Keywords
Multiple Organ Failure; Pancreatitis
Limitations of the Original Atlanta Classification
In 1992, 41 recognized experts in acute pancreatitis (AP) from all over the world finalized Atlanta classification (Original Atlanta Classification, OAC) which provided clear definitions of the disease and simplified the terminology [1]. However, these definitions of severity and local complications received considerable criticism over the subsequent two decades [2]. It came to be recognized that mere presence of organ failure (OF) did not determine the morbidity and mortality of AP; rather it was the persistence of OF which mattered most. Secondly, it was realized that prognostication of severity needed to be simplified. Thirdly, the interpretation of fluid collections like the pseudocyst and pancreatic abscess varied widely. There was poor inter-observer agreement on morphological criteria to define them that needed to be rectified.
The Revised Atlanta Classification
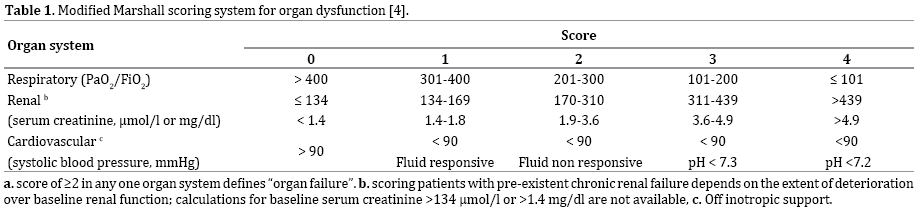
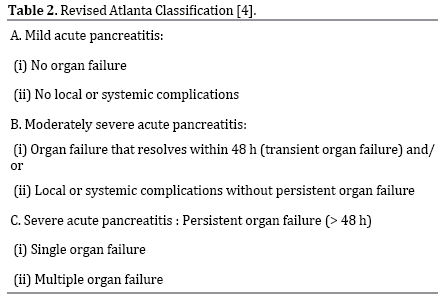
In the ensuing years after the OAC, various revisions of it were suggested as well as debated. The revisions of OAC and definitions have been updated recently as the revised Atlanta classification (RAC) [4] according to which the diagnosis of AP requires two of the following three features: (1) abdominal pain consistent with acute pancreatitis; (2) serum lipase activity (or amylase activity) at least three times greater than the upper limit of normal; and (3) characteristic findings of acute pancreatitis on contrast-enhanced computed tomography (CECT) and less commonly magnetic resonance imaging (MRI) or transabdominal ultrasonography [4]. This classification redefines severity of AP into 3 categories mild, moderate and severe, and also morphologically describes fluid collections occurring following AP [4]. In addition, based on the CECT criteria, 2 distinct types of AP: acute interstitial edematous pancreatitis and acute necrotizing pancreatitis (ANP) have been described. ANP is further subdivided into pancreatic parenchymal necrosis alone, peripancreatic necrosis alone and pancreatic parenchymal and peripancreatic necrosis [4, 5]. The classification of severity is primarily based on presence of organ failure (OF) which is assessed by modified Marshall scoring system (Table 1), and local or systemic complications (exacerbation of co-morbid conditions) (Table 2). Severe AP is characterized by persistent OF which is indicated by presence and persistence of systemic inflammatory response syndrome (SIRS). Persistent OF may involve a single or multiple organs and such patients usually have one or more local complications. These patients are at an increased risk of death, with a mortality reported as high as 36–50% [4, 6]; which may increase further with the development of infected necrosis [7, 8].
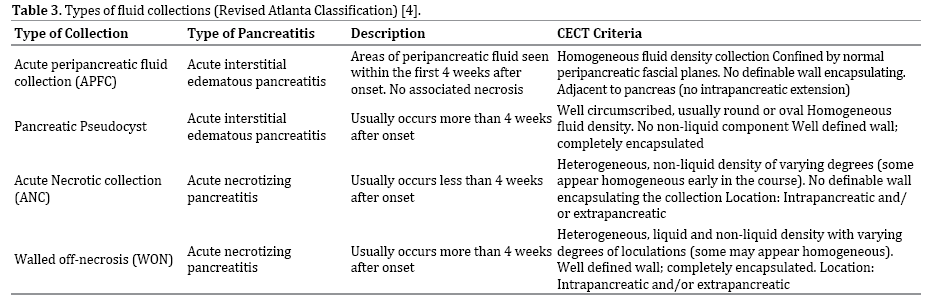
In RAC, the description of the fluid collections and their terminology has been made precise and it provides the standardization that had been a source of controversy in the past few years (Table 3) [1, 4, 10-11]. Following this defined nomenclature, there is bound to be a better appreciation of the disease course and sequelae thereof. In addition, the RAC advocates the use of SIRS status which offers important prognostic information as increasing SIRS criteria during the initial 24 hours of hospitalization have an increased risk of persistent OF, necrosis as well as mortality [6, 9].
Thus, RAC has provided us with uniformity in nomenclature including radiologic descriptions of pancreatic and peripancreatic fluid collections. It has given due importance to OF especially in the early phase of the illness, knowledge of which has emerged as the key determinant of outcome. The exact description of local complications including their sequence of development is likely to help the clinician in optimizing treatment strategies.
Have We Reached Near an Ideal Classification? or Is It a Work-In-Progress?
