Keywords
Adenocarcinoma; Amylases; Intraoperative Complications; Pancreas; Pancreaticoduodenectomy
Abbreviation
POD postoperative day; POPF postoperative pancreatic fistula
INTRODUCTION
For patients with periampullary tumors, including pancreatic cancer, the only treatment with curative intention is a radical pancreatico-duodenectomy[1]. Postoperative leakage from the pancreatic anastomosis is a feared complication that might increase the risk of postoperative morbidity and mortality and result in a prolonged hospital stay. A commonly accepted definition is leakage of drain fluid on postoperative day three or later, with an amylase level of more than three times the upper reference value in serum[2]. The leakage is graded from A to C according to the symptoms and clinical effect. Grade A has no effect on the clinical course, whereas grade C frequently requires intensive care and even a reoperation. The term POPF (postoperative pancreatic fistula) is typically used [2].
The risk of postoperative fistula might be correlated to the texture of the pancreas and the diameter of the pancreatic duct. The risk is increased with a soft pancreatic texture and a duct diameter of 3 mm or less. The risk is further increased by the occurrence of both factors [3]. Other suggested risk factors are the volume of the remnant pancreas and obesity [4, 5]. A system to stratify the risk of anastomotic leakage based on the effects of body mass index (BMI) and the diameter of the pancreatic duct on the preoperative radiology results has been proposed. With this scoring system, patients with obesity and a narrow pancreatic duct have a high risk of POPF, whereas patients with a main pancreatic duct diameter of more than 10 mm have a low risk of POPF [6].
Increased amylase in the drain fluid on postoperative day (POD) 2 and elevated C-reactive protein (CRP) on POD 3 are reported to be strong predictors for pancreatic fistula. A postoperative CRP peak on POD 2 that falls thereafter has been correlated with a low risk of postoperative complications [7].
Pancreatic drains are postoperatively used to evacuate pancreatic fluid and thereby reduce the harm of an eventual pancreatic fluid leak. Drains might increase the risk of complications, including infections. An unelevated amylase value found on POD 1 could indicate that no pancreatic anastomotic leakage is present.
A retrospective analysis of all the pancreaticoduodenectomies performed between January 2011 and December 2014 at Linköping University Hospital was performed. The primary purpose was to evaluate the prognostic value of amylase in the drain fluid on POD 1. A secondary aim was to further validate the prognostic value of CRP for complications after the Whipple procedure.
MATERIAL AND METHODS
All the patients operated on using the Whipple procedure in the surgical department at Linköping University Hospital between January 2011 and December 2014 were included. The Whipple procedure was performed as a classical Whipple operation or as a pylorus-preserving procedure. For the classical Whipple procedure, a gastroenteroanastomosis was antecolic in all the cases, and the enteroenteranastomosis was constructed with a linear stapler. The operations were standard or radical pancreatoduodenectomies that regularly included lymph node stations 12 (all) and 8p, whereas stations 9 and 14 (v,c,d) as well as 15 were only included when the nodes were found to be enlarged [8]. Only the right side of the superior mesenteric artery was regularly skeletonized. Regarding staging, station 16b1 was regularly removed, whereas 16a2 was only removed upon the clinical suspicion of tumor involvement. Resections of the portal vein/superior mesenteric vein were performed when tumor invasion was suspected. In most patients, pancreaticoenteric reconstruction was performed with a two layer ductto- mucosa pancreaticojejunostomy, whereas some reconstructions were performed with a purse-string pancreaticojejunostomy [9, 10]. Biliary reconstruction was achieved with an end-to side hepaticojejunostomy, and bowel continuity was restored with a stapled sideto- side gastrojejunostomy as well as a stapled side-toside enteroenterostomy. A drain was inserted through a separate incision in the abdominal wall and placed in the vicinity of the pancreaticojejunostomy and secured with a non-absorbable suture in the skin. The drain was postoperatively removed when the volume during the past twenty-four hours was less than 200 mL and amylase in the drain fluid was not elevated above 3x the normal serum values.
The data regarding the demographic and surgery related variables as well as the postoperative data and histopathology were retrospectively sampled from the hospital records.
The postoperative complications are reported according to the Clavien-Dindo score [11]. The results are expressed as the median (range), if not otherwise stated. The comparisons between the category variables were performed with a χ2 test, and the comparisons between the means were performed with a t-test. For each variable only available patients are used for statistical comparisons. The unit for amylase is μkat/L, and the unit for CRP is mg/L. The risk factors for POPF evaluated in this study included the pancreatic duct width (> or < than 3 mm) and texture (soft or hard). These factors were evaluated at the time of anastomotic construction. The grading of POPF was conducted according to the established criteria [2].
