Keywords
Enteral Nutrition; Jejunum; Nutritional Status; Pancreatitis, Chronic
Abbreviations
CCK: cholecystokinin; CRP: C-reactive protein
INTRODUCTION
Chronic pancreatitis develops following repetitive or sustained injury to the pancreas and occurs secondary to excessive alcohol intake in 60-70% of chronic pancreatitis patients [1]. The UK incidence of chronic pancreatitis is 1 per 100,000 per annum (UK prevalence 3 per 100,000) [2] and it may follow a slow burning pattern or be characterised by acute episodes with quiescent intermittent periods. The complications of chronic pancreatitis are part of a wide spectrum that not only affect the pancreas itself, but also other organ systems and the condition is associated with significant morbidity and mortality.
The management of chronic pancreatitis remains challenging. Patients should be encouraged to stop drinking and smoking, and to partake of a healthy lifestyle; however, analgesia, often in the form of opiates, is almost always required and can lead to dependence [3, 4]. Ultimately, invasive options such as endoscopic and surgical manoeuvres, including Frey’s and Beger’s procedures, as well as total pancreatectomy with autologous islet cell transplantation, may become necessary [3]. Novel methods such as pain-modifying agents, coeliac plexus and nervous blocks, antioxidants and radiation therapy may have a role to play in the future [3, 5].
Following disease development, a combination of factors lead to nutritional deterioration and significant weight loss, often necessitating long-term programmes of nutrition, prolonged hospital admission and substantial use of health-care resources. Attacks of chronic pancreatitis generate a metabolic response that may be indistinguishable from attacks of acute pancreatitis [6] or sepsis [7, 8], and that may increase with the severity of the disease episode [9]. Experimental studies reveal that hypermetabolic states may subsequently occur with resting energy expenditure of 30-50% above normal [10, 11], effects that can be raised even further by the presence of sepsis [10]. Further, skeletal muscle proteolysis may lead the circulating aminoacid pool to fall to 40% of normal and muscle mass by 15% [12]. Furthermore, pancreatitis patients with a persistently negative nitrogen balance have been shown to have a significantly elevated mortality rate [13].
Therefore, chronic pancreatitis creates a hypermetabolic state that rapidly depletes in-built nutritional stores and is exacerbated by pain, nausea and vomiting, ileus, gastric stasis, dysmotility, outlet obstruction, and continuing alcohol consumption that all contribute to decreased nutritional intake and ongoing pancreatic damage [14, 15]. Pancreatic damage in chronic pancreatitis results in reduced pancreatic enzyme secretion, as well as decreased bicarbonate secretion, thus acting to further affect the functionality of the secreted pancreatic enzymes by providing an inhospitable environment [14].
Pancreatic damage clinically affects fat digestion before that of carbohydrate and protein, resulting in steatorrhoea [15] and deficiencies in vitamins A, D, E and K [16]. As function deteriorates further and lipase and trypsin secretion decrease, azotorrhoea may also develop [16]. Metabolic errors can also occur, as the catabolic stress state leads to increased levels of catecholamines and cortisol, and a subsequent disturbance in the insulin/glucagon ratio, beta cell dysfunction and insulin resistance may follow [6, 17]. Insulin may therefore be required in more than 80% of patients not previously diagnosed as diabetic [6] and new diagnoses of diabetes will follow in 20-30% as beta cell mass decreases [6, 18, 19]. Fat metabolism is further altered as lipolysis and lipid oxidation increase [6, 20]. Despite this, fat clearance can be reduced, leading to hypercholesterolaemia and hypertriglyceridaemia [6, 12, 21]. Specific deficiencies in calcium, magnesium, zinc, thiamine and folic acid have also been reported [1] and thus the trace element and nutritional deficiencies already present in ethanolic patients can be further compounded [18].
Although guidelines now advocate the use of nasogastric or nasojejunal feeding in acute pancreatitis, at present there are no British Society of Gastroenterology or Department of Health guidelines to guide the nutritional management of patients with chronic pancreatitis. Although small bowel can be routinely accessed for enteral feeding, by either percutaneous endoscopic gastrojejunostomy or direct percutaneous endoscopic jejunostomy, there is only minimal data regarding clinical outcome and safety of long-term jejunal feeding in chronic pancreatitis.