It had taken 2 decades for the OAC to be revised to RAC. However with application of the RAC into clinical practice, its limitations had started to get recognized. Over the last two decades there has been better understanding of the disease process, improvements in imaging techniques and rapid advancements in patient care. As more data emerge and the complexities of the spectrum of acute pancreatitis unfold, key concepts are likely to get revised. Thus it is not surprising that questions have been raised about the completeness of the RAC. It is likely that the classification will need to be updated continuously till we reach the utopian goal of perfection. Some of the shortcomings of the RAC are reviewed below.
Infected Pancreatic Necrosis: Is It Getting the Importance Due To It?
The RAC has not given due consideration to infected necrosis (IN) while classifying severity into mild, moderate and severe. It does however mention that the presence of infection within areas of necrosis is a marker of increased risk of death, and IN and persistent OF together have higher mortality. However the presence or absence of IN does not count in classifying patients as moderate or severe AP.
The importance of infection of pancreatic necrosis as an adverse prognostic factor was first reported by Beger et al. [12] who showed that the contamination rate was 23.8% in patients operated in the first week which increased to 71.4% in the third week. Intra- and extra pancreatic necrosis were more widespread and frequent in patients with proven contamination with a postoperative mortality of 37.8% in patients with IN versus 9% in sterile necrosis (SN). Similarly Bradley and Allen [13] and Fedorak et al. [14] demonstrated increased mortality in patients with IN in their retrospective studies. Tenner et al. [15] observed that though there was no difference in development of OF with respect to IN but the death rate was higher in patients with IN.
The interplay between IN and OF was also studied by Isenmann et al. [16] who noticed that OF was more frequent in patients with IN than in those with SN. Similar observations were made by Buchler et al. [17] and Mee et al. [18] who found that patients with IN had OF more often, and had and higher mortality compared to those with SN. Perez et al. [19] on the other hand reported that patients with pancreatic necrosis and/or IN did not have increased prevalence of OF or IN but did hasve an increased mortality rate associated with multiple OF. Other studies have also supported the contention that IN affects survival and occurrence of OF [20-23].
Petrov et al. [24] in their systematic review on AP found that patients with both OF and IN had 2 times higher risk of death in comparison with patients with OF and no IN and patients with IN and no OF. A mortality rate of 30% was seen in patients with OF, regardless of the presence or absence of IN, while in the presence of IN, regardless of the presence or absence of OF, there was a mortality of 32%. This underlines the importance of both the entities. Subgroups of patients with both OF and IN have a substantially higher mortality and both OF and IN are probably equivalent determinants of severity. Patients with both OF and IN together had more severe disease and a higher mortality rate (43%). Similar findings were also reported in a Dutch study [25]. A recent study by Choi et al. [26] showed that patients with severe AP with IN had greater need for ICU care, had longer duration of ICU stay and total hospital stay along with increased inhospital mortality compared with those without IN. They have suggested that for more precise evaluation of clinical outcomes of patients with SAP defined by the RAC, SAP patients with IN should be considered separately from those without IN in severity classification [26]. Although infection of pancreatic necrosis occurs increasingly with increasing duration of the disease, interestingly, a substantial proportion (11-29%) of patients develop IN within the first 7-14 days which may have a bearing on the course and management of the illness [12, 24, 27-32].
These studies exemplify the role of infection in determining the outcome of AP. Thus there is a need to distinguish infected from non-infected necrosis. Severity stratification, therefore must factor infection of the pancreatic necrosis.
Dynamic Nature of Organ Failure in Acute Pancreatitis
Persistence of OF has been given a pivotal role in the RAC in defining the severity of AP. However, the RAC does not give due consideration to the dynamic nature of the OF, whether there is ongoing worsening or improvement in individual OF over a period of time. The magnitude of OF in terms of number of OF has also not been given due importance. Buter et al. [33] showed that deteriorating OF was an independent determinant of mortality in patients with AP. Johnson et al. [34] also showed that the duration of OF during the first week of predicted severe AP was strongly associated with the risk of death or local complications. Data from a study by Lankisch et al. [35] also give support to the concept of dynamic nature of OF. They showed that one third of patients with initial OF would have deterioration of OF as compared to only 7% of those who had no OF in the early course of the disease. We also recently reported that patients with persistent and deteriorating OF had 5 times higher mortality as compared to those who had only persistent OF [36].
Sharma et al. [37] reported the dynamic nature of the organ failure in a large study wherein patients with severe pancreatitis were divided into early severe OF within 7 days of pancreatitis (ESAP) and late severe AP. Among the patients with OF, 64% had single OF and 36% had multiorgan failure (MOF), which increased to 63% during hospitalization with increasing mortality. In a study from our centre, OF was present in more than half the patients among whom about half had single OF, one third had two OF and one fifth had had MOF [38]. Importantly increasing mortality rates were noted with increasing number of OF, approaching 100% with MOF [38]. In view of the difference in outcomes of those with single OF and those with MOF; categorizing them into a separate severity category may be useful.
Secondly the RAC is based on the concept of a biphasic natural course of AP and uses a different method of classification for the early phase and the late phase of AP [4]. In the early phase of the disease, the classification of severity is to be based on the presence or absence of persistent OF and in the late phase, it is to be based on the different morphologic characteristics of local complications evaluated by radiologic imaging and the need for active intervention there of (operative, endoscopic, laparoscopic, or percutaneous) or other supportive measures (such as need for respiratory ventilation or renal dialysis), as well as on the presence or absence of persistent OF. However, Mole et al. [39] demonstrated no apparent bimodal distribution of severe disease occurring early in the course of the disease. Thus the concept of a biphasic natural course of AP may be questionable [7].
