Keywords
Anti-Inflammatory Agents; Cholangiopancreatography, Endoscopic Retrograde /adverse effects; Pancreatitis / prevention and control
INTRODUCTION
Post-ERCP pancreatitis (PEP) is the most common major complication associated with ERCP [1]. It is distinct from asymptomatic hyperenzymemia [2] and may present with varying levels of severity, which influence inpatient length of stay and prognosis [3]. Multiple risk factors for the development of PEP have been identified and are broadly categorized into patient-dependent or procedure-dependent risks. The patient dependent risks most consistently identified are female gender, younger age, suspected sphincter of Oddi dysfunction (SOD) as an indication, previous episodes of PEP, current alcohol use, former cigarette smoking, lack of chronic pancreatitis and the presence of normal serum bilirubin. Procedure and operator dependent risk factors include difficult cannulation, pancreatic duct (PD) contrast injection (the risk of PEP increasing proportionally with number of injections), use of precut or access sphincterotomy, PD sphincterotomy, minor papilla sphincterotomy, failed clearance and operator inadequacy [1, 3-11].
The primary role of pharmacologic prevention of post- ERCP pancreatitis is to reduce the levels of intra-pancreatic enzymes and prevent the activation of digestive enzymes and lysosomal hydrolases. Over 35 different drugs have been studied to date. Chemopreventive studies have targeted various mechanisms of injury including protease inhibitors (gabexate and ulinastatin), modulators of pancreatic enzyme secretion (octreotide and somatostatin), smooth muscle relaxants (nitroglycerin, phosphodiesterase inhibitors and calcium channel blockers), and antiinflammatories (NSAIDs, corticosteroids, IL-10 and heparin). While pharmacologic prophylaxis has been appealing, many drugs have failed to show significant reduction in PEP and the prophylactic placement of PD stents has gained widespread acceptance [12-14]. The technique, however, is demanding even in experienced hands and carries costs and potentially serious adverse outcomes [15]. The administration of NSAIDs however, is generally safe, straightforward and inexpensive. Thus investigative efforts into their chemopreventive roles in PEP has emerged over the last decade.
NSAID MECHANISM OF ACTION
The pathophysiology of PEP involves various inciting events that lead to a common final pathway of inappropriate activation of pancreatic enzymes and auto-digestion. These inciting events may cause mechanical obstruction (from trauma or edema of the pancreatic sphincter or duct), may increase pancreatic ductal pressure or may be functional due to spasm of the sphincter of Oddi [16]. Infection from instrumentation, duodenal contents or increased hydrostatic pressure may also be inciting events, the latter possibly resulting from overinjection of contrast medium and subsequent damage to ductal epithelial cells [9, 16]. While conflicting evidence regarding the role of acinarization have been observed, the use of ionic contrast medium has not been found to be a significant risk factor [3, 9, 17-20]. Repeated attempts at cannulation, however, do increase the risk of developing PEP [14].
While risk factors predispose certain patients to developing PEP, there have been several steps described that take place after the inciting event which lead to a common pathophysiology of acute pancreatitis [21, 22]. After trypsinogen activation, a local inflammatory response is triggered by acinar cell damage [23] and numerous inflammatory mediators are implicated in this process, several of which are relevant to the discussion of NSAIDs and their action in PEP. The 4 main mechanisms by which NSAIDs act are: inhibition of cylcooxygenase (COX), inhibition of phospholipase A2 (PLA), prevention of leukocyte adhesion and migration, and inhibition of integrins.
The most well described mechanism is the inhibition of the COX2 enzyme, which may or may not be selective. In an early paper, Vane described the decreased production of prostaglandins by aspirin and indomethacin administration [24]. COX2 is the enzyme responsible for catalyzing the rate limiting step of the conversion of arachidonic acid to prostaglandin and thromboxane, both of which are known to be important in acute inflammatory reactions [25]. In murine models of acute pancreatitis, COX2 mRNA is increased, in turn leading to increased production of prostaglandin [26]. There have also been studies on arachidonic acid metabolites in acute pancreatitis in porcine models. In these studies pancreatitis was induced by injection of free fatty acid and various arachidonic acid metabolites were measured. The prostaglandins PGF1 alpha and PGF2 alpha and thromboxane B2 were found to be elevated in lymph, and increased levels of PGF1 were found in pancreatic venous blood [27].