Aims
The aim of our study was to assess the effectiveness of a nasojejunal nutrition programme in patients with chronic pancreatitis, and in particular to evaluate weight effects, as well as tolerance and complications associated with nasojejunal nutrition.
METHODS
Patients
All patients admitted to our tertiary pancreatic unit, with a diagnosis of chronic pancreatitis that were fed via the nasojejunal route, between January 2004 and December 2007, were included in the study. Data were retrospectively collected from the patient’s medical records.
A diagnosis of chronic pancreatitis was made based upon the Marseille-Rome classification (1988) following assessment of symptom profile (including abdominal pain, weight loss, nausea and vomiting) and imaging characteristics of chronic pancreatitis (including calcification, duct dilatation and stricturing and glandular atrophy).
Abdominal pain, analgesic requirements and gastrointestinal symptoms were evaluated by clinical assessment during the patient’s initial admission, during any re-admissions and also during their follow up consultations.
Insertion of Nasojejunal Catheters
Nasojejunal catheters were inserted for standardised indications including inability to tolerate oral feeding or inability to ingest sufficient calories for body weight (pain or duodenal stenosis); gross weight loss (more than 10% of pre-morbid body weight); or acute complications of chronic pancreatitis contributing to the aforementioned (such as pseudocyst, fistula, pseudoaneurysm, acute inflammation or acute pain). Nasojejunal catheters were inserted by direct endoscopic placement through the pylorus and over a guidewire. Fine-bore (6-10 French gauge) tubes were inserted and fluoroscopic screening was utilised if necessary to confirm placement.
Feeding
Correct placement of nasojejunal catheters was confirmed radiologically and feeding commenced within 24 hours of insertion. A standard, semielemental nasojejunal feeding regime was initiated in all patients at a rate of 30 mL/h. The feeding rate was subsequently increased by 10 mL/h every 12 hours until the patient was reviewed by a dietician; 1,200 mL of the standard feed provided 1,560 kcal (1.3 kcal/mL), 80 g protein, 52 mmol Na+ and 53 mmol K+.
All patients were reviewed by a dietician within 48 hours and an individualised feeding regimen established with the goal of reaching full caloric requirement on day 3 (30 mL/kg/day of 1 kcal/mL feed). The regimen was subsequently altered according to the patient’s clinical course and physical activity. Patients were allowed to consume oral liquids as their clinical course improved and their tolerance increased; they were also allowed to take oral medications.
All patients were discharged with a nasojejunal tube in situ only once their analgesic provision was adequate or their pain had settled; they were capable of managing their nasojejunal catheter and nutrition; they had no active or acute complications of chronic pancreatitis; and a home care package had been established.
Follow-up
Patients were closely followed up in the out-patient department by surgery, gastroenterology and dietician teams. Upon review, patients were routinely asked about complications associated with the feeding technique and also to crudely rate their tolerance of the feed as ‘excellent’, ‘good’, ‘average’, or ‘poor’.
ETHICS
The study incorporated a retrospective, observational cohort and therefore no formal, written informed consent was taken or institutional ethical approval requested. The study protocol conformed to the Declaration of Helsinki.
STATISTICS
Data are reported as frequencies and median and range or mean±SD values. Statistical analysis was carried out by using the SPSS (Statistical Package for the Social Sciences; version 16) software package. The Fisher’s exact and the Pearson chi-square tests were used for comparison of proportions for categorical data, where appropriate. The one-way ANOVA and the paired Student’s t test were used for comparisons of continuous data, where appropriate. Two-tailed P values less than 0.05 were considered statistically significant.
RESULTS
Patient Demographics
Fifty-eight (35 males, 23 females) patients with chronic pancreatitis were admitted to our tertiary pancreatic unit and fed via a nasojejunal route, between January 2004 and December 2007.
The median patient age was 46 years (range: 20-67 years) and median age of diagnosis was 43 years (range: 18-62 years). Median time from diagnosis of chronic pancreatitis to nasojejunal feeding was two years (range 0-23 years) and the median follow-up period was 16 months (range: 3-36 months).
