point of PD, is the most in-demand skill and requires
a sophisticated level of practice. There has been a growing
interest for the use of barbed sutures, predominantly
in urologic procedures within robotic approach
depending on its feasible and practical application
compared to other suture materials [14]. We published
our recent experience in using V-loc suture device
during our modified PJ technique with the promising
outcome considering the fistula rate [9]. In another
report pointing out the difficulties encountered in the
conversion from conventional PD to the TLPD, the
feasibility of our modified PJ anastomosis technique
using V-Loc suture was also mentioned in detail [15].
The aim of the present study was to evaluate the utility
of V-Loc suture device for PJ anastomosis during totally
laparoscopic pancreaticoduodenectomy.
METHODS
Patient Selection
From January 2012 to March 2017, 42 consecutive
cases (25 male and 17 female) underwent TLPD procedure
by the same surgical team including two experienced
hepato-pacreato-biliary surgeons. Informed consent
form was obtained before surgery. The local ethical
committee approved this study with an IRB number of
1249 and the research was conducted in accordance
with the Helsinki Declaration. Exclusion criteria for TLPD
procedure included vascular involvement, previous history
of pancreatic trauma or injury, history of major abdominal
surgery and severe cardiopulmonary morbidity. For initial
case series, small tumor size was preferred. Data collection
was prospectively performed and entered in SPSS by an
assistant secretary.
The outcome measures included operation time,
duration of laparoscopic PJ anastomosis, postoperative
morbidity and mortality rates. The clinical course was
documented for each patient, and the complications were
classified according to the criteria of Clavien and Dindo [16].
POPF rate was also evaluated according to the
international study group on pancreatic fistula (ISGPF)
definition [17]. Pancreatic fistula was diagnosed
when there was measurable drain output on or after
postoperative three days, with amylase content three-fold
greater than the synchronous serum amylase level. Three
different grades of POPF (grade A, B, C) were defined by
ISGPF according to the clinical impact on the patient’s
hospital course. Grade A, also called “transient fistula,”
has no clinical impact. A CT scan typically shows no
peripancreatic collections and the use of total parenteral
nutrition, antibiotics, or somatostatin analogs are not
needed. Grade B is mostly associated with abdominal pain,
fever, and/ or leukocytosis, and antibiotics are usually
required; somatostatin analogs may also be used. A CT scan
may show peripancreatic collections. Grade C is severe, and
always shows a significant change in clinical management
or a deviation from the usual clinical pathway. A CT scan
usually shows worrisome peripancreatic collections that
require percutaneous drainage or re-exploration. Mostly,
there are associated complications such as sepsis and organ
dysfunction, and the possibility of postoperative mortality
rises. And another common postoperative morbidity,
delayed gastric emptying, according to international study
group of pancreatic surgery (Grade A-B-C: nasogastric
requirement in the postoperative period, unable to tolerate
solid orally, vomiting, need for prokinetics).
Suture Material
Following completion of resection procedure (PD),
previously transected jejunum was removed up through
mesentery of transverse colon to the anastomosis
field. Following seromucosal approximation with 6-0
polydioxanone (PDS), three sutures with 5-0 PDS were
located into the Wirsung duct to ensure better exposure. After then, 6-inch length, green 4-0 V-Loc™ 180 barbed
suture material with V20 needle was introduced for
laparoscopic reconstruction. The V-Loc™ absorbable
wound closure device (Covidien Healthcare, Mansfield,
MA) was produced from a copolymer of glycolic acid
and trimethylene carbonate, and consisted of a barbed
absorbable thread armed with a surgical needle at one end
and a loop end effector at the other. The barbed structure
and loop end design allowed for tissue approximation
without the need to tie surgical knots and squeeze the
pancreatic tissue. It was fully absorbed by 180 days.
Surgical Technique
This technique was a laparoscopic modification of
our previously described open PJ procedure [9]. The
patient was placed on a split-leg table and positioned in
reverse Trendelenburg position. The monitor was put on
the patient’s left side toward the head, and the operating
surgeon located between the legs of the patient or on the
right side considering the stages of the procedure. Five
trocars (two 5mm, two 10 mm and one 12 mm) (Figure
1) were used. After pneumoperitoneum, the operation
began with staging laparoscopy. In our previous paper, the
procedure until pancreatic transection was described in
detail [9]. After mobilization of the head of the pancreas,
a tunnel was formed between the posterior aspect of the
neck of the pancreas and the anterior to the superior
mesenteric and portal veins. And pancreatic parenchymal
transection was performed using an endostapler. The
inferior part of remnant pancreas was mobilized 2-3 cm
towards the superior and laterally in preparation for easy
PJ. The dissected segment of the jejunum was brought up
through the dorsal plane of mesentery for reconstruction.