The Role of Extra Pancreatic Necrosis in Determining Severity of Acute Pancreatitis
An interesting facet of this illness, which was lacking in the OAC and has been recognized by RAC, is the presence of extrapancreatic necrosis (EXPN). In the OAC, necrotizing pancreatitis was defined as diffuse or focal area(s) of nonviable pancreatic parenchyma typically associated with extra pancreatic fat necrosis or non-enhanced pancreatic parenchyma >3 cm in length or involving >30% of the area of the pancreas [1]. This definition did not include patients with EXPN. EXPN is defined as “extra pancreatic morphological changes exceeding fat stranding with complete enhancement of the pancreatic parenchyma without signs of focal or diffuse non-enhancement” [4]. The RAC has recognized EXPN as an important component of morphology but has not taken into account its impact on course of the disease.
There are conflicting reports about implications of EXPN in the management and outcome of AP [40-42]. Bakker et al. [40] found that patients with EXPN less frequently suffered from complications like persistent OF and IN. These patients also had decreased need for intervention and had lower mortality. They however suggested that patients with EXPN need extra consideration during necrosectomy to avoid iatrogenic pancreatic injury. Singh et al. [41] while evaluating patients with interstitial pancreatitis (IP) noted that patients with EXPN had greater levels of disease severity, compared to patients with IP. In a recent study by Rana et al. [42], about one fourth of the study patients had EXPN alone that was found to have higher frequency of organ failure than patients with IP. They also noted that patients with widespread EXPN had appreciably higher frequency of pleural effusion, ascites and multi-organ failure, but similar outcome as patients with limited EXPN. Interestingly, Heiss et al. [43] found certain CT features which exhibited a significant correlation with mortality. Among these were the incidence of distant fluid collections (posterior pararenal space and/or paracolic gutter) wherein the mortality was doubled. They also noted that presence of fluid collections in the left posterior pararenal space was significantly associated with increased mortality [43].
It thus seems that EXPN may need to be considered as a separate entity. It could have implications in prognostication and management. Prospective studies on these issues could help us understand the importance of EXPN better
Extra Pancreatic Infection (EPI): Does it Make a Difference?
The RAC has not considered the role of EPIs in the outcome of AP. The importance of EPIs and their effect on the outcome of AP have been highlighted by various studies. Garg et al. [44] detected extra pancreatic bacterial infections in 31.7% of their patients having evidence of ongoing or worsening pancreatitis. The most common organisms isolated were Escherichia coli and Pseudomonas aeruginosa. Similarly, Bourgaux et al. [45] reported EPIs in 25% of their patients, most common sites of infection being the peritoneal fluid, blood, respiratory tract and urinary tract. Besselink et al. [46] reported that the initial infection in patients with AP was diagnosed a median of 8 days after admission (in contrast to diagnosis of IN, median day 26; bacteremia/pneumonia, median day 7) and 80% patients who died had an infection. They also reported that in patients with pancreatic parenchymal necrosis, bacteremia was associated with increased risk of IN and was associated with higher mortality.
We in a prospective study also found that the number of EPIs was significantly higher than pancreatic infections with no association between the presence of the two infections [47]. Mortality was nearly double in patients with EPIs as compared to patients without them. It was suggested that in addition to pancreatic infections, early detection and treatment of EPIs may positively affect patient outcome. In a recent study by Cacopardo et al. [48] a higher complication rate and mortality were noted among patients with systemic infection (positive blood cultures) than those who only had a localized infection. Rao et al. [49] also reported occurrence of EPIs in about 15% patients with AP. They noted that persistent OF, length of hospital stay and mortality was higher when compared with sterile group.
Thus, to say the least, EPIs have a significant bearing on the outcome of AP as they are associated with OF, longer hospital stay and higher mortality. It needs to be determined how this can be included in RAC.
Local Complications: What More?
While a majority of the extra pancreatic complications have been included in RAC [4], a few that may have important bearing on the outcome of AP have not been considered. These include fistulization [50-57] and vascular complications other than splanchnic thrombosis [58-64]. Gastrointestinal tract fistulization due to pancreatitis has a major impact on both clinical and surgical outcome. While most of the older studies had reported that fistulization in patients with AP generally occurred after surgical or radiological intervention [50, 51, 54]; recent data suggest that it can occur spontaneously as well [52, 53]. Tsiotos et al. [50] in one of the early studies on the issue had reported that most pancreatic fistulae related to AP were external and occurred after surgery or radiological intervention. One third of their patients had enteric fistulae, with the colon being the most common site. Doberneck [51] reported development of intestinal fistulae in about half of their patients with necrotizing pancreatitis, again more often after an intervention. Mohamed with Siriwardena [54] reported frequent occurrence of colonic complications in severe AP, with 15% of patients presenting with necrosis, fistulae and stricture. While colonic necrosis has been considered in the RAC, necrosis and fistulization of other sites has not been given due recognition. Enteric fistulae in patients with AP can occur spontaneously as well. In our study of 289 patients we identified 12 patients with fistulae (none had undergone surgery prior to detection of fistula); duodenum was the most common site, followed by stomach and colon [52]. We have also observed that among patients with fistulization, those with colonic fistulae and those presenting with bleeding have higher mortality.