Available data identified the aetiological cause as alcohol in 35 patients (60.3%), gallstones in 23 (22.4%), idiopathic in 6 (10.3%), and hyperlipidaemia, post-ERCP, drugs (steroids) and a peri-ampullary mass in one patient (1.7%) each.
Patients were discharged from hospital after a median of 14 days (range: 8-74 days) and nasojejunal feeding continued for a median of 47 (28-139 days) days in total.
Weight Effects
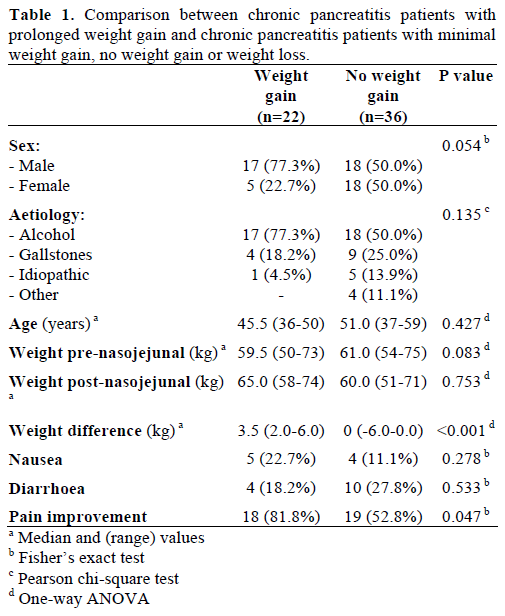
The patient’s median weight prior to initiation of nasojejunal feeding was 60.0 kg (range: 42-123 kg) and 61.5 kg (range: 48-108 kg) at post-nasojejunal feeding review. Median weight change was +1 kg (range: from -24 to +27 kg; P=0.454). There was no association between aetiology and change in weight (P=0.130). A comparison of those patients experiencing a prolonged weight gain with those experiencing minimal weight gain, no weight gain or weight loss demonstrates that the former were more likely to be younger, male and have an alcohol aetiology; further, the use of nasojejunal feeding was more likely to be associated with improvements in pain in weight gain chronic pancreatitis patients (although none of the aforementioned results reached statistical significance; Table 1).
Analgesic Effect
All patients presented with abdominal pain, requiring at least weekly opiate derivatives as analgesia. Fortysix patients (79.3%) reported resolution of their abdominal pain and cessation of opioid analgesia intake over the nasojejunal feeding period (Figure 1); although some patients underwent additional procedures for the management of acute complications. Upon discharge, 35 (60.3%) patients were still taking regular simple analgesia (paracetamol/ibuprofen) and 12 patients (20.7%) were still taking at least weekly opioid derivatives.
Figure 1. The outcome following nasojejunal nutrition in this cohort
of patients with chronic pancreatitis.
Twelve (20.7%) patients reported significant pain recurrence during the follow-up period (median time to recurrence 4 months; range: 1-25 months). There was no association between aetiology and analgesic effect.
Tolerance and Complications
Forty-two (72.4%) patients reported their tolerance of the feeding regime as ‘good’ or ‘excellent’ (Figure 1). Only 4 (7%) patients reported their tolerance of the feeding regime as ‘poor’.
Complications were largely minor and infrequent, with diarrhoea (as per subjective patient assessment of alteration in bowel habit to looser or more frequent) occurring in 14 patients (24.1%) and nausea (as per subjective patient assessment) in a further 9 patients (15.5%) (Figure 2). Eleven (19.0%) patients required re-admission for tube blockage and 10 (17.2%) for tube displacement, mandating catheter reinsertion or repositioning. There were no complications associated with nasojejunal catheter insertion and there was no association between aetiology and tolerance or complications (data not shown).
Figure 2. Complications associated with nasojejunal nutrition in this
cohort of patients with chronic pancreatitis.
Pancreatic Morphology
Twenty patients (34.5%) showed radiological improvement in their pancreatic morphology, as assessed on routine computed tomography (Figure 1).