Figure 1: Trocar positioning for laparoscopic pancreaticoduodenectomy (two 5 mm, two 10 mm and one 12 mm).
Firstly, the dorsal part of the jejunal seromuscular
layer and the dorsal part of the capsular parenchyma of
the pancreatic stump were sutured with 4-0 V-Loc suture
in a continuous manner (Figures 2a, b). Following dorsal
external suturing layer, at the second step, a stent was
inserted into the main pancreatic duct and reconstruction
process began with 2-layers end-to-side dunking technique
of PJ. At an approximate length of 2 cm from the closed
stump of the jejunum, a small hole about 5 mm in diameter,
-considering the pancreatic duct diameter- in the jejunum
on the antimesenteric side was created. Then, the dorsal
inner layer was performed with interrupted stitches, 0.5-1
cm apart, using 5-0 polydioxanone (PDS) sutures. Thirdly,
the ventral inner layer was created between the ventral
cut edge of the pancreatic stump, and the ventral jejunal
seromuscular part using 5-0 PDS interrupted sutures (Figures 3a, b). Lastly, the ventral external layer of PJ
was also performed using another 4-0 V-Loc suture device (Figures 4a, b). We placed the sutures 5 -7 mm apart.
Figure 2: (a). V-Loc barbed suture device, (b). external posterior layer of pancreaticojejunostomy.
Figure 3: Dorsal inner layer (a). and ventral inner layer of pancreaticojejunostomy (b). using 5-0 polydioxanone.
Figure 4: (a, b). External dorsal layer of pancreaticojejunostomy.
Internal pancreatic ductal stenting using 6 or 8
Fr PVC stent was routinely used without securing.
The reconstruction was continued with end-to-side
hepaticojejunostomy (HJ), and completed with an end-toside
gastrojejunostomy. The specimen was extracted into an endobag through the extended infraumbilical trocar
site. Two Jackson-Pratt drains were placed near the PJ and
HJ anastomosis.
Drains remained in place for at least 5 days after
surgery, and the volumes and the amylase concentration
of the drainage were recorded. Drains were removed
regarding the volume and structure of the drainage fluid,
and also amylase concentration. After discharge, patients
were recommended to visit surgical outpatient department
on the postoperative day 7, then every 3–6 months for
surveillance of tumor recurrence distinct from the course
of adjuvant management.
Statistical Analysis
IBM SPSS version 20 (IBM, Chicago) was utilized
for analysis. There were only descriptive measures.
Continuous variables were represented as mean±standard
deviation or median and range. Categorical variables were
expressed as percentages.
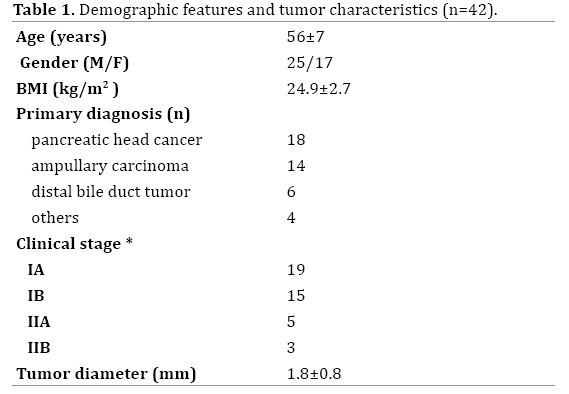
RESULTS
Demographic features and the underlying diseases
are shown in Table 1. The mean operating time was
339±43 min (range: 280-415 min), and the mean time
of PJ anastomosis was 36±4.8 (range: 30-46 min). Mean
diameter of pancreatic duct was 3.5±1.2 mm (range: 3-6
mm). Mean length of hospital stay was 8.1±4 day (range:
6-34 days). Detailed surgical and postoperative data are
shown in Table 2.