This study was approved by the local ethics committee of southeast Sweden (Dnr 2015/161-31).
RESULTS
In total, 170 patients, 82 men and 88 women, 70 years of age (28-84), were included. The ASA score was 2 (1-4), and the preoperative BMI was 25 (16-39).
The operating time was 315 (111-817) minutes, and the estimated blood loss was 500 (25-6500) mL. In total, 139 patients (82%) underwent a standard Whipple procedure, 19 patients (11%) had a pylorus preserving Whipple procedure and 12 patients (7%) were operated on with a standard Whipple procedure and additional organ resections. The hospital stay was 9 days (4-107). Eighteen patients (11%) remained in the intensive care unit (ICU) for 4.5 days (1-24).
The grades of the patient complications were as follows: ≥ grade of 3b in 27 patients (16%); grade 3b in 11 patients (7%); grade 4a in 7 patients (4%); grade 4a in 4 patients (2%); and grade 5 in 5 patients (3%). Five patients (3%) died during the hospital stay, and 4 patients (2%) died within 90 days.
In total, 148 (87%) patients received a drain during surgery, whereas 22 (13%) patients did not. The drain amylase was measured on day one in 145 of the patients (98%) who had received a perioperative drain. Therefore the sample size for the primary outcome variable was 145 patients. The patients who did not receive a drain during surgery were considered to have a low risk of developing pancreatic fistula, on the basis of the texture of the pancreas and the diameter of the pancreatic duct. Five (23%) of the patients who did not receive a preoperative drain had an ultrasonography (US)-guided drain postoperatively on the suspicion of a pancreatic fistula, and 2 (9%) of these patients had a confirmed fistula with elevated amylase in the drain fluid, which were classified as grade C fistulas.
In total, 23 patients had postoperative US-guided drainage (4 of these patients had other complications with a higher grade then 3a), and of those, 11 had elevated amylase in the drain fluid (POPF).
The duration of drainage treatment was 4 (2-24) days for the patients who received a perioperative drain and 5.5 (1-62) days for the patients who underwent US-guided drainage postoperatively.
Comparison between Normal and Elevated Amylase in the Drain Fluid on POD 1
In total, 80 patients (55%) had normal drain amylase on POD 1, of whom 8 (10%) developed a postoperative complication grade ≥3b and 2 (3%) developed a POPF. None of the patients with a complication grade of ≥3b had a POPF. The patients were subjected to computed tomography when the clinical condition deteriorated, any fluid collection were either US guided drained or if the patient were reoperated upon and there were any suspicion of leakage from the pancreaticojejunostomy a drain was inserted. Fluid from the drains were analyzed for eventual amylase content.
The two patients with a POPF were classified as grade A. In total, 65 patients (45%) had elevated amylase in the drain fluid on POD 1. Of those, 14 (22%) patients had a postoperative complication of ≥3b, and 10 of these had a POPF of grade C. An additional 19 patients had a POPF, 12 of grade A and 7 of grade B (Figure 1). The difference in the complication rate between the groups with normal and elevated drain amylase on POD 1 did not reach statistical significance (p=0.054); however, the difference in the POPF rate was significant (p<0.001). Table 1 presents these details.