Blood Tests
Thirty-nine patients (67.2%) had blood tests on both the day of nasojejunal feeding commencement and cessation. Over the period of the nasojejunal feeding, significant improvements were seen in many blood and serum parameters, including sodium (from 134.8 to 138.1 mEq/L; P<0.001), urea (from 3.4 to 5.1 mmol/L; P<0.001), creatinine (from 58.3 to 60.3 μmol/L; P<0.001), corrected calcium (from 2.24 to 2.35 mmol/L; P=0.018), albumin (from 34.5 to 38.7 g/L; P=0.002), CRP (from 73.0 to 25.5 mg/L; P=0.006), and haemoglobin (from 11.8 to 12.4 g/dL; P=0.036) (Table 2).
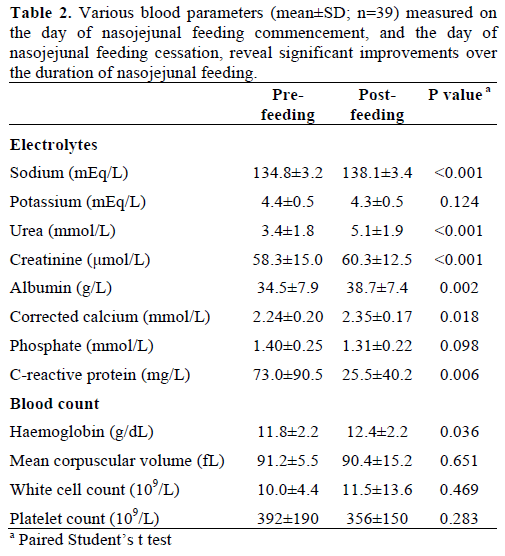
Phosphate measured at 24 hours for assessment of refeeding syndrome was 1.31±0.22 mmol/L while the values measured before feeding were 1.40±0.25 mmol/L (P=0.098).
Outcome
Twelve patients (20.7%) went on to have definitive surgical management of their chronic pancreatitis during the follow-up period.
DISCUSSION
In mild chronic pancreatitis, abstinence from alcohol and effective analgesia can often be sufficient to control pain and enable nutritional improvements through oral intake. Replacement of pancreatic enzymes and acid suppression are of modest effectiveness in treating pain [5]; and frequent small meals, low in fat but rich in carbohydrates, calories and protein, are important to maintain adequate nutrition [22]. Fat soluble vitamins and other micronutrients should be supplemented as clinically indicated. More than 80% of patients can usually be treated adequately with standard food supplemented by pancreatic enzymes [1], only 10-15% of patients will require oral nutritional supplements and enteral tube feeding is only indicated in approximately 5% [1, 23], usually for treatment of severe pain, significant weight loss or acute complications.
A recent plethora of investigations, although mainly focusing upon acute pancreatitis, have shown that enteral nutrition is associated with attenuation of the acute phase response [24], a lower rate of sepsis-related complications (particularly extra-pancreatic) [25, 26], improved glucose control [25], decreased financial cost [26], possible reduced length of hospital stay [27, 28] and possible reduced mortality rates [27]. The enteral route may also be useful in preventing gut compromise as this may serve as a trigger and perpetuator of multiple organ failure or sepsis in pancreatitis [29]. This observational study demonstrates that the use of nasojejunal nutrition in patients with chronic pancreatitis can be safely commenced in hospital and continued following discharge. Further, its use is associated with improvements in weight and blood parameters, as well as being well-tolerated and associated with minimal complications.
Our findings mirror the few studies investigating the role of nasojejunal feeding in chronic pancreatitis. Hamvas et al. observed 19 patients with necrotising chronic pancreatitis to show that 12 fed via a nasojejunal route recovered more quickly and required less interventions than 7 patients fed via a parenteral route [30, 31]. Similarly, Stanga et al. [23] retrospectively analysed 57 chronic pancreatitis patients (median duration of jejunal feeding 113 days) to illustrate an average weight increase of 4.3 kg (P<0.05) and a decrease in the proportion of patients with significant abdominal pain (96% to 23%; P<0.05), as well as noting that complications were largely minor and infrequent. Interestingly, patients with nonalcoholic pancreatitis suffered from ongoing weight loss and failure to put on weight as well as a higher number of physician visits due to abdominal pain and gastrointestinal complications. The authors concluded that reduced pancreatic gland stimulation may be the key to producing these effects, although the critical underlying mechanisms remained unclear. Ogara et al. [32] utilised nasojejunal feeding catheters in 30 chronic pancreatitis patients for a median duration of 4.6 months and median follow-up of 7.5 months. Nine out of 20 patients that had reported uncontrolled pain at initial evaluation reported pain levels that were completely, or nearly completely, resolved following treatment with jejunal feeds alone (P=0.0008). However, the cohort underwent a mean weight loss of 1.6 kg (P=0.27) (although some patients had suspected malignancy) and 12 patients suffered complications in total.