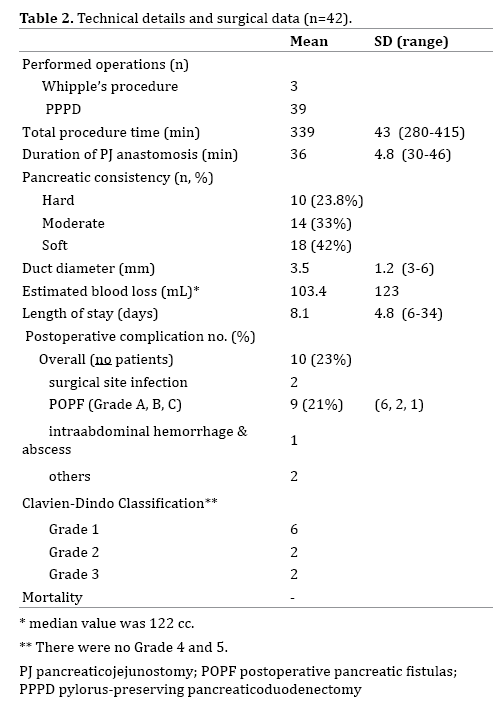
Ten (23%) patients had 15 complications and POPF
was observed in nine patients (21%): Grade A in 6,
Grade B in 2 and Grade C in 1 (Table 2). One patient with
Grade C fistula underwent emergent reoperation due to
intraabdominal abscess and subsequent hemorrhage. The
recovery period was uneventful after then. One patient with HJ stricture underwent revision surgery, and reanastomosis
was laparoscopically performed. One patient
required percutaneous drainage catheter placement
due to intraabdominal collection secondary to the POPF.
The remaining complications including delayed gastric
emptying (n=8, 19%) were managed conservatively. Most
of them (n=5) were Grade A and no patients with Grade C
were observed. There was no postoperative mortality.
DISCUSSION
Technological advances and rising availability of
featured materials provide better intraoperative scores
and postoperative recovery period. However, details of
surgical technique remain a debate resulting in roughly
similar POPF rate. In the light of this study of prospectively
collected data, we suggest that the use of V-Loc suture
during TLPD might be reasonable concerning with
comparable results with previous series, Additionally, the
V-Loc suture device can be beneficial for tissue protection
avoiding tightening the pancreas after every suture bite
and time-saving without need for a knot-tying.
Although minimally invasive techniques have often
replaced open surgery in many abdominal surgical procedures, regarding hepato-pancreato-biliary surgery,
few centers have adopted minimally invasive PD due to the
complexity of the procedure and technical difficulties. PJ
anastomosis is the key point in pancreatic cancer surgery.
The probability of POPF after open surgery is between
5% and 40% [9, 10]. Several studies noted enhanced
recovery period and significantly lower complication
rates in minimally invasive PD [4, 5, 18, 19], whereas
some authors reported higher or similar rate of POPF in
minimally invasive approach compared to open [11, 20].
Likewise to latter group, a very recent meta-analysis
of nonrandomized comparative studies demonstrated
some worrisome results for the laparoscopic approach in terms of morbidity, especially when considering TLPD
[21]. This could be attributed to the fact that most of the
studies included are based on their initial experience. Thus,
later reports probably reveal better outcomes as the surgeons
overcome the learning curve.
The two-layer, end-to-side, duct-to-mucosa PJ was the
most commonly used pancreatic anastomosis approach, as we
also perform in our center, however, there is still no clear
consensus defining 100% safe technique of pancreaticenteric
anastomosis. At least ten various methods are
available to prevent POPF [19]. In a very recent report
by ISGPS, the risks for anastomotic complications have
been mostly based on gland factors, such as texture and
disease pathology. No technical variations have been
found superior to another [22]. In our previous study,
V-Loc knotless wound closure device used in external
anastomoses of open pancreaticoduodenectomy was
found advantageous and secure especially concerning soft
pancreatic texture [9]. Apart from the short-term outcomes
such as POPF, considering stenosis of the main pancreatic
duct at the PJ anastomosis, that is one of the postoperative
complications after such dunking technique, our results
(2.3%) were also satisfying.