Vascular complications like arterial and venous thrombosis and pseudo-aneurysms can also adversely affect the outcome of AP. However the RAC has taken into account only splanchnic thrombosis [4]. The frequency of fatal hemorrhagic complications of pancreatitis varies between 1.2% and 14.5%, and these complications seem to be related to the severity of disease [58]. Importantly, gastrointestinal bleeding was a component of severe AP as per OAC; the RAC has not included it for defining the severity of AP. Flati et al. [59] found that about one third of their patients died if severe bleeding occurred following AP. Also noteworthy was the frequent association of severe necrosis with massive hemorrhage and a high mortality rate in their study [59]. Balachandra and Siriwardena [60] in their systematic review identified two categories of patients one having spontaneous bleeding likely from a pseudo-aneurysm with 31% mortality and the other with post-operative bleeding with 55% mortality.
Splanchnic vein thrombosis (SVT) is seen in 1-24% of patients with AP and has been mentioned by the RAC as a local complication [4]. Besselink [63] explained the importance of this complication in the management of IN by pre-operative identification of splenomegaly, major collaterals or varices to avoid a left-sided minimally invasive approach. In a recent review, Nadkarni et al. [64] have mentioned safe use of anticoagulation in the management of splanchnic as well as nonsplanchnic (deep venous thrombosis or pulmonary venous) thrombosis in patients with AP without added mortality.
Therefore despite being relatively less common, gastrointestinal fistulization and bleeding need to be recognized as serious complications with a high morbidity and mortality. They may need to be included as local complications like splanchnic vascular thrombosis.
Moderately Severe Acute Pancreatitis: A Very Wide Basket
The RAC mentions a new severity category of moderately severe acute pancreatitis (MSAP), which is worse than mild AP but better than severe AP [4]. It mandates the presence of transient OF and/or presence of local or systemic complications [4]. However the bags of local and systemic complications are rather mixed [65]. As per the RAC, systemic complications are defined as ‘exacerbation of coexisting disease’. The question arises: whether the exacerbation of a coexisting disease is a cause or consequence of AP. A preexisting co morbidity like hyperlipidemia may be causal while age >65 or obesity may be poor prognostic factors per se [66]. Yet AP can exacerbate diabetes mellitus, chronic obstructive airways disease, cardiovascular compromise or renal insufficiency. The number of co-morbidities also needs to be taken into account [41, 66].
While the need to include the category of MSAP was rightly based on data provided by studies from Mayo Clinic [67, 68]; the inclusion of fluid collection(s) as a local complication in categorizing MSAP has been criticized [65]. The morphological category of acute peripancreatic fluid collections (APFC) is often a harmless accompaniment of interstitial pancreatitis of generally no consequence [4]. Therefore using APFC to categorize MSAP may upgrade the severity erroneously. Moreover as Lerch has pointed out, as per the RAC, whether the fluid is mere fluid or pus is now immaterial [65]. Therefore innocuous APFC cannot be equated with infected fluid collection(s).
Currently the RAC classifies a very broad and heterogeneous group of patients as having MSAP. As pointed out in the preceding text the category of MSAP needs to be better defined.
(Re)Classifying Acute Pancreatitis: How Many Classifications?
The RAC only considers one clinically applicable variable to define severe AP which is persistent OF [4]. On the other hand, presence of data demonstrates the larger spectrum of clinically relevant changes in AP such as (peri) pancreatic complication (absent, sterile, infectious) and OF (absence, transient, persistent) [7]. Recognition of these variables prompted the classification of severity into four categories by Windsor and Petrov [7] (Table 3). Talukdar and Vege [69], on the other hand, utilized the categorization of OF into early and late to propose a 5-tier classification which took into account the dynamics of the disease and also included infection as a key determinant. Sharma et al. [37] had suggested a classification based on timing of onset of OF, classifying patients in to fulminant and subfulminant AP. However before these classifications could be validated two new classification systems including the RAC were proposed [4, 7].
Dellinger et al. [70] proposed an International Multidisciplinary Consultation Determinant-Based Classification (DBC) for severity of AP based on the factors called “determinants” which are both local and systemic. The local determinant of severity is necrosis of the pancreas and/or peripancreatic tissue and the systemic determinant is a certain distant organ dysfunction, covered by the term OF (Table 4). The determinant based classification (DBC) was validated earlier by us in a prospectively analyzed data [71]. The mortality in critical AP was almost double of severe AP with low mortality with moderate AP and none with mild AP.

Following our validation of DBC, 2 recent studies have compared RAC and DBC [72, 73]. Nawaz et al. [72] found that the DBC performed better in predicting need for intervention, whereas RAC performed better in predicting hospital stay. Petrov et al. [74] using a score validated metric net reclassification improvement (NRI), reconstructed the data provided in our study [71] and concluded that the DBC scored over the OAC and the RAC, as the DBC recognizes AP being a complex and dynamic disease rather than based on a 2-phase (early and late) model of AP. In a recent editorial by Yadav [75] the issue of too many classifications was aptly summarized. He commented that DBC appears to develop the scope of the RAC further by creating severity categories that are based on the primary determinants of mortality in AP that closely match the implied basis of RAC. The application of RAC appears to be more relevant to the day-to-day clinical care of patients as classifying patients into categories is simpler than with DBC because it is not reliant on (early) contrast-enhanced CT.
The Optimum Imaging Technique for Assessment of Fluid Collections
The RAC recommends high resolution contrast-enhanced computed tomography (CECT) as the investigation to diagnose pancreatic/peripancreatic necrosis and to categorize fluid collections. However, an early CECT may not define precisely the presence and extent of pancreatic and peripancreatic necrosis [4]. Nevertheless, CECT should be performed in patients who develop or are likely to develop SAP or complications [76]. Performing a CECT 5–7 days after admission is more consistent in establishing the incidence and extent of pancreatic necrosis [4]. It should be repeated in case of clinical deterioration, decrease in hematocrit, or sepsis. CECT is also useful for percutaneous intervention and for assessment of successful treatment [76].