Pain associated with chronic pancreatitis is extremely challenging to manage and remains largely resistant to therapy, partly because the mechanisms underlying it are poorly understood. Elevated cholecystokinin (CCK) levels are one of the proposed mechanisms leading to pain in chronic pancreatitis [33] and feeding low in the gastrointestinal tract may invoke a minimal degree of pancreatic stimulation [34], thus decreasing CCK levels. However, Keith et al. investigated two patients with chronic pancreatitis to illustrate no change in volume or amylase output in response to intra-jejunal infusion of an elemental formula [35]. Further, despite the fact that the concept of resting the pancreas by decreasing its stimulatory activity makes physiological sense, it remains difficult to definitively prove any beneficial effects upon pain relief or outcome [12, 36, 37] and the fact that at least minor baseline pancreatic enzyme secretion occurs means that the pancreas is never fully ‘rested’ [38]. However, jejunal feeding may help to reduce other gastrointestinal complications that may contribute to pain [23], such as gastric paresis with associated symptoms such as nausea, vomiting and abdominal pain [39, 40, 41]. Elemental and semi-elemental feeds are more effective at reducing exocrine secretion than standard feeds with intact proteins at oral [42, 43], duodenal [44] and jejunal [45] levels. Elemental formulae also lead to decreased gastric acid production and further decreased pancreatic stimulation [46].
Although there are no studies correlating the degree of undernutrition with the course of disease in chronic pancreatitis, poor nutritional status is likely to contribute to a negative outcome [1]. Nutritional assessment and management therefore remains crucial not only in the context of outcome from disease but also in planning any future intervention. Improvements in certain blood parameters in this study, such as CRP, platelets and haemoglobin, require interpretation in the context of the patient’s improving disease profile during the study period and caution should be taken in attributing them directly to the use of nasojejunal feeding alone. However, hyponatremia is one of the commonest abnormalities found in hospital in-patients [47] and its presence in many critically ill patients is associated with an increased risk of death and illnessassociated morbidity [48, 49]. Under normal circumstances, the plasma sodium concentration is maintained within a narrow range; however, chronic inflammatory diseases, such as chronic pancreatitis, may affect this balance by producing an excess of interleukin-6 [50], while alcoholism and liver cirrhosis can also lead to hyponatremia. Thus, chronic pancreatitis patients may be at significant risk of hyponatraemia and nasojejunal feeding may be an effective way of correcting this imbalance. Significant increases in albumin, urea and creatinine were also observed in this study; however, such surrogate markers of nutrition and malnutrition have often been used with contention and their clinical relevance debated [51, 52]. Less contentious would be their use as surrogate markers for gain in lean body weight, an expected result of an appropriate feeding regime. However, whilst a gain in weight was seen (and inferred from the biochemical results to be lean body mass) this was not significant; although an initial weight loss period during the acute phase of the disease may have reduced the overall net weight gain effect. In future studies, serial, objective measures of muscle mass may be useful to circumvent this issue [53]. Refeeding syndrome is also a concern in the initiation of feeding in the malnourished or starved and is characterised by hypophospahatemia and hypokalemia [54, 55]. Whilst mean phosphate levels declined during the first 24 hours of feeding (from 1.40 to 1.31 mmol/L; P=0.098), none fell below the normal range and nasojejunal feeding in this population does not seem to be associated with an increased risk of refeeding syndrome.