Additionally, several studies have been conducted in animal models involving administration of selective or non-selective COX inhibitors. Ethridge et al. induced pancreatitis in either COX1 or COX2 knockout mice or a wild-type followed by administration of NS-398 (a selective COX2 inhibitor). They surveyed the pancreas and lungs histologically and found less severe pancreatic injury in the COX2 knockout [28]. Similar results have been confirmed using either histologic or biochemical markers of pancreatitis severity and have suggested a role of COX2 metabolites in not only local but systemic inflammation with COX2 inhibition leading to attenuated lung and renal injury [29-31].
Phospholipase A2 [PLA2] is an enzyme that catalyzes the lipolysis of phosphoglycerides at the sn-2 position and leads to the release of arachidonic acid [32]. Two different types have been described in the context of acute pancreatitis. Type II phospholipase A2 has been demonstrated to have a substantially increased activity in murine models of acute pancreatitis, particularly in necrotizing and severe variants associated with lung injury [33, 34]. The association of increased PLA2 activity with pancreatitis has also been investigated in human studies that reveal an association of increased catalytic activity of PLA2 with necrotizing pancreatitis and pancreatitis complicated by respiratory dysfunction [35, 36]. Interestingly, indomethacin has been demonstrated to reduce PLA2 activity in vitro in a study that used serum from patients with necrotizing pancreatitis as an enzymatic source [37]. The study found that indomethacin exhibited the strongest inhibition of PLA2 of all agents tested (diclofenac, ketoprofen, chlorpromazine, tobramycin, doxycycline, several coritcosteroids, bupivacaine, digoxin, lidocaine, metoprolol, and vancomycin). Of note, diclofenac did reduce PLA2 activity by 93% but at supratherapeutic administration [37].
The neutrophil adhesion and extravasation process presents another mechanism on which NSAIDs may act to ameliorate acute pancreatitis. After an appropriate stimulation from pro-inflammatory cytokines, endothelial cells and neutrophils begin the “rolling” process whereby they interact and bind with one another [38]. The end result of this process is migration of the activated neutrophil from the lumen of the capillary to the extracellular space. Further studies have suggested that NSAIDs modulate this process by exerting a dose and time dependent down-regulation on the L-selectin molecule present on the neutrophil surface [39, 40], and are important in facilitating neutrophil-endothelial cell adhesion [38].
NSAIDs are also able to interfere with the activation process of integrins important in platelet activation. The glycoprotein IIb/IIIa (αIIbβ3) integrin is an important integrin responsible for platelet aggregation and adhesion via its binding of platelets to von Willebrand factor, fibrinogen, vitronectin, fibronectin, and collegen [41]. Meloxicam, piroxicam, indomethacin and aspirin, but not aceclofenac or diclofenac, decreased integrin αIIbβ3 ativation independent of their inhibition of COX [42]. Additionally, piroxicam and meloxicam have been shown to exert several different effects on integrins in neutrophil activation. Both drugs prevent L-selectin and CD11b activation, a process important in neutrophil activation and induced by TNF and other inflammatory molecules [43]. The same study also showed that piroxicam treatment prevented changes in the beta 1 integrins important in the activation of T lymphocytes [43]. Furthermore, salicylates have also been shown to decrease T lymphocyte migration via mitigation of an integrin-mediated mechanism [44].
CLINICAL STUDIES
Initial studies evaluating the role of NSAID’s demonstrated the efficacy of oral or intramuscular administration in reducing mortality in rodents [45]. Moreover, in a double blind controlled study, Danish researchers used indomethacin 50mg twice daily rectal suppositories to demonstrate a significant reduction in the frequency and intensity of acute pancreatitis [46]. NSAIDs are inexpensive, simple to administer and relatively safe. While their application in pancreatitis is not new, their investigation for chemoprevention in PEP has been a natural progression over the last decade.