A number of workers have highlighted that CECT may not be the best imaging modality to diagnose solid and liquid components of WON or pseudocyst [65, 77]. The RAC mentions the use of magnetic resonance imaging (MRI), transabdominal ultrasonography or endoscopic ultrasonography for confirming solid content in the collections [4]. There is emerging data on the role of EUS to differentiate the amount of solid necrotic debris in the collection having management implications. Rana et al. [78] in a retrospective analysis found that patients with symptomatic WON having <10% necrotic debris needed only single session of endoscopic drainage, whereas patients with 10-40% solid debris needed two or more sessions and with > 40% debris required direct endoscopic debridement or surgical necrosectomy. This area also needs further prospective evaluation.
Despite the known limitations of CECT, it still remains the modality of choice in view of the recent well defined morphological characteristics by RAC and its wide availability. However there is a need to study the role of other imaging modalities especially in selecting management options.
Unresolved Issues: Dynamic Disease: Dynamic Terminology
It thus seems that while the RAC is a valiant attempt at categorizing AP, especially as it revised a 20 year old classification; it has thrown many new questions. We need prospective studies on dynamics of OF, correct categorization or sub categorization of moderately severe AP, reviewing the need to confirm IN, implications of characterizing fluid collections and extrapancreatic necrosis besides optimizing the imaging techniques. Though the RAC desists from the need of carrying out fine needle aspiration to diagnose IN, it still talks of classifying fluid collections as infected/non-infected. As we have recently shown that infection of fluid collections can be diagnosed non-invasively using labeled leucocytes and Positron Emission Tomography [79], and recently diffusion-weighted magnetic resonance imaging (DWMRI) has been used in the detection of infection in fluid collections [80]. There is a suggestion that other paradigms may also need to be reviewed [80, 81, 82].
Conclusion
To conclude, the revised Atlanta classification (RAC) has precisely defined the diverse facets of this versatile illness with a few caveats as we have endeavored to portray. As the accompanying editorial with the publication of RAC had admitted, that “many aspects remain debatable, particularly in areas where published data are scarce, and thus now require verification and validation in prospective clinical trials” [81]. Recently Garg and Imrie [82] have emphasized on the early severe group and infected pancreatic necrosis for prognostication of AP; whereas Windsor et al. [83] have reflected upon the perspective of developments in care of patients of AP in different settings requiring better methods for predicting and classifying severity as well as the discovery of accurate biomarkers of severity.
Thus, the emphasis on the way forward in classifying the severity of AP is a continuous as well as a dynamic process. There is always a scope to enhance the functionality besides the practicality of a classification; with the various advancements in all fields encompassing this illness amendments are mandated in due course of time.
Conflicting Interest
The authors had no conflicts of interest.
References
- Bradley EL III. A clinically based classification system for acute pancreatitis.Summary of the International Symposium on Acute Pancreatitis, Atlanta, GA, September 11 through 13, 1992.Arch Surg 1993; 128: 586-590. [PMID: 8489394]
- Bollen TL, van Santvoort HC, Besselink MG, van Leeuwen MS, Horvath KD, Freeny PC, et al. The Atlanta Classification of acute pancreatitis revisited. Br J Surg 2008; 95: 6-21. [PMID: 17985333]
- McKay CJ, Imrie CW. Staging of acute pancreatitis. Is it important? SurgClin North Am 1999; 79: 733-743. [PMID: 10470323]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62:102-111. [PMID: 23100216]
- Acute Pancreatitis Classification Working Group. Revision of the Atlanta classification of acute pancreatitis.2008. www.pancreasclub.com/resources/AtlantaClassification.pdf .
- Mofidi R, Duff MD, Wigmore SJ, Madhavan KK, Garden OJ, Parks RW. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. Br J Surg 2006; 93:738-744. [PMID: 16671062]
- Petrov MS, Windsor JA. Classification of the severity of acute pancreatitis: how many categories make sense? Am J Gastroenterol 2010; 105:74-76. [PMID: 19844203]
- van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA, Dejong CH, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis (PANTER trial). N Engl J Med 2010; 362:1491-1502. [PMID: 20410514]
- Wu BU, Hwang JQ, Gardner TH, Repas K, Delee R, Yu S, et al. Lactated Ringer's solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol 2011; 9: 710-717. [PMID: 21645639]