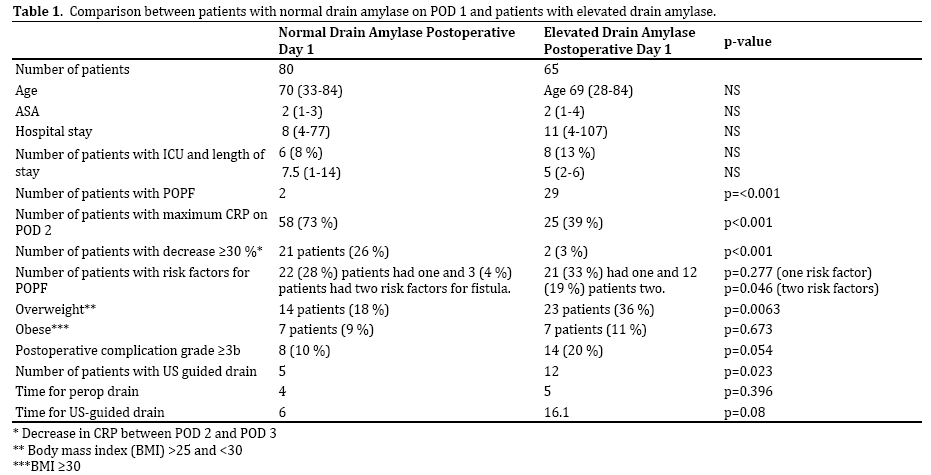
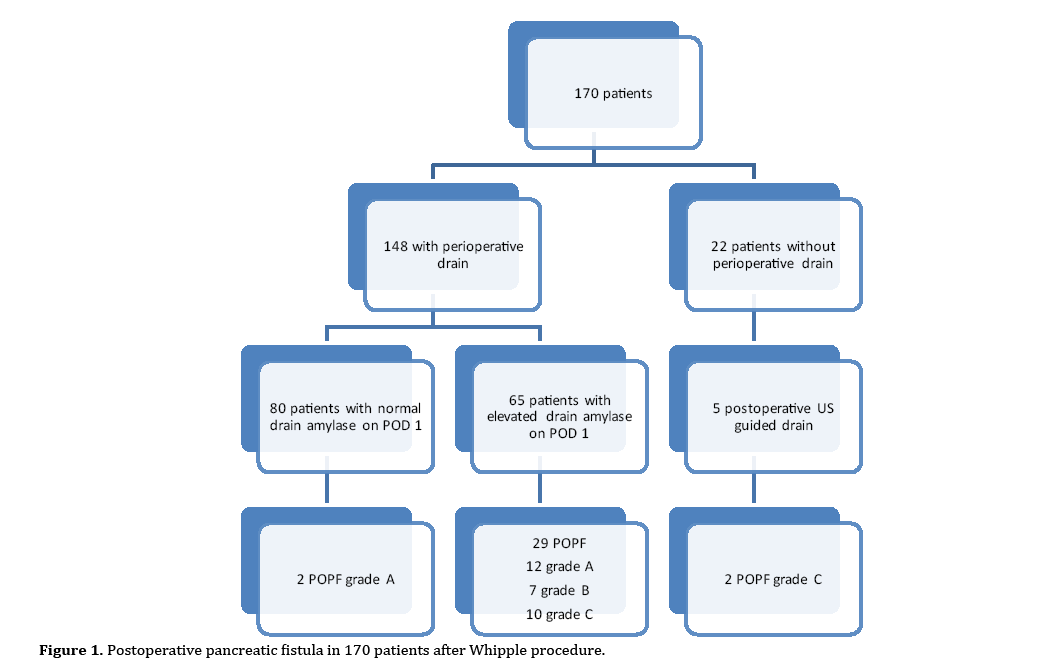
Figure 1. Postoperative pancreatic fistula in 170 patients after Whipple procedure.
In the group with normal drain amylase, 24 patients (30%) had no obvious risk factors (soft texture or duct diameter <3 mm) for a POPF, 22 (28%) patients had one risk factor and 3 (4%) patients had two risk factors for a POPF. Both patients who developed a POPF had one risk factor each for a POPF. In the group with elevated drain amylase, 14 (22%) patients had no described risk factor for POPF, 21 (32%) had one risk factor and 12 (19%) had two risk factors. The difference in the number of patients with two risk factors is statistically significant (p=0.046).
The duration of perioperative drain placement was 4 (2-14) days in the group with normal amylase compared to 5 (2-24) days in the group with elevated drain amylase on POD 1. In the group with normal amylase, 5 patients (6.3%) needed an US-guided drain, which was retained for 1 (1-22) day compared to 15 (1-63) days in the patients with elevated amylase (n=12; 19%) requiring US-guided drainage. The difference in the number of patients who received US-guided drainage is significant (p=0.023).
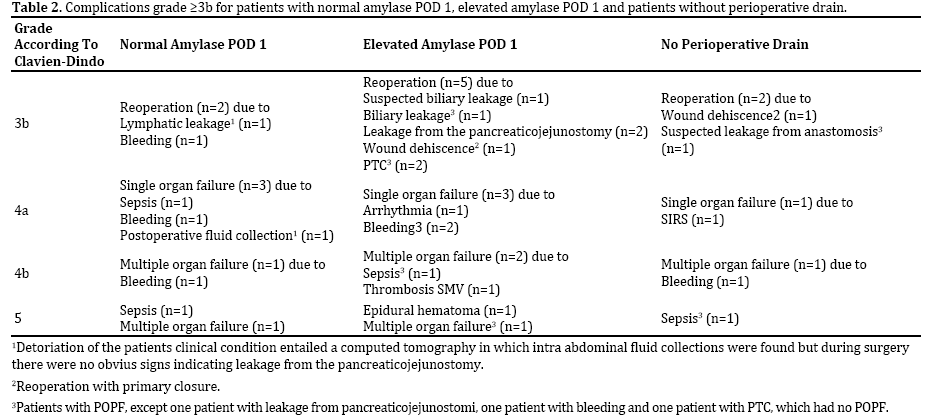
The difference in the length of hospital stay and the ICU stay was not significant between the two groups, with a hospital stay of 8 (4-77) days for the patients with normal drain amylase on POD 1 compared to 11 (4-107) days in the other group. Six patients (8%) had an ICU stay of 7.5 (1- 14) days in the group with normal drain amylase on POD 1, whereas 8 (13%) patients in the group with elevated amylase on POD1 required ICU treatment. Table 2 shows the details regarding the group with normal amylase on POD 1, the group with elevated amylase on POD 1 and the group without preoperative drainage.