CONCLUSION
Reduction in malnutrition, adequate energy and calorie intake, and relief of pain are the main goals of therapy in chronic pancreatitis, all of which can be aided via the delivery of nasojejunal nutrition. However, all home-based or long-term nutrition programmes for chronic pancreatitis should be developed in a multidisciplinary setting with the involvement of gastroenterology, radiology, dietician and nursing colleagues. Aetiological factors, complications, and changing severity and nutritional requirements mandates that nutrition teams work closely with surgical and gastroenterological colleagues to swiftly resolve the disease process and reduce the likelihood of long-term complications.
The limitations of this and other studies, including the retrospective nature of the cohorts, and the lack of objective pain assessments and control groups, mandates future randomised controlled trials to further assess the effect of nasojejunal feeding in chronic pancreatitis.
Acknowledgements
J.R.A.S., who is supported as the ‘Jason Boas Hepatopancreaticobiliary Fellow’ by the No Surrender Charitable Trust, drafted the manuscript. All authors have significantly contributed to, read and approved the final manuscript. A part of these data was presented at the “Association of Surgeons of Great Britain and Ireland Conference 2008”
Conflict of interest
All authors declare that they have no competing interests
References
- Meier R, Ockenga J, Pertkiewicz M, Pap A, Milinic N, Macfie J, et al. ESPEN Guidelines on Enteral Nutrition: Pancreas. ClinNutr 2006; 25:275-84. [PMID 16678943]
- Goldacre MJ, Roberts SE. Hospital admission for acute pancreatitis in an English population, 1963-98: database study of incidence and mortality. BMJ 2004; 328:1466-9. [PMID 15205290]
- Gachago C, Draganov PV. Pain management in chronic pancreatitis. World J Gastroenterol 2008; 14:3137-48. [PMID 18506917]
- Giger U, Stanga Z, DeLegge MH. Management of chronic pancreatitis. NutrClinPract 2004; 19:37-49. [PMID 16215095]
- Abdel Aziz AM, Lehman GA. Current treatment options for chronic pancreatitis. Curr Treat Options Gastroenterol 2007; 10:355- 68. [PMID 17897574]
- Havala T, Shronts E, Cerra F. Nutritional support in acute pancreatitis. GastroenterolClin North Am 1989; 18:525-42. [PMID 2509354]
- Di Carlo V, Nespoli A, Chiesa R, Staudacher C, Cristallo M, Bevilacqua G, Staudacher V. Hemodynamic and metabolic impairment in acute pancreatitis. World J Surg 1981; 5:329-39. [PMID 7293195]
- Shaw JH, Wolfe RR. Glucose, fatty acid, and urea kinetics in patients with severe pancreatitis. The response to substrate infusion and total parenteral nutrition. Ann Surg 1986; 204:665-72. [PMID 3098198]
- Curtis CS, Kudsk KA. Nutrition support in pancreatitis. SurgClin North Am 2007; 87:1403-15, viii. [PMID 18053838]
- Dickerson RN, Vehe KL, Mullen JL, Feurer ID. Resting energy expenditure in patients with pancreatitis. Crit Care Med 1991; 19:484-90. [PMID 2019133]
- Hébuterne X, Hastier P, Péroux JL, Zeboudj N, Delmont JP, Rampal P. Resting energy expenditure in patients with alcoholic chronic pancreatitis. Dig Dis Sci 1996. 41: 533-9. [PMID 8617130]
- Helton WS. Intravenous nutrition in patients with acute pancreatitis. In: Rombeau JL (Ed). Clinical Nutrition: Parenteral Nutrition. W.B. Saunders 1990. p. 442-461.