- Brun A, Agarwal N, Pitchumoni C S. Fluid Collections in and Around the Pancreas in Acute Pancreatitis. J Clin Gastroenterol 2011; 45:614-625. [PMID: 21750432]
- Sheu Y, Furlan A, Almusa O, Papachristou G, Bae KT. The revised Atlanta classification for acute pancreatitis: a CT imaging guide for radiologists. EmergRadiol 2012; 19:37-43. [PMID: 22160496]
- Beger H G, Bittner R, Block S, Buchler M. Bacterial contamination of pancreatic necrosis: A prospective clinical study. Gastroenterology 1986; 91:433-438. [PMID: 3522342]
- Bradley EL III, Allen K. A prospective longitudinal study of observation versus surgical intervention in the management of necrotizing pancreatitis. Am J Surg 1991;161:19-25. [PMID: 1987854]
- Fedorak IJ, Ko TC, Djuricin G, McMahon M, Thompson K, Prinz RA, et al. Secondary pancreatic infections: are they distinct clinical entities? Surgery 1992; 112:824-830. [PMID: 1411957]
- Tenner S, Sica G, Hughes M, Noordhoek E, Feng S, Zinner M, Banks PA. Relationship of necrosis to organ failure in severe acute pancreatitis. Gastroenterology 1997; 113:899-903. [PMID: 9287982]
- Isenmann R, Rau B, Beger HG. Bacterial infection and extent of necrosis are determinants of organ failure in patients with acute necrotizing pancreatitis. Br J Surg 1999; 86:1020-1024. [PMID: 10460637]
- Büchler MW, Gloor B, Müller CA, Friess H, Seiler CA, Uhl W, et al. Acute necrotizing pancreatitis: treatment strategy according to the status of infection. Ann Surg 2000; 232:619-626. [PMID: 11066131]
- Mee Le J, Paye F, Sauvanet A, O'Toole D, Hammel P, Marty J, et al. Incidence and reversibility of organ failure in the course of sterile or infected necrotizing pancreatitis. Arch Surg 2001; 136:1386-1390. [PMID: 11735865]
- Perez A, Whang EE, Brooks DC, Moore FD Jr, Hughes MD, Sica GT, et al. Is severity of necrotizing pancreatitis increased in extended necrosis and infected necrosis? Pancreas 2002; 25:229-233. [PMID: 12370532]
- Götzinger P, Sautner T, Kriwanek S, Beckerhinn P, Barlan M, Armbruster C, et al. Surgical treatment for severe acute pancreatitis: extent and surgical control of necrosis determine outcome. World J Surg 2002; 26:474-478. [PMID: 11910483]
- Bhansali SK, Shah SC, Desai SB, Sunawala JD. Infected necrosis complicating acute pancreatitis: experience with 131 cases. Indian J Gastroenterol 2003; 22:7-10. [PMID: 12617444]
- Garg PK, Madan K, Pande GK, Khanna S, Sathyanarayan G, Bohidar NP, Tandon RK. Association of extent and infection of pancreatic necrosis with organ failure and death in acute necrotizing pancreatitis.Clin Gastroenterol Hepatol 2005; 3:159-166. [PMID: 15704050]
- Remes-Troche JM, Uscanga LF, Peláez-Luna M, Duarte-Rojo A, González-Balboa P, Teliz MA, et al. When should we be concerned about pancreatic necrosis? Analysis from a single institution in Mexico City. World J Surg 2006; 30:2227-2233. [PMID: 17103098]
- Petrov MS, Shanbhag S, Chakraborty M, Phillips AR, Windsor JA. Organ failure and infection of pancreatic necrosis as determinants of mortality in patients with acute pancreatitis. Gastroenterology 2010; 139:813-820. [PMID: 20540942]
- van Santvoort HC, Bakker OJ, Bollen TL, Besselink MG, Ahmed Ali U, Schrijver AM, et al. A conservative and minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterology 2011; 141:1254-1263. [PMID: 21741922]
- Choi JH, Kim MH, Oh D, Paik WH, Park do H, Lee SS, et al. Clinical relevance of the revised Atlanta classification focusing on severity stratification system. Pancreatology 2014; 14:324-329. [PMID: 25174301]
- Petrov MS, Chong V, Windsor J A. Infected pancreatic necrosis: Not necessarily a late event in acute pancreatitis. World J Gastroenterol 2011; 17: 3173-3176. [PMID: 21912463]
- Rattner DW, Legermate DA, Lee MJ, Mueller PR, Warshaw AL. Early surgical débridement of symptomatic pancreatic necrosis is beneficial irrespective of infection. Am J Surg 1992; 163: 105-119. [PMID: 1733356]
- Gerzof SG, Banks PA, Robbins AH, Johnson WC, Spechler SJ, Wetzner SM, et al. Early diagnosis of pancreatic infection by computed tomography guided aspiration. Gastroenterology 1987; 93: 1315-1320. [PMID: 3678750]
- Rau B, Pralle U, Mayer JM, Beger HG. Role of ultrasonographically guided fine-needle aspiration cytology in the diagnosis of infected pancreatic necrosis.Br J Surg 1998; 85:179-184. [PMID: 9501810]
- Tsui NC, Zhao E, Li Z, Miao B, Cui Y, Shen Y, Qu P. Microbiological findings in secondary infection of severe acute pancreatitis: a retrospective clinical study. Pancreas 2009; 38:499-502. PMID: 19342981]
- Petrov MS, Windsor JA. Response to Talukdar and Vege. Am J Gastroenterol 2011; 106:1170-1171.
- Buter A, Imrie CW, Carter CR, Evans S, McKay CJ. Dynamic nature of early organ dysfunction determines outcome in acute pancreatitis. Br J Surg 2002; 89:298-302. [PMID: 11872053]
- Johnson CD, Abu-Hilal M. Persistent organ failure during the first week as a marker of fatal outcome in acute pancreatitis. Gut 2004; 53: 1340-1344.