There was a significant difference in the number of patients with the maximum value of CRP on postoperative day 2 and the number of patients with a decrease of 30% of more in CRP from postoperative day 2 to postoperative day 3. The difference in the number of overweight patients (25> BMI <30) was significant (p=0.0063), whereas the number of patients with obesity (BMI>30) was not significant.
Postoperative CRP
Comparing CRP on POD 2 and POD 3 between the group with normal drain amylase on POD 1 and the group with elevated amylase on POD 1, 58 patients (73%) in the group with normal amylase had the highest postoperative value on POD 2 compared to 25 (39%) in the group with elevated amylase on POD 1 (p=0.000015). Additionally, there was a significant difference in the number of patients with a decrease in CRP from POD 2 to POD 3 between the groups; 21 (26%) of the patients with normal drain amylase had a decrease of 30% or more compared to 2 (3%) of the patients with elevated drain amylase on POD 1.
In the group with normal amylase, the differences in the CRP level on POD 1, POD 2 and POD 3 were not significant in the patients with a complication ≥ grade 3b compared to those without. The difference in the decrease in CRP from POD 2 to POD 3 was not significant.
In the group with elevated amylase on POD 1, 14 patients had a complication of ≥grade 3b, compared to 51 without a complication of ≥grade 3b. The CRP level decreased by 6%, with an increase of 1% from POD 2 to POD 3. Additionally, 7 of the 26 patients had an increased CRP level from POD 2 to POD 3. One patient in each group had a decrease of 30% or more from POD 2 to POD 3. The difference was not statistically significant.
In the group with normal amylase on POD 1 and a complication ≥ 3b, 5 patients had the highest CRP level on POD 2 compared to the group with elevated drain amylase on POD 1 and a complication ≥3b, whereas 3 patients (5%) had the highest CRP on POD 2. The difference was not statistically significant.
Comparing the patients with complications to those without, regardless of the drain amylase on POD 1, there was no significant difference in the CRP level on POD 1, POD 2 and POD 3 or a significant difference in the postoperative day with the highest CRP.
DISCUSSION
In this retrospective study of 170 consecutive Whipple procedures, postoperative complications ≥ grade 3b occurred in 16% of the patients, and the postoperative mortality was 3%. The rate of POPF was 19%, and 12 (31%) of those were grade C complications. The patients with non-elevated drain amylase on POD 1 very rarely developed a POPF compared to the patients with elevated levels. The rate of severe complications was not significantly different, although there tended to be a correlation between increased amylase on POD 1 and postoperative complications. Additionally, there was a significant difference between these two groups in the number of patients with a maximum CRP level on POD 2 and a decrease in CRP between POD 2 and POD 3. There was no significant difference in the CRP level in the group of patients with complications compared to the group without, regardless of the level of amylase in the drain fluid on POD 1.
The finding that elevated amylase in the drain fluid as early as postoperative day one is correlated with an increased risk of POPF and is associated with an increased risk of postoperative complications has two implications. First, the drain might be removed early in patients with a normal value on POD 1; and second, the patients with elevated amylase might require close observation and monitoring for the early detection of complications. This finding is consistent with a previous study that found a correlation between an elevation of amylase in the drain fluid on POD 1 and POPF occurrence [12], and it is also consistent with other studies in which a correlation between the level of amylase in the drain fluid and POPF severity was found [13, 14].
Early removal of the drain might be safe regarding POPF under the condition that the drain amylase is not elevated. It should however been kept in mind that this study has not considered drains in relation to leakage from biliary- or enteric anastomosis. The removal of the drain on postoperative day 4 compared to day 8 reduces postoperative complications [15]. It is not routine in our department to retain a drain as long as 8 days, provided that the patient does not have a POPF. The use of a drain routinely has been reported not to reduce postoperative mortality or morbidity [16, 17].