- Sitzmann JV, Steinborn PA, Zinner MJ, Cameron JL. Total parenteral nutrition and alternate energy substrates in treatment of severe acute pancreatitis. SurgGynecolObstet 1989; 168:311-7. [PMID 2494706]
- Petersen JM, Forsmark CE. Chronic pancreatitis and maldigestion. SeminGastrointest Dis 2002; 13:191-9. [PMID 12462705]
- DiMagno EP, Go VL, Summerskill WH. Relations between pancreatic enzyme ouputs and malabsorption in severe pancreatic insufficiency. N Engl J Med 1973; 288:813-5. [PMID 4693931]
- Twersky Y, Bank S. Nutritional deficiencies in chronic pancreatitis. GastroenterolClin North Am 1989; 18:543-65. [PMID 2680966]
- Marulendra S, Kirby DF. Nutrition support in pancreatitis. NutrClinPract 1995; 10:45-53. [PMID 7731424]
- Holt S. Chronic pancreatitis. South Med J 1993; 86:201-7. [PMID 8434293]
- Latifi R, McIntosh JK, Dudrick SJ. Nutritional management of acute and chronic pancreatitis. SurgClin North Am 1991; 71:579-95. [PMID 1904645]
- Cerra FB. Hypermetabolism, organ failure, and metabolic support. Surgery 1987; 101:1-14. [PMID 3541266]
- Kohn CL, Brozenec S, Foster PF. Nutritional support for the patient with pancreatobiliary disease. Crit Care NursClin North Am 1993; 5:37-45. [PMID 8448001]
- DiMagno EP. Medical treatment of pancreatic insufficiency. Mayo ClinProc 1979; 54:435-42. [PMID 36518]
- Stanga Z, Giger U, Marx A, DeLegge MH. Effect of jejunal long-term feeding in chronic pancreatitis. JPEN J Parenter Enteral Nutr 2005; 29:12-20. [PMID 15715269]
- Windsor AC, Kanwar S, Li AG, Barnes E, Guthrie JA, Spark JI, Welsh F, et al. Compared with parenteral nutrition, enteral feeding attenuates the acute phase response and improves disease severity in acute pancreatitis. Gut 1998; 42:431-5. [PMID 9577354]
- Eckerwall GE, Axelsson JB, Andersson RG. Early nasogastric feeding in predicted severe acute pancreatitis: A clinical, randomized study. Ann Surg 2006; 244:959-65. [PMID 17122621]
- Petrov MS, Kukosh MV, Emelyanov NV. A randomized controlled trial of enteral versus parenteral feeding in patients with predicted severe acute pancreatitis shows a significant reduction in mortality and in infected pancreatic complications with total enteral nutrition. Dig Surg 2006; 23:336-44. [PMID 17164546]
- McClave SA, Chang WK, Dhaliwal R, Heyland DK. Nutrition support in acute pancreatitis: a systematic review of the literature. JPEN J Parenter Enteral Nutr 2006; 30:143-56. [PMID 16517959]
- Gupta R, Patel K, Calder PC, Yaqoob P, Primrose JN, Johnson CD. A randomised clinical trial to assess the effect of total enteral and total parenteral nutritional support on metabolic, inflammatory and oxidative markers in patients with predicted severe acute pancreatitis (APACHE II > or =6). Pancreatology 2003; 3:406-13. [PMID 14526151]
- De Beaux AC, Plester C, Fearon KC. Flexible approach to nutritional support in severe acute pancreatitis. Nutrition 1994; 10:246-8. [PMID 7919677]
- Hamvas J, Schwab R, Pap A. Jejunal feeding in chronic pancreatitis with severe necrosis. JOP. J Pancreas (Online) 2001; 2:112-6. [PMID 11870333]
- Hamvas J, Pap A. The role of jejunal feeding in the treatment of acute necrotizing pancreatitis and in recurrence of chronic pancreatitis with severe necrosis. OrvHetil 1998: 139:945-9. [PMID 9595928]
- Ogara M, Fang JC, Peterson KA, Disario JA. Jejunal feeding in chronic pancreatitis. GastrointestEndosc 2007; 65:AB248.
- Toskes PP. Update on diagnosis and management of chronic pancreatitis. CurrGastroenterol Rep 1999; 1:145-53. [PMID 10980942]
- Corcoy R, Sanchez JM, Domingo P, Net A. Nutrition in the patient with severe acute pancreatitis. Nutrition 1988; 4:269-75.