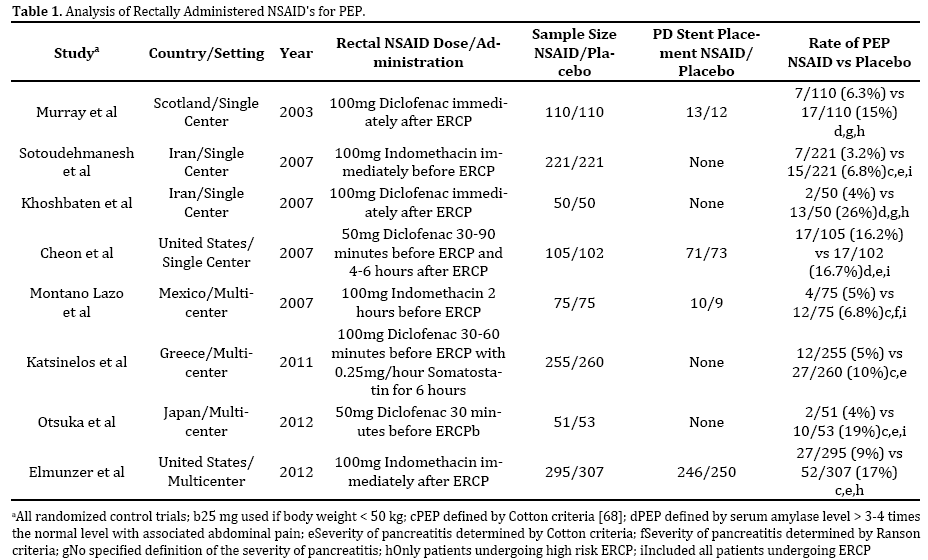
In the first randomized controlled trial (RCT), Murray et al. demonstrated the efficacy of rectal diclofenac administration immediately after ERCP to prevent PEP. A total of 220 patients were evaluated with 110 receiving rectal diclofenac and the others a placebo. PEP was reduced in the diclofenac group compared to those receiving placebo (6. 4% vs. 15. 5%, p=0. 049) [47]. While the study only marginally achieved statistical significance, interestingly it showed no benefit in the highest risk population, patients with SOD; and was further limited by the lack of multivariate analysis.
Subsequent trials evaluating the efficacy of NSAID’s yielded dichotomous results (Table 1) [47-54]. While there was a trend towards a lower incidence of PEP, the studies were complicated by differing designs and definitions of PEP; raising further questions regarding the role of NSAID prophylaxis. In a meta-analysis of four studies involving rectally administered NSAID’s (a total of 912 patients), Elmunzer et al. sought to provide clarity to this issue. The analysis revealed a pooled relative risk for PEP of 0. 36 (95%CI 0. 22-0. 60) after administration of prophylactic NSAIDs and a relative risk of 0. 30 (95%CI 0. 01-0. 76) for moderate to severe pancreatitis [55]. Rectally administered NSAID’s distinctly demonstrated a tendency toward the reduction of incidence and severity of PEP. Congruent with these findings, another metaanalysis involving 6 randomized controlled trials with a total of 1,300 patients (treatment arm included both rectal diclofenac and oral indomethacin) found a statistically significantly lower risk of PEP in the NSAID vs placebo arm [56]. Authors of both meta-analyses concluded that while NSAIDs appeared to be effective in preventing PEP, there were several limitations including the small number of trials and sample size, inconsistent definitions of PEP (two trials used serum amylase levels of 4 times the upper limit of normal), and restrictive representative populations for which widespread applicability was uncertain.
After the publication of these meta-analyses, three more trials provided further conflicting results regarding NSAID chemoprophylaxis [53, 57, 58]. While one trial had positive findings [53], two others demonstrated no benefit [57, 58]. Given the inconsistent data, rectal NSAID’s were infrequently used in practice. Furthermore, despite the evidence from animal trials (discussed above) suggesting the efficacy of selective COX2 inhibitors in acute pancreatitis, a human study of valdecoxib in the prevention of PEP showed no significant effect [59]. In fact, several case reports implicating selective COX2 inhibitors as an etiology of acute pancreatitis were described [60-63].
More recently however, a large multicenter prospective randomized double blind placebo controlled trial was conducted in which patients undergoing ERCP (n=602) were randomized to receive 100mg indomethacin rectally (n=295) immediately after ERCP or placebo (n=307), with PEP rates of 27/295 (9. 2%) vs 52/307 (16. 9%); respectively, p=0. 005 and moderate to severe PEP of 4. 5% vs. 8. 8%; respectively, p=0. 03 [54]. The majority of patients included in the study were high risk, with clinical suspicion of SOD, suggesting that the results are applicable to this patient population. While this was the first large multicenter trial to demonstrate that a single dose of rectally administered indomethacin provided immediately after ERCP reduced the risk of PEP, especially in the highest risk patient population, it may have underemphasized the role of concomitant prophylactic stenting of the PD [64].
