Keywords
Endoscopy, Gastrointestinal; Lithotripsy; Pain; Pancreatitis; Quality of Life
Abbreviations
CP: chronic pancreatitis; MPD: main pancreatic duct; QoL: quality of life
Due to its therapeutic properties, endoscopy can influence the quality of life (QoL) of patients suffering from chronic pancreatitis (CP). Pancreatic ductal decompression represents the most frequent endoscopic procedure in patients with painful CP and it can be considered as a first-line treatment for improving the clinical condition. Endoscopy can limit surgery to unsuccessful or relapse cases. The best candidates for endoscopic treatment are patients with cephalic obstruction of the main pancreatic duct (MPD) by stone(s) and/or stricture(s) with upstream dilation (type IV or, respectively, type V according to the Brussels or the Cambridge ERCP classification) [1, 2]. These patients had pain as a consequence of an elevated intraductal pressure. Combined techniques are usually employed to remove stones and/or to dilate a stenosis, such as a pancreatic sphincterotomy, mechanic lithotripsy, extracorporeal shockwave lithotripsy (ESWL) and pancreatic stent(s). Endoscopy has the potential of improving the QoL in patients with CP since it can decrease or entirely eliminate pancreatic pain and MPD dilation, two variables capable of impairing physical and mental domains [3, 4, 5]. In the Pezzilli et al. study [3], pain was the unique clinical variable able to significantly impair all physical and mental domains in a SF-36 questionnaire administered to 190 consecutive patients with proven CP.
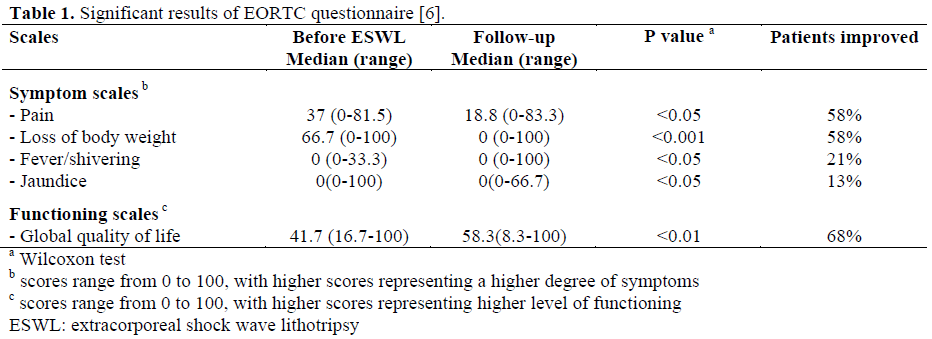
In the literature, only a German study has been published to assess the efficacy of endoscopy in improving the QoL in patients with CP [6]. The efficacy of pancreatic sphincterotomy in achieving this goal was proposed by an American group [Kalloo AN, Baltimore, MD, USA] but this research is ongoing and no data have been published yet. The German study [6] evaluated the QoL after extracorporeal shockwave lithotripsy (ESWL) in combination with interventional endoscopy in 48 patients with symptomatic obstructive calcific CP. A questionnaire of the European Organization for Research and Treatment of Cancer (EORTC-QLQ) modified for patients with CP [7, 8] was used for assessing healthrelated QoL. Relief of pain after endoscopic treatment was defined as a change in character of pain from type A (recurrent short episodes of pain with an intensity greater than 20 in a visual analogic scale) or B (prolonged episodes of pain with an intensity greater than 20 in a visual analogic scale) to type C (absence of type A or B pain). The pain score was calculated by combining pain on a visual analogic scale, frequency of pain attacks, medication for controlling pain, and loss of capacity to work. Endoscopic pancreatic sphincterotomy of the major or minor papilla (pancreas divisum cases) was done in all patients before ESWL and stenting in cases with critical stricture(s). Overall pain relief was recorded in 82% of patients with a JOP. J Pancreas (Online) 2006; 7(1):117-119. © 2006 JOP and author(s). Free circulation of this article is permitted only for research and study purposes. Any commercial and for-profit usage is subject to authorization by the Publisher: see the JOP Special Copyright Statement at https://www.joplink.net/jop/special.html for license details. JOP. Journal of the Pancreas - https://www.joplink.net - Vol. 7, No. 1 Supplement - January 2006. [ISSN 1590-8577] 118 significant decrease of cumulative and individual pain scores. Improvement of the pain score correlated with a decrease in pancreatic duct diameter and weight gain; the latter also correlated with an improved QoL (r=0.58; P<0.005). Complete stone clearance, reduction of the MPD caliber and improvement of the pain score were factors associated with post-ESWL gains. As shown in Table 1, after endoscopy, the global quality of life improved in 68% of patients (significant improvement of functioning scores, P<0.01). Between the several symptoms considered, pain relief, body weight gain, regression of fever and jaundice also improved significantly after endoscopy.