The barbed type suture was initially described for
tendon repair to decrease the need for the knot and
increase gripping strength between tissues. The barbed
polyglyconate suture was first used for the UVA during
robot-assisted radical prostatectomy beginning in 2010
[23]; safety and feasibility were previously demonstrated
in several studies [24]. Application of the V-LocTM suture
(Covidien, Mansfield, MA) in pancreaticojejunostomy
formation may offer some advantages over conventional
suture types. The V-Loc suture maintains excellent
hemostasis and minimal tissue damage which is a major
issue especially in patients with soft pancreas quality,
provides by no need for repeated suture tightening and
tissue traction after each needle passage. Moreover, barbs
prevent suture slippage and distribute forces; therefore,
tearing and plausible ischemic changes in the suture line
are avoided.
The barbed suture technique is easy to perform which
is of benefit to the surgeon during the transition period
from conventional to laparoscopic or robotic PD and
results in less operative time [25, 27, 28]. Most of the
series using barbed sutures reported significantly shorter
reconstruction time regarding V-loc suture usage for
anastomosis. Tewari and colleagues recently published a
retrospective comparative series -V-Loc vs. conventional
suture- and noted significantly shorter total reconstruction
times in V-Loc group (8 vs. 13.5 min; p<0.001) [25]. In a
systematic review and meta-analysis investigating the
efficacy and safety of knotless barbed sutures, both suture
and operative time were found significantly reduced, and
no increase was recorded with regard to the postoperative
complication related to the suture material [27]. In this
study, there was no comparison group laparoscopically.
Comparative analysis of V-loc and conventional techniques for laparoscopic PD, Edil et al. reported less operative time
with similar postoperative morbidity [28]. Our results were
remarkable when compared other laparoscopic PD series.
Because duration of PJ has not been routinely evaluated, it
is not possible to note that PJ time is comparable.
The pancreatic texture is defined using surgeon-based
experience and known to be one of the most important
factors predicting the safety of anastomosis. Soft pancreas
has been the most challenging type to create secure PJ
avoiding POPF [29, 30, 31]. In the present study, during
laparoscopic surgery, in which tactile function is absent
or limited, we identify pancreatic texture during needle
passing and observing elasticity gripping the pancreatic
tissue delicately with a laparoscopic hand instrument.
Considering quite high frequency of soft pancreas in
our series that was around 40%, the frequency of POPF
was 21%. This might be related to the aforementioned
features of barbed suture. Edil et al. reported similar POPF
rate in their comparative studies (V-loc vs. conventional
suture technique), however, pancreatic texture was not
mentioned in [28].
There has been a steep learning curve for laparoscopic
PD, regarding especially PJ reconstruction. Difficulties
during learning period were also reported in our previous
paper [15]. However, we have observed easier adaptation to
laparoscopic PD using V-loc suture for PJ. The shorter time
for anastomosis and comparable costs were among other
advantages. In the present study, we incorporated V-Loc
suture into the PJ technique during TLPD. Interpreting
our experience in open and laparoscopic approach, we
assume that, V-Loc barbed suture allows the surgeon to
focus particularly on subsequent stitch placement without
any effort to prevent slippage of the suture ensuring more
efficient workflow.
Laparoscopic PD remains limited to small series of
patients due to technically challenging. Suturing is one
of the key points of PJ anastomosis during TLPD, as also
mentioned by Kendrick et al. presenting the tips of the
TLPD underlining the “suturing skill is a must” [7, 32].
Given the autonomous locking mechanism of the V-Loc
through a non-traumatic way, no tension or squeeze of
the pancreas or knotting is required. In our study, the
rate of POPF and overall morbidity were 20% and 23%,
respectively. These remarkable results were attributed
to a long-standing experience in conventional PD. Given
the growing experience in laparoscopic procedures;
complication rate is decreasing whereas popularity of this
approach is rising.
Despite its merit, limitations of our study included
small size, nonrandomized, single surgical team cohort,
the lack of a control group and short-term follow-up.
CONCLUSIONS
In the last decade, rising trend in minimally invasive
approach in hepato-pancreato-biliary surgery has provided
promising outcome, especially in pancreaticoduodenectomy that result in enhanced recovery. The primary challenge
is the pancreaticojeunostomy, the most technically
demanding part that directly affects the outcome.