Similar to the two previous meta-analyses, a larger metaanalysis of 10 RCTs [47-51, 53, 54, 57-59] involving a total of 2,269 patients demonstrated a relative risk of PEP of 0. 57 (95% CI, 0. 38-0. 86) after NSAID prophylaxis [65]. In this analysis, patients receiving NSAID’s were 43% less likely to experience PEP. The analysis further demonstrated a 54% reduction in the development of moderate to severe PEP. Moreover, peri-procedural NSAID use revealed no significant adverse events, thereby highlighting their relative safety at 1 or 2 doses. The metaanalysis; however, had limitations. Three low-quality trials [50, 53, 57] were included which are susceptible to bias, rending their results questionable. Further, three different kinds of NSAID’s were utilized in the included trials (diclofenac, indomethacin, and valdecoxib), with varying routes of administration and doses. Interestingly, the six studies assessing rectally administered NSAIDs were positive; whereas the four studies [51, 57-59] using oral, intravenous, intramuscular, and intraduodenal NSAIDs yielded negative results. Based on the limited studies, it would seem that rectally administered NSAIDs are the most effective for chemoprophylaxis. However, further studies are required to assess whether the route of administration plays a role in the prevention of postprocedure pancreatitis.
While rectal NSAID’s remain a convenient and effective therapy, the timing of NSAID administration remains a question. Previous clinic trials assessing the role for NSAID prophylaxis has included both pre-ERCP and post-ERCP drug administration [47-54, 60]. In a metaanalysis by Sethi et al. the timing of NSAID’s (pre vs post) demonstrated no difference in the efficacy of preventing PEP [66]. Post-ERCP administration appears to be the most logical; thereby, limiting unnecessary drug administration and targeting NSAID’s for higher risk patients.
A ROLE FOR NSAIDS VIS-A-VIS PD STENTING
Over the last decade, the use of temporary PD stenting and now NSAIDs have been shown to be effective for PEP prophylaxis. The most significant limitation in prior studies in assessing the true effect of NSAID prophylaxis has been the inability to accurately identify the rate of prophylactic pancreatic stents usage in the study populations. In their multicenter randomized trial, Elmunzer et al. identified that more than 80% of patients had PD stent placement in addition to indomethacin or placebo. Indomethacin conferred a similar reduction in the risk of PEP in both patients with and without PD stent placement: 16. 1% vs 9. 7% (p=0. 04) and 20. 6% vs6. 3% (p=0. 049), respectively [54]. This established the efficacy of NSAIDs for chemoprophylaxis in high-risk patients requiring PD stenting. PD stent placement remains technically demanding and costly, while the administration of NSAIDs is cost-effective and safe; making it an attractive alternative. A recent network meta-analysis performed both direct and indirect comparisons of rectal NSAIDs and PD stents to assess for the reduction of PEP [67]. The results demonstrated no significant benefit of rectal NSAIDs plus stents compared to NSAIDs alone (OR, 1. 46; 95% CI, 0. 79-2. 69). When rectal NSAIDs were compared to stents, the pooled analysis was positive for NSAIDs (OR, 0. 48; 95% CI, 0. 26 -0. 87). The clinical implications of these findings are significant and suggest that NSAIDs may offer a primary alternative to PD stent placement, especially in high-risk patients. However, given the limited number of studies involving high-risk patients and the inherent limitation of extrapolation in network meta-analysis, further randomized prospective trials are required to draw this conclusion confidently.
CONCLUSION
While prior attempts at pharmacologic prevention of post- ERCP pancreatitis have been disappointing, NSAIDs remain inexpensive, simple and safe to use. Given the most recent prospective multicenter trial and network meta-analysis demonstrating the efficacy of rectal indomethacin, the prophylactic administration of a single dose rectal NSAID will likely gain wider acceptance. Until then, further high quality RCTs are needed to better compare prophylactic rectal NSAIDs versus prophylactic PD stenting in average and high-risk patients.
Conflict of Interest
The authors did not report any potential conflicts of interest.