- Lankisch PG, Pflichthofer D, Lehnick D. Acute pancreatitis: Which patient is most at risk? Pancreas 1999; 19:321-324. [PMID: 10547190]
- Thandassery RB, Yadav TD, Dutta U, Appasani S, Singh K, Kochhar R. Dynamic nature of organ failure in severe acute pancreatitis: the impact of persistent and deteriorating organ failure. HPB (Oxford) 2013; 15:523-528. [PMID: 23750495]
- Sharma M, Banerjee D, Garg P K. Characterization of Newer Subgroups of Fulminant and Subfulminant Pancreatitis Associated With a High Early Mortality. Am J Gastroenterol 2007; 102:2688-2695. [PMID: 17662103]
- Wig JD, Bharathy KG, Kochhar R, Yadav TD, Kudari AK, Doley RP. Correlates of organ failure in severe acute pancreatitis. JOP 2009; 10:271-275. [PMID: 19454818]
- Mole DJ, Olabi B, Robinson V, Garden OJ, Parks RW. Incidence of individual organ dysfunction in fatal acute pancreatitis: analysis of 1024 death record, HPB (Oxford) 2009; 11:166-170. [PMID: 19590643]
- Bakker OJ, van Santvoort H, Besselink MG, Boermeester MA, van Eijck C, Dejong K, et al. Extrapancreatic necrosis without pancreatic parenchymal necrosis: a separate entity in necrotising pancreatitis? Gut 2013; 62:1475-1480. [PMID: 22773550]
- Singh VK, Bollen TL, Wu BU, Repas K, Maurer R, Yu S, et al. An assessment of the severity of interstitial pancreatitis.Clin Gastroenterol Hepatol 2011; 9:1098-1103. [PMID: 21893128]
- Rana SS, Sharma V, Sharma RK, Chhabra P, Gupta R, Bhasin DK. Clinical Significance of Presence and Extent of Extra Pancreatic Necrosis in Acute Pancreatitis. J GastroenterolHepatol.2015; 30:794-798. [PMID: 25251298]
- Heiss P, Bruennler B. Salzberger B, Lang S, Langgartner J, Feuerbach S, et al. Severe Acute Pancreatitis Requiring Drainage Therapy: Findings on Computed Tomography as Predictor of Patient Outcome. Pancreatology 2010; 10:726-733. [PMID: 21242714]
- Garg PK, Khanna S, Bohidar NP, Kapil A, Tandon RK. Incidence, spectrum and antibiotic sensitivity pattern of bacterial infections among patients with acute pancreatitis. J GastroenterolHepatol 2001; 16:1055-1059. [PMID: 11595073]
- Bourgaux JF, Defez C, Muller L , Vivancos J, Prudhomme M, Navarro F, et al. Infectious complications, prognostic factors and assessment of anti-infectious management of 212 consecutive patients with acute pancreatitis. GastroenterolClinBiol 2007; 31:431-435. [PMID: 17483784]
- Besselink MG, van Santvoort HC, Boermeester MA, Nieuwenhuijs VB, van Goor H, Dejong CH, et al. Timing and impact of infections in acute pancreatitis. Br J Surg 2009; 96:267-273. [PMID: 19125434]
- Noor MT, Radhakrishna Y, Kochhar R , Ray P, Wig JD, Sinha SK, Singh K. Bacteriology of infection in severe acute pancreatitis. JOP 2011; 12:19-25. [PMID: 21206096]
- Cacopardo B, Pinzone M, Berretta S, Fisichella R, Di Vita M, Zanghì G, et al. Localized and systemic bacterial infections in necrotizing pancreatitis submitted to surgical necrosectomy or percutaneous drainage of necrotic secretions. BMC Surg 2013; 13:S50. [PMID: 24267612]
- Rao C, Bhasin DK, Rana SS, Gupta R, Gautam V, Singh K. Implications of culture positivity in acute pancreatitis: does the source matter? J GastroenterolHepatol 2013; 28:887-892. [PMID: 23425090]
- Tsiotos GG, Smith CD, Sarr MG.Incidence and management of pancreatic and enteric fistulas after surgical management of severe necrotizing pancreatitis.Arch Surg 1995; 130:48-52. [PMID: 7802576]
- Doberneck RC. Intestinal fistula complicating necrotizing pancreatitis. Am J Surg 1989; 158:581-584. [PMID: 2589594]
- Kochhar R, Jain K, Gupta V, Singhal M, Kochhar S, Poornachandra KS, et al. Fistulization in the GI tract in acute pancreatitis. Gastrointest Endosc 2012; 75:436-440. [PMID: 22154413]
- Aldridge MC, Francis ND, Glazer G, Dudley HA. Colonic complications of severe acute pancreatitis.Br J Surg 1989; 76:362-367. [PMID: 2655821]
- Mohamed SR, Siriwardena AK. Understanding the colonic complications of pancreatitis. Pancreatology 2008; 8:153-158. [PMID: 18382101]
- Suzuki A, Suzuki S, Sakaguchi T, Oishi K, Fukumoto K, Ota S, et al. Colonic fistula associated with severe acute pancreatitis: report of two cases. Surg Today 2008; 38:178-183. [PMID: 18239882]
- Wille-Jørgensen P, Frederiksen HJ. Colonic necrosis or fistula following pancreatitis orgastric surgery.Eur J Surg 1991; 157:137-139.