- Keith RG. Effect of a low fat elemental diet on pancreatic secretion during pancreatitis. SurgGynecolObstet 1980; 151:337-43. [PMID 7404299]
- Ranson JH. Acute pancreatitis: pathogenesis, outcome and treatment. ClinGastroenterol 1984; 13:843-63. [PMID 6386241]
- Kirby DF, Craig RM. The value of intensive nutritional support in pancreatitis. JPEN J Parenter Enteral Nutr 1985; 9:353-7. [PMID 3925181]
- Povoski SP, Nussbaum MS. Nutrition support in pancreatitis: fertile ground for prospective clinical investigation. NutrClinPract 1995; 10:43-4. [PMID 7731423]
- Chowdhury RS, Forsmark CE, Davis RH, Toskes PP, Verne GN. Prevalence of gastroparesis in patients with small duct chronic pancreatitis. Pancreas 2003; 26:235-8. [PMID 12657948]
- Davies AR, Froomes PR, French CJ, Bellomo R, Gutteridge GA, Nyulasi I, et al. Randomized comparison of nasojejunal and nasogastric feeding in critically ill patients. Crit Care Med 2002; 30:586-90. [PMID 11990920]
- Montejo JC, Grau T, Acosta J, Ruiz-Santana S, Planas M, García-De-Lorenzo A, et al. Multicenter, prospective, randomized, single-blind study comparing the efficacy and gastrointestinal complications of early jejunal feeding with early gastric feeding in critically ill patients. Crit Care Med 2002; 30:796-800. [PMID 11940748]
- Neviackas JA, Kerstein MD. Pancreatic enzyme response with an elemental diet. SurgGynecolObstet 1976; 142:71-4. [PMID 801]
- McArdle AH, Echave W, Brown RA, Thompson AG. Effect of elemental diet on pancreatic secretion. Am J Surg 1974; 128:690-2. [PMID 4440810]
- Guan D, Ohta H, Green GM. Rat pancreatic secretory response to intraduodenal infusion of elemental vs polymeric defined-formula diet. JPEN J Parenter Enteral Nutr 1994; 18:335-9. [PMID 7933441]
- Vison N, Hecketsweiler P, Butel J, Bernier JJ. Effect of continuous jejunal perfusion of elemental and complex nutritional solutions on pancreatic enzyme secretion in human subjects. Gut 1978; 19:194-8. [PMID 631640]
- Voitk A, Brown RA, Echave V, McArdle AH, Gurd FN, Thompson AG. Use of an elemental diet in the treatment of complicated pancreatitis. Am J Surg 1973; 125:223-7. [PMID 4688003]
- Adrogue HJ, Madias NE. Hyponatremia. N Engl J Med 2000; 342:1581-9. [PMID 10824078]
- Gheorghiade M, Abraham WT, Albert NM, GattisStough W, Greenberg BH, O'Connor CM, et al. Relationship between admission serum sodium concentration and clinical outcomes in patients hospitalized for heart failure: an analysis from the OPTIMIZE-HF registry. Eur Heart J 2007; 28:980-8. [PMID 17309900]
- Nair V, Niederman MS, Masani N, Fishbane S. Hyponatremia in community-acquired pneumonia. Am J Nephrol 2007; 27:184-90. [PMID 17356253]
- Murakami T, Matoba H, Kuga Y, Ozawa S, Kubota K, Yoshida S. Hyponatremia in a patient with chronic inflammatory disease. Intern Med 1998; 37:792-5. [PMID 9804092]
- Seres DS. Surrogate nutrition markers, malnutrition, and adequacy of nutrition support. NutrClinPract 2005; 20:308-13. [PMID 16207668]
- McClave SA, Snider HL, Spain DA. Preoperative issues in clinical nutrition. Chest 1999: 115(5 Suppl.):64S-70S. [PMID 10331336]
- Seymour JM, Ward K, Sidhu PS, Puthucheary Z, Steier J, Jolley CJ, et al. Ultrasound measurement of rectus femoris cross-sectional area and the relationship with quadriceps strength in COPD. Thorax 2009; 64:418-23. [PMID 19158125]
- Crook MA, Hally V, Panteli JV. The importance of the refeeding syndrome. Nutrition 2001; 17:632-7. [PMID 11448586]
- Gariballa S. Refeeding syndrome: a potentially fatal condition but remains underdiagnosed and undertreated. Nutrition 2008; 24:604-6. [PMID 18359196]