References
- Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, Moore JP, et al. Complications of endoscopic biliary sphincterotomy. N EnglJ Med. 1996; 335:909-918. [PMID:8782497]
- Pieper-Bigelow C, Strocchi A, Levitt MD. Where does serum amylase come from and where does it go? GastroenterolClin North Am. 1990; 19:793-810. [PMID:1702756]
- Freeman ML, DiSario JA, Nelson DB, Fennerty MB, Lee JG, Bjorkman DJ, OverbyCS,et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc. 2001; 54:425-434. [PMID:11577302]
- Christoforidis E, Goulimaris I, Kanellos I, Tsalis K, Demetriades C, Betsis D. Post-ERCP pancreatitis and hyperamylasemia: patient-related and operative risk factors. Endoscopy. 2002; 34:286-292. [PMID:11932783]
- Loperfido S, Angelini G, Benedetti G, Chilovi F, Costan F, De Berardinis F, De BernardinM,et al. Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastrointest Endosc. 1998; 48:1-10. [PMID:9684657]
- Masci E, Toti G, Mariani A, Curioni S, Lomazzi A, Dinelli M, Minoli G, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001; 96: 417-423. [PMID:11232684]
- Mariani A, Giussani A, Di Leo M, Testoni S, Testoni PA. Guidewire biliary cannulation does not reduce post-ERCP pancreatitis compared with the contrast injection technique in low-risk and high-risk patients. Gastrointest Endosc. 2012; 75:339-346. [PMID:22075192]
- Wang P, Li ZS, Liu F, Ren X, Lu NH, Fan ZN, Huang Q,et al. Risk Factors for ERCP-Related Complications: A Prospective Multicenter Study. Am J Gastroenterol. 2009; 104:31-40. [PMID:19098846]
- Cheng CL, Sherman S, Watkins JL, Barnett J, Freeman M, Geenen J, Ryan M, et al. Risk factors for post-ERCP pancreatitis: a prospective multicenter study. Am J Gastroenterol. 2006; 101:139-147. [PMID:16405547]
- DeBenedet AT, Raghunathan TE, Wing JW, Wamsteker E, and DimagnoMJ. Alcohol Use and Cigarette Smoking as Risk Factors for Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis. Clin Gastroenterol Hepatol. 2009; 7:353-8e4. [PMID:19168153]
- Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: a comprehensive review. Gastrointest Endosc. 2004; 59:845-864. [PMID:15173799]
- Choudhary A, Bechtold ML, Arif M, Szary NM, Puli SR, Othman MO, et al. Pancreatic stents for prophylaxis against post-ERCP pancreatitis: ameta-analysis and systematic review. Gastrointest Endosc. 2011; 73:275- 282. [PMID:21295641]
- Sofuni A, Maguchi H, Mukai T, Kawakami H, Irisawa A, Kubota K, Okaniwa S, et al. Endoscopic pancreatic duct stents reduce the incidence of post-endoscopic retrograde cholangiopancreatography pancreatitis in high-risk patients. Clin Gastroenterol Hepatol. 2011; 9:851-858. [PMID:21749851]
- Dumonceau JM, Andriulli A, Deviere J, Mariani A, Rigaux J, Baron TH, Testoni PA. European Society of Gastrointestinal Endoscopy (ESGE) Guideline: prophylaxis of post-ERCP pancreatitis. Endoscopy. 2010; 42:503-515. [PMID:20506068]
- Bakman YG, Safdar K, Freeman ML. Significant clinical implications of prophylactic pancreatic stent placement in previously normal pancreatic ducts. Endoscopy. 2009; 41:1095-1098. [PMID:19904701]
- Murray WR. Reducing the incidence and severity of post ERCP pancreatitis. Scand J Surg. 2005; 94:112-6. [PMID:16111092]
- Johnson GK, Geenen JE, Bedford RA. A comparison of nonionic versus ionic contrast media: results of a prospective, multicenter study. Midwest Pancreaticobiliary Study Group. Gastrointest Endosc. 1995; 42:312-316. [PMID:8536898]
- Sherman S, Hawes RH, Rathgaber SW, Uzer MF, Smith MT, Khusro QE, Silverman WB, et al. Post-ERCP pancreatitis: Randomized, prospective study comparing a low- and high-osmolality contrast agent. Gastrointest Endosc. 1994; 40:422-427. [PMID:7926531]