Application of the V-Loc suture in pancreaticojejunostomy
is technically easier which is of advantage to the surgeon
learning laparoscopic PD and provides promising outcome.
Author contributions
Karatepe O and Battal M contributed to the conception
and design, acquisition of data, or analysis and
interpretation of data; Karatepe O and Yazici P drafted the
article or revising it critically for important intellectual
content; Karatepe O and Battal M made the final approval
of the version to be published.
Conflict of Interest
Authors declared no conflict of interest and financial
disclosure.
References
- Gagner M, Pomp A. Laparoscopic pylorus-preserving pancreatoduodenectomy. Surg Endosc 1994; 8:408-10. [PMID: 7915434]
- Lai, Eric CH, Yang GP, Tang CN. Robot-assisted laparoscopic pancreaticoduodenectomy versus open pancreaticoduodenectomy – A comparative study. Int J Surg 2012; 10:475-9. [PMID: 22732431]
- Dulucq JL, Wintringer P, Mahajna A. Laparoscopic pancreaticoduodenectomy for benign and malignant diseases. Surg Endosc 2006; 20:1045-50. [PMID: 16736311]
- Chen S, Chen JZ, Zhan Q, Deng XX, Shen BY, Peng CH, et al. Robot-assisted laparoscopic versus open pancreaticoduodenectomy: a prospective, matched, mid-term follow-up study. Surg Endosc 2015; 29:3698-711. [PMID: 25761559]
- Boggi U, Palladino S, Massimetti G, Vistoli F, Caniglia F, De Lio N, et al. Laparoscopic robot-assisted versus open total pancreatectomy: a case-matched study. Surg Endosc 2015; 29:1425-32. [PMID: 25159652]
- Palanivelu C, Jani K, Senthilnathan P, Parthasarathi R, Rajapandian S, Madhankumar MV, et al. Laparoscopic pancreaticoduodenectomy: technique and outcomes. J Am Coll Surg 2007; 205:222-30. [PMID: 17660068]
- Kendrick ML, Cusati D. Total laparoscopic pancreaticoduodenectomy: feasibility and outcome in an early experience. Arch Surg 2010; 145:19-23. [PMID: 20083750]
- Croome KP, Farnell MB, Que FG, Reid-Lombardo KM, Truty MJ, Nagorney DM, et al. Total laparoscopic pancreaticoduodenectomy for pancreatic ductal adenocarcinoma: oncologic advantages over open approaches? Ann Surg 2014; 260:633-8; discussion 638-40. [PMID: 25203880]
- Malya FU, Karatepe O, Bektasoglu H, Cipe G, Bozkurt S, Hasbahceci M, et al. A Reliable Pancreaticojejunal Anastomosis with V-Loc 180 Wound Closure Device for Soft Pancreatic Stump. Hepatogastroenterology 2014; 61:484-488. [PMID: 24901167]
- Ramacciato G, Mercantini P, Petrucciani N, Nigri GR, Kazemi A, Muroni M, et al. Risk factors of pancreatic fistula after pancreaticoduodenectomy: a collective review. Am Surg 2011; 77:257-69. [PMID: 21375833]
- Lai EC, Lau SH, Lau WY. Measures to prevent pancreatic fistula after pancreatoduodenectomy: a comprehensive review. Arch Surg 2009; 144:1074-80. [PMID: 19917946]
- Gagner M, Palermo M. Laparoscopic Whipple procedure: review of the literature. J Hepatobiliary Pancreat Surg 2009; 16:726-30. [PMID: 19636494]
- Gumbs AA, Rodriguez Rivera AM, Hoffman JP, Milone L. Laparoscopic pancreatoduodenectomy: a review of 285 published cases. Ann Surg Oncol 2011; 18:1335-41. [PMID: 21207166]
- Chapman S, Turo R, Cross W. Vesicourethral anastomosis using V-Loc™ barbed suture during robot-assisted radical prostatectomy. Cent European J Urol 2011; 64:236. [PMID: 24578901]
- Battal M, Yilmaz A, Ozturk G, Karatepe O. The difficulties encountered in conversion from classic pancreaticoduodenectomy to total laparoscopic pancreaticoduodenectomy. J Minim Access Surg 2016; 12:338-41. [PMID: 27251830]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205-13. [PMID: 15273542]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. International Study Group on Pancreatic Fistula Definition: Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138:8-13. [PMID: 16003309]