While these results point out a better quality of life for patients with CP undergoing endoscopic treatment, in the abovementioned Italian study, endoscopic pancreatic sphincterotomy does not seem to affect physical and mental domains.
In this regard, it is important to discuss the time interval between the diagnosis and the evaluation of health-related QoL. The negative effect of the endoscopic treatment on QoL in the Italian study could be due to a longer interval (mean 210 months, range 0- 629 months vs. median 69 months, range 1- 300 months) between the time of the diagnosis and that of the evaluation of the QoL. Not only this, it must also be considered that, in the German study, the time interval between the end of the endoscopic treatment and that of the QoL re-evaluation was equal to a median of seven months only (range 5-9 months), representing a short-term period.
Unfortunately, no studies are present in the literature which assess the effect of the endoscopic treatment in improving the QoL in patients with CP after a medium or long-term follow-up. This assessment can be made indirectly on the basis of clinical gains only; however, we must realize that the evaluation is that of physicians and not of patients.
In the largest series, clinical improvement, obtained by adequate MPD drainage, was observed in approximately two-thirds of the patients during a mean follow-up period of 1- 5 years. It correlated closely with a low frequency of pain attacks before the endoscopic treatment, the short duration of the disease before treatment and the absence of MPD stricture. Of 1,670 patients with CP treated by ESWL and endoscopic pancreatic ductal drainage, a mean of 16% (range 6- 26%) needed surgery (unsuccessful endoscopy or relapses of pain). The longest follow-up study for evaluating the clinical outcome of patients with CP after endoscopic treatment was published by Delhaye et al. [9]. During a mean follow-up period of more than 14 years, clinical success (less than 5 hospitalizations without surgery) was observed in 81% of 56 surviving patients which significantly decreased the annual hospitalization rate for pain during the entire follow-up period. This long-term clinical success was associated with the short duration of the disease before initial therapy and the absence of smoking at the last follow-up evaluation. Abstinence from alcohol consumption did not affect pain but constituted the only risk factor for mortality. In Italy, there is usually some scepticism about endoscopic intervention on the pancreas but, after endoscopic treatment, patients with CP had few complications, needed less pain medication and seemed to improve their quality of life. The use of an adequate questionnaire for the evaluation of the healthrelated quality of life of these patients could give a crucial answer in helping to assess the real long-term efficacy of endoscopic treatment in chronic pancreatitis.
References
- Cremer M, Toussaint J, Hermanus A, Deltenre M,De Tceuf J, Engelholm L. Primary chronic pancreatitis.A classification based on endoscopic pancreatography. ActaGastroenterolBelg 1976; 39:522-46. [PMID 1023728]
- Sarner M, Cotton PB. Classification of pancreatitis. Gut 1984; 25:756-9. [PMID 6735257]
- Pezzilli R, MorselliLabate AM, Ceciliato R, Frulloni L, Cavestro GM, Comparato G, et al. Quality of life in patients with chronic pancreatitis. Dig Liver Dis 2005; 37:181-9. [PMID 15888283]
- Wehler M, Reulbach U, Nichterlein R, Lange K, Fischer B, Farnbacher M, et al. Health-related quality of life in chronic pancreatitis: a psychometric assessment. Scand J Gastroenterol 2003; 38:1083-9. [PMID 14621285]
- Wehler M, Nichterlein R, Fischer B, Farnbacher M, Reulbach U, Hahn EG, Schneider T. Factors associated with health-related quality of life in chronic pancreatitis. Am J Gastroenterol 2004; 99:138-46. [PMID 14687155]
- Brand B, Kahl M, Sidhu S, Nam VC, Sriram PV, Jaeckle S, Thonke F, Soehendra N. Prospective evaluation of morphology, function, and quality of life after extracorporeal shockwave lithotripsy and endoscopic treatment of chronic calcific pancreatitis. Am J Gastroenterol 2000; 95:3428-38. [PMID 11151873]
- Bloechle C, Izbicki JR, Knoefel WT, Kuechler T, Broelsch CE. Quality of life in chronic pancreatitis-- results after duodenum-preserving resection of the head of the pancreas. Pancreas 1995; 11:77-85. [PMID 7667246]
- Fitzsimmons D, Kahl S, Butturini G, van Wyk M, Bornman P, Bassi C, et al. Symptoms and quality of life in chronic pancreatitis assessed by structured interview and the EORTC QLQ-C30 and QLQPAN26. Am J Gastroenterol 2005; 100:918-26. [PMID 15784041]
- Delhaye M, Arvanitakis M, Verset G, Cremer M, Deviere J. Long-term clinical outcome after endoscopic pancreatic ductal drainage for patients with painful chronic pancreatitis. Clin GastroenterolHepatol 2004; 2:1096-106. [PMID 15625655]