- Pezzilli R, Romboli E, Campana D, Corinaldesi R. Mechanisms Involved in the Onset of Post-ERCP Pancreatitis. JOP. 2002; 3:162-168. [PMID:12432182]
- Ogawa M, Kawaguchi Y, Kawashima Y, Mizukami H, Maruno A, Ito H, Mine T. Comparison of ionic, monomer, high osmolar contrast media with non-ionic, dimer, iso-osmolar contrast media in ERCP. Tokai J Exp Clin Med. 2013; 38:109-113. [PMID:24030487]
- Koike H, Steer ML, Meldolesi J. Pancreatic effects of ethionine: blockade of exocytosis and appearance of crinophagy and autophagy precede cellular necrosis. Am J Physiol. 1982; 242:G297-307. [PMID:7065251]
- Saluja AK, Donovan EA, Yamanaka K, Yamaguchi Y, Hofbauer B, Steer ML. Cerulein-induced in vitro activation of trypsinogen in rat pancreatic acini is mediated by cathepsin B. Gastroenterology. 1997; 113:304-310. [PMID:9207291]
- Granger J, Remick D. Acute Pancreatitis: models, markers, and mediators. Shock 2005; 24:45-51. [PMID:16374372]
- Vane JR. Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nat New Biol. 1971; 231:232-236. [PMID:5284360]
- Lee SH, Soyoola E, Chanmugam P, et al. Selective expression of mitogen-inducible cyclooxygenase in macrophages stimulated with lipopolysaccharide. J Biol Chem 1992; 267:25934-25938. [PMID:1464605]
- Zabel-Langhenning A, Holler B, Engeland K, Mossner J. Cyclooxygenase-2 transcription is stimulated and amylase secretion is inhibited in pancreatic acinar cells after induction of acute pancreatitis. BiochemBiophys Res Commun 1999; 265:545-549. [PMID:10558906]
- Vollmar B, Waldner H, Schmand J, Conzen PF, Goetz AE, Habazettl H, Schweiberer L, et al. Release of arachidonic acid metabolites during acute pancreatitis in pigs. Scand J Gastroenterol. 1989; 24:1253-1264. [PMID:2602907]
- Ethridge RT, Chung DH, Slogoff M, Ehlers RA, Hellmich MR, Rajaraman S, Saito H, et al. Cyclooxygenase-2 gene disruption attenuates the severity of acute pancreatitis and pancreatitis-associated lung injury. Gastroenterology. 2002; 123:1311-1322. [PMID:12360491]
- Foitzik T, Hotz HG, Hotz B, Wittig F, Buhr HJ. Selective inhibition of cyclooxygenase-2 (COX-2) reduces prostaglandin E2 production and attenuates systemic disease sequelae in experimental pancreatitis. Hepatogastroenterology. 2003; 50:1159-1162. [PMID:12846004]
- O'Brien G, Shields CJ, Winter DC, Dillon JP, Kirwan WO, Redmond HP. Cyclooxygenase-2 plays a central role in the genesis of pancreatitis and associated lung injury. Hepatobiliary Pancreat Dis Int. 2005; 4:126- 129. [PMID:15730936]
- Seo SW, Jung WS, Piao TG, Hong SH, Yun KJ, Park RK, Shin MK, et al. Selective cyclooxygenase-2 inhibitor ameliorates cholecystokinin-octapeptide-induced acute pancreatitis in rats. World J Gastroenterol. 2007; 13:2298-2304. [PMID:17511027]
- Dennis EA, Cao J, Hsu YH, Magrioti V, Kokotos G. Phospholipase A2 enzymes: physical structure, biological function, disease implication, chemical inhibition, and therapeutic intervention. Chem Rev. 2011; 111:6130-6185. [PMID:21910409]
- Uhl W, Schrag HJ, Schmitter N, Nevalainen TJ, Aufenanger J, Wheatley AM, Büchler MW. Pathophysiological role of secretory type I and II phospholipase A2 in acute pancreatitis: an experimental study in rats. Gut. 1997; 40:386-392. [PMID:9135530]
- Kihara Y, Yoshikawa H, Honda H, Fukumitsu K, Yamaguchi T, Otsuki M. Natural disruption of group 2 phospholipase A2 gene protects against choline-deficient ethionine-supplemented diet-induced acute pancreatitis and lung injury. Pancreas. 2005; 31:48-53. [PMID:15968247]