- Zhou NX, Chen JZ, Liu Q, Zhang X, Wang Z, Ren S, et al. Outcomes of pancreatoduodenectomy with robotic surgery versus open surgery. Int J Med Robot 2011; 7:131-7. [PMID: 21412963]
- Chen K, Pan Y, Liu XL, Jiang GY, Wu D, Maher H, et al. Minimally invasive pancreaticoduodenectomy for periampullary disease: a comprehensive review of literature and meta-analysis of outcomes compared with open surgery. BMC Gastroenterol 2017; 17:120. [PMID: 29169337]
- Corcione F, Pirozzi F, Cuccurullo D, Piccolboni D, Caracino V, Galante F, et al. Laparoscopic pancreaticoduodenectomy: experience of 22 cases. Surg Endosc 2013; 27:2131–2136. [PMID: 23355144]
- Ricci C, Casadei R, Taffurelli G, Pacilio CA, Ricciardiello M, Minni F. Minimally Invasive Pancreaticoduodenectomy: What is the Best "Choice"? A Systematic Review and Network Meta-analysis of Non-randomized Comparative Studies. World J Surg 2018; 42:788-805. [PMID: 28799046]
- Shrikhande SV, Barreto G, Shukla PJ. Pancreatic fistula after pancreaticoduodenectomy: the impact of a standardized technique of pancreaticojejunostomy. Langenbecks Arch Surg 2008; 393:87-91. [PMID: 17703319]
- Kaul S, Sammon J, Bhandari A, Peabody J, Rogers CG, Menon M. A novel method of urethrovesical anastomosis during robot-assisted radical prostatectomy using a unidirectional barbed wound closure device: feasibility study and early outcomes in 51 patients. J Endourol 2010; 24:1789-1793. [PMID: 20626271]
- Sammon J, Kim TK, Trinh QD, Bhandari A, Kaul S, Sukumar S, et al . Anastomosis during robot-assisted radical prostatectomy: randomized controlled trial comparing barbed and standard monofilament suture. Urology 2011; 78:572-9. [PMID: 21782218]
- Tewari A, Jhaveri J, Rao S, Yadav R, Bartsch G, Te A, et al. Total reconstruction of the vesico-urethral junction. BJU Int 2008; 101:871-7. [PMID: 18321319]
- Williams SB, Alemozaffar M, Lei Y, Hevelone N, Lipsitz SR, Plaster BA, et al. Randomized controlled trial of barbed polyglyconate versus polyglactin suture for robot-assisted laparo- scopic prostatectomy anastomosis: technique and outcomes. Eur Urol 2010; 58:875-881. [PMID: 20708331]
- Lin Y, Lai S, Huang J, Du L. The Efficacy and Safety of Knotless Barbed Sutures in the Surgical Field: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sci Rep 2016; 6:23425. [PMID: 27005688]
- Edil BH, Cooper MA, and Makary MA. Laparoscopic Pancreaticojejunostomy Using a Barbed Suture: A Novel Technique. J Laparoendosc Adv Surg Tech 2014; 24:887-891. [PMID: 25412083]
- Graham JA, Kayser R, Smirniotopoulos J, Nusbaum JD, Johnson LB. Probability prediction of a postoperative pancreatic fistula after a pancreaticoduodenectomy allows for more transparency with patients and can facilitate management of expectations. J Surg Oncol 2013; 108:137-138. [PMID: 23775846]
- Wellner UF, Kayser G, Lapshyn H, Sick O, Makowiec F, Höppner J, et al. A simple scoring system based on clinical factors related to pancreatic texture predicts postoperative pancreatic fistula preoperatively. HPB (Oxford) 2010; 12:696-702. [PMID: 21083795]
- Belyaev O, Munding J, Herzog T, Suelberg D, Tannapfel A, Schmidt WE, et al. Histomorphological features of the pancreatic remnant as independent risk factors for postoperative pancreatic fistula: a matched-pairs analysis. Pancreatology 2011; 11:516-524. [PMID: 22056514]
- Tewari M. Laparoscopic Pancreatic resections for cancer. Pushing the boundaries. Indian J Surg 2015; 77:428-32. [PMID: 26722207]