- Tüney D, Altun E, Barlas A, Yegen C. Pancreatico-colonic fistula after acute necrotizing pancreatitis. Diagnosis with spiral CT using rectal water soluble contrast media. JOP 2008; 9:26-29. [PMID: 18182739]
- Mallick I H, Winslet M C. Vascular Complications of Pancreatitis. JOP 2004; 5:328-337. [PMID: 15365199]
- Flati G, Andrén-Sandberg A, La Pinta M, Porowska B, Carboni M. Potentially fatal bleeding in acute pancreatitis: pathophysiology, prevention, and treatment. Pancreas 2003; 26:8-14. [PMID: 12499910]
- Balachandra S, Siriwardena AK. Systematic appraisal of the management of the major vascular complications of pancreatitis. Am J Surg 2005; 190:489-495. [PMID: 16105542]
- Zhou F, Wang C, Xiong J, Wan C, Zheng C. Experience in diagnosis and treatment of bleedingcomplications in severe acute pancreatitis.J HuazhongUnivSciTechnolog Med Sci. 2005; 25:182-184. [PMID: 16116967]
- Sharma PK, Madan K, Garg PK. Hemorrhage in acute pancreatitis: should gastrointestinal bleeding be considered an organ failure? Pancreas 2008; 36:141-145. [PMID: 18376304]
- Besselink M G. Splanchnic vein thrombosis complicating severe acute pancreatitis. HPB 2011; 13: 831-832. [PMID: 22081916]
- Nadkarni NA, Khanna S, Vege SS. Splanchnic venous thrombosis and pancreatitis. Pancreas 2013; 42:924-931. [PMID: 23587854]
- Lerch Markus M. Classifying an unpredictable disease: the revised Atlanta classification of acute pancreatitis. Gut 2013; 62:2-3. [PMID: 23220948]
- Frey C, Zhou H, Harvey D, et al. Co-morbidity is a strong predictor of early death and multi-organ system failure among patients with acute pancreatitis. J Gastrointest Surg 2007; 11:733-742. [PMID: 17417710]
- Vege S S, Gardner T B, Chari S T, White RH. Low Mortality and High Morbidity in Severe Acute Pancreatitis without Organ Failure: A Case for Revising the Atlanta Classification to Include “Moderately Severe Acute Pancreatitis”. Am J Gastroenterol 2009; 104:710-715. [PMID: 19262525]
- Talukdar R, Clemens M, Vege SS. Moderately severe acute pancreatitis: prospective validation of this new subgroup of acute pancreatitis. Pancreas 2012; 41:306-309. [PMID: 22015971]
- Talukdar R, Vege SS. Classification of the Severity of Acute Pancreatitis. Am J Gastroenterol 2011, 106:1169-1170. [PMID: 21637274]
- Dellinger E P, Forsmark,C E, Layer P, Lévy P, Maraví-Poma E, Petrov MS, et al. Determinant-Based Classification of Acute Pancreatitis Severity An International Multidisciplinary Consultation. Ann Surg 2012;256: 875-880. [PMID: 22735715]
- Thandassery R B, Yadav T D, Dutta U, Appasani S, Singh K, Kochhar R. Prospective Validation of 4-Category Classification of Acute Pancreatitis Severity. Pancreas 2013; 42: 392-396. [PMID: 23429498]
- Nawaz H, MounzerR ,Yadav D , Yabes JG, Slivka A, Whitcomb DC, Papachristou GI. Revised Atlanta and Determinant-Based Classification: Application in a Prospective Cohort of Acute Pancreatitis Patients. Am J Gastroenterol 2013; 108: 1911-1917. [PMID: 24126632]
- Acevedo-Piedra N G, Moya-Hoyo N, Rey-Riveiro M, Gil S, Sempere L, Martínez J. Validation of the Determinant-based Classification and Revision of the Atlanta ClassificationSystems for Acute Pancreatitis; Clinical Gastroenterology and Hepatology 2014;12:311-316. [PMID: 23958561]
- Petrov, M S, Windsor J A, Le´vy P. New International Classification of Acute Pancreatitis: More Than Just 4 Categories of Severity. Pancreas 2013; 42:389-399. [PMID: 23486363]
- Yadav D. Acute Pancreatitis: Too Many Classifications? What Is a Clinician or Researcher to Do? Clin Gastroenterol Hepatol. 2014; 12:317-319. [PMID: 24090730]
- Thoeni RF. The revised Atlanta classification of acute pancreatitis: its importance for the radiologist and its effect on treatment. Radiology 2012; 262:751-764. [PMID: 22357880]
- Bradley EL, III. Confusion in the imaging ranks: time for a change? Pancreas 2006; 33:321-322. [PMID: 17079933]
- Rana SS, Bhasin DK, Sharma RK, Kathiresan J, Gupta R. Do the morphological features of walled off pancreatic necrosis on endoscopic ultrasound determine the outcome of endoscopic transmural drainage? Endosc Ultrasound 2014; 3:118-22. [PMID: 24955341]
- Bhattacharya A, Kochhar R, Sharma S, Ray P, Kalra N, Khandelwal N, Mittal BR. PET/CT with 18F-FDG-Labeled Autologous Leukocytes for the Diagnosis of Infected Fluid Collections in Acute Pancreatitis. J Nucl Med 2014; 55:1267-1272. [PMID: 24994930]
- Islim F, Salik A, Bayramoglu S, Guven K, Alis H, Turhan AN. Non-invasive detection of infection in acute pancreatic and acute necrotic collections with diffusion-weighted magnetic resonance imaging: preliminary findings. Abdom Imaging 2014; 39:472-481. [PMID: 24441591]
- Gress TM1, El-Omar EM, editorial board of Gut. Revision of the Atlanta classification acute pancreatitis: the editorial perspective. Gut 2013; 62:1. [PMID: 23220947]
- Garg PK, Imrie CW. Severity classification of acute pancreatitis: The continuing search for a better system. Pancreatology 2015; 15:99-100. [PMID: 25700979]
- Windsor JA, Johnson CD, Petrov MS, Layer P, Garg PK, Papachristou GI. Classifying the severity of acute pancreatitis: Towards a way forward. Pancreatology 2015;15:101-4[PMID: 25683639]