- Büchler M, Malfertheiner P, Schädlich H, Nevalainen TJ, Friess H, Beger HG. Role of phospholipase A2 in human acute pancreatitis. Gastroenterology. 1989; 97:1521-1526. [PMID:2684722]
- Gronroos JM, Nevalainen TJ. Increased concentrations of synovial-type phospholipase A2 in serum and pulmonary and renal complications in acute pancreatitis. Digestion. 1992; 52:232-236. [PMID:1459357]
- Mäkelä A, Kuusi T, Schröder T. Inhibition of serum phospholipase-A2 in acute pancreatitis by pharmacological agents in vitro. Scand J Clin Lab Invest. 1997; 57:401-407. [PMID:9279965]
- Díaz-González F, Sánchez-Madrid F. Inhibition of leukocyte adhesion: an alternative mechanism of action for anti-inflammatory drugs. Immunol Today. 1998; 19:169-72. [PMID:9577093]
- González-Alvaro I, Carmona L, Díaz-González F, González-Amaro R, Mollinedo F, Sánchez-Madrid F, Laffón A, et al. Aceclofenac, a new nonsteroidalantiinflammatory drug, decreases the expression and function of some adhesion molecules on human neutrophils. J Rheum. 1996; 23:723-972. [PMID:8730134]
- Díaz-González F, González-Alvaro I, Campanero MR, Mollinedo F, del Pozo MA, Muñoz C, Pivel JP, et al. Prevention of in vitro neutrophil-endothelial attachment through shedding of L-selectin by nonsteroidalantiinflammatory drugs. J Clin Invest. 1995; 95:1756-6175. [PMID:7535797]
- Lefkovits J, Plow EF, Topol EJ. Platelet glycoprotein IIb/IIIa receptors in cardiovascular medicine. N Engl J Med. 1995; 332:1553-1559. [PMID:7739710]
- Dominguez-Jimenez C, Diaz-Gonzalez F, Gonzalez-Alvaro I, Cesar JM, Sanchez-Madrida F. Prevention of aII(b)ß3 activation by non-steroidal antiinflammatory drugs. FEBS Letters. 1999; 446:318-322. [PMID:10100866]
- Garcia-Vicuna R, Diaz-Gonzalez F, Gonzalez-Alvaro I. Prevention of cytokine-induced changes in leukocyte adhesion receptors by nonsteroidalantiinflammatory drugs from the oxicam family. Arthritis Rheum. 1997; 40:143-153. [PMID:9008610]
- Gerli R, Paolucci C, Gresele P, Bistoni O, Fiorucci S, Muscat C, Belia S, et al. Salicylates inhibit adhesion and transmigration of T lymphocytes by preventing integrin activation induced by contact with endothelial cells. Blood. 1998; 92:2389-2398.
- Lankisch PG, Koop H, Winckler K, Kunze H, Vogt W. Indomethacin treatment of acute experimental pancreatitis in the rat. Scand J Gastroenterol. 1978; 13:629-633. [PMID:705258]
- Ebbehøj N, Friis J, Svendsen LB, Bülow S, Madsen P. Indomethacin treatment of acute pancreatitis. A controlled double-blind trial. Scand J Gastroenterol. 1985; 20:798-800. [PMID:2413519]
- Murray B, Carter R, Imrie C, Evans S, O'Suilleabhain C. Diclofenac reduces the incidence of acute pancreatitisafter endoscopic retrograde cholangiopancreatography. Gastroenterology. 2003; 124:1786-1791. [PMID:12806612]
- Sotoudehmanesh R, Khatibian M, Kolahdoozan S, Ainechi S, Malboosbaf R, Nouraie M. Indomethacin may reduce the incidence and severity of acute pancreatitis after ERCP. Am J Gastroenterol. 2007; 102:978-983. [PMID:17355281]
- Khoshbaten M, Khorram H, Madad L, EhsaniArdakani MJ, Farzin H, Zali M. Role of diclofenac in reducing post-endoscopic retrograde cholangiopancreatography pancreatitis. J Gastroenterol Hepatol. 2008; 23:e11-6. [PMID:17683501]
- MontañoLoza A, Rodríguez Lomelí X, García Correa JE, DávalosCobián C, Cervantes Guevara G, Medrano Muñoz F, Fuentes Orozco C, et al. Effect of the administration of rectal indomethacin on amylase serum levels after endoscopic retrograde cholangiopancreatography, and its impact on the development of secondary pancreatitis episodes. Rev Esp Enferm Dig. 2007; 99:330-336. [PMID:17883296]
- Cheon YK, Cho KB, Watkins JL, McHenry L, Fogel EL, Sherman S, Schmidt S. Efficacy of diclofenac in the prevention of post-ERCP pancreatitis in predominantly high-risk patients: a randomized double-blind prospective trial. Gastrointest Endosc. 2007; 66:1126-1132. [PMID:18061712]
- Katsinelos P, Fasoulas K, Paroutoglou G, Chatzimavroudis G, Beltsis A, Terzoudis S, Katsinelos T, et al. Combination of diclofenac plus somatostatin in the prevention of post-ERCP pancreatitis: a randomized, double-blind, placebo-controlled trial. Endoscopy. 2012; 44:53-59. [PMID:22198776]
- Otsuka T, Kawazoe S, Nakashita S, Kamachi S, Oeda S, Sumida C, Akiyama T, et al. Low-dose rectal diclofenac for prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis: a randomized controlled trial. J Gastroenterol. 2012; 47:912-917. [PMID:22350703]
- Elmunzer BJ, Scheiman JM, Lehman GA, Chak A, Mosler P, Higgins PD, Hayward RA, et al. A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012; 366:1414-1422. [PMID:22494121]
- Elmunzer BJ, Waljee AK, Elta GH, Taylor JR, Fehmi SM, Higgins PD. A meta-analysis of rectal NSAIDs in the prevention of post-ERCP pancreatitis. Gut. 2008; 57:1262-1267. [PMID:18375470]
- Dai HF, Wang XW, Zhao K. Role of nonsteroidal anti-inflammatory drugs in the prevention of post-ERCP pancreatitis: a meta-analysis. Hepatobiliary Pancreat Dis Int. 2009; 8:11-16. [PMID:19208508]
- Senol A, Saritas U, Demirkan H. Efficacy of intramuscular diclofenac and fluid replacement in prevention of post-ERCP pancreatitis. World J Gastroenterol. 2009; 15:3999-4004. [PMID:19705494]
- Elmi F RF, Lim JK, et al. A Prospective, Multicenter, Randomized, Double Blinded Controlled Study to Determine Whether A Single Dose of Intraduodenal Indomethacin Can Decrease the Incidence and Severity of Post-ERCP Pancreatitis. Gastrointest Endosc. 2010:AB232.
- Bhatia V, Ahuja V, Acharya SK, Garg PK. A randomized controlled trial of valdecoxib and glyceryltrinitrate for the prevention of post-ERCP pancreatitis. J ClinGastoenterol. 2011; 45:170-176. [PMID:20717044]
- Mennecier D, Ceppa F, Sinayoko L. Acute pancreatitis after treatment by celecoxib. Gastroenterol Clin Biol. 2007; 31:668-669. [PMID:17925765]
- Nind G, Selby W. Acute pancreatitis: a rare complication of celecoxib. Intern Med J. 2002; 32:624-625. [PMID:12512760]
- Amaravadi RK, Jacobsen BC, Solomon DG, Fishcr MA. Acute pancreatitis associated with rofecoxib. Am J Gastroenterol. 2002; 97:1077-1078. [PMID:12003405]
- Carrillo-Jimenez R, Nurnberger M. Celecoxib-induced acute pancreatitis and hepatitis: a case report. Arch Intern Med. 2000; 160:553- 554. [PMID:10695699]
- Baron TH, Abu Dayyeh BK, Zinsmeister AR. Rectal indomethacin to prevent post-ERCP pancreatitis. N Engl J Med. 2012; 367:277-278. [PMID:22808973]
- Ding X, Chen M, Huang S, Zhang S, Zou X. Nonsteroidal anti-inflammatory drugs for prevention of post-ERCP pancreatitis: a meta-analysis. Gastrointest Endosc. 2012; 76:1152-1159. [PMID:23164513]
- Sethi S, Sethi N, Wadhwa V, Garud S, Brown A. A meta-analysis on the role of rectal diclofenac and indomethacin in the prevention of post-endoscopic retrograde cholangiopancreatography pancreatitis. Pancreas. 2014; 43:190-197. [PMID:24518496]
- Akbar A, Abu Dayyeh BK, Baron TH, Wang Z, Altayar O, Murad MH. Rectal nonsteroidal anti-inflammatory drugs are superior to pancreatic duct stents in preventing pancreatitis after endoscopic retrograde cholangiopancreatography: a network meta-analysis. Clin Gastroenterol Hepatol. 2013; 11:778-783. [PMID:23376320]