Comparing the group with normal amylase on POD 1 and the group with elevated amylase, this study showed a significant difference in the maximum value of CRP. This finding is consistent with previous results; however, the peak in CRP was on POD 3 [18]. The decrease in CRP from POD 2 to POD 3 was more pronounced in the group with normal amylase than in the group with elevated amylase. In total, 26% of the patients in the group with normal amylase had a decrease in the CRP level of 30% or more between POD 2 and POD 3.
Comparing the subgroups of patients with complications in the group with normal amylase on POD 1 and the group with elevated amylase, there were decreases as well as increases of CRP; however, the median difference was small. There was no significant difference in the change in CRP. There was no significant difference in the increase of the CRP level from POD 1 to POD 3 among the patients with a complication ≥3b compared to the patients without severe complications, regardless of the level of drain amylase on POD 1.This finding differs from previous results, which showed that patients with a POPF had an increase in CRP from POD 1 to POD 3 [19].
In our study, we found a significant difference between the patients with and without elevated amylase on POD 1 and the number of patients with a soft pancreas and thin pancreatic duct; there was no significant difference in the number of patients with only one of those risk factors. Additionally, we found a significant difference in the number of overweight patients, but not in the number of obese patients, compared to the number of patients with normal body weight (BMI<25). These three risk factors for a POPF [20, 21] are not consistently described for all patients. It has been reported that there is no difference in morbidity and mortality in patients with normal weight, overweight and obesity [22].
Our results suggest that patients with complications and elevated drain amylase on POD 1 have a postoperative elevation of CRP later and that the decrease between day 2 and day 3 is small. This finding is consistent with other results; patients with risks of complications have a longer inflammatory response than do patients with no complications [23].
CONCLUSION
These results suggest that patients with normal amylase in drain fluid on POD 1 after the Whipple procedure have a significantly lower risk of POPF and that the risk of postoperative complications might be lower than in patients with elevated drain amylase on POD 1.
Conflict of Interest
The authors declare that they have no competing interests.
References
- Chen SC, Shyr YM, Wang SE. Longterm survival after pancreaticoduodenectomy for periampullary adenocarcinomas. HPB (Oxford) 2013;15:951-7. [PMID: 23472708]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138:8-13. [PMID: 16003309]
- Ansorge C, Strommer L, Andren-Sandberg A, Lundell L, Herrington MK, Segersvard R. Structured intraoperative assessment of pancreatic gland characteristics in predicting complications after pancreaticoduodenectomy. Br J Surg 2012;99:1076-82. [PMID: 22556164]
- Del Chiaro M, Rangelova E, Ansorge C, Blomberg J, Segersvard R. Impact of body mass index for patients undergoing pancreaticoduodenectomy. World J GastrointestPathophysiol 2013;4:37-42. [PMID: 23755369]
- Frozanpor F, Loizou L, Ansorge C, Segersvard R, Lundell L, Albiin N. Preoperative pancreas CT/MRI characteristics predict fistula rate after pancreaticoduodenectomy. World J Surg 2012;36:1858-65. [PMID: 22450754]
- Roberts KJ, Hodson J, Mehrzad H, Marudanayagam R, Sutcliffe RP, Muiesan P, et al. A preoperative predictive score of pancreatic fistula following pancreatoduodenectomy. HPB (Oxford) 2014;16:620-8. [PMID: 24246089]
- Ansorge C, Nordin JZ, Lundell L, Strommer L, Rangelova E, Blomberg J, et al. Diagnostic value of abdominal drainage in individual risk assessment of pancreatic fistula following pancreaticoduodenectomy.Br J Surg 2014;101:100-8. [PMID: 24306817]
- Pedrazzoli S. Extent of lymphadenectomy to associate with pancreaticoduodenectomy in patients with pancreatic head cancer for better tumor staging.Cancer Treat Rev 2015. [PMID: 26045226]
- Bassi C, Falconi M, Molinari E, Mantovani W, Butturini G, Gumbs AA, et al. Duct-to-mucosa versus end-to-side pancreaticojejunostomy reconstruction after pancreaticoduodenectomy: results of a prospective randomized trial. Surgery 2003;134:766-71. [PMID: 14639354]
- Jiang C, Wang M, Xu Q, Wu X, Yu D, Ding Y. A modified technique for end-to-side pancreaticojejunostomy by purse-string suture.J Surg Oncol 2011;104:852-6. [PMID: 21713776]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205-13. [PMID: 15273542]
- Sutcliffe RP, Battula N, Haque A, Ali A, Srinivasan P, Atkinson SW, et al. Utility of drain fluid amylase measurement on the first postoperative day after pancreaticoduodenectomy.World J Surg 2012;36:879-83. [PMID: 22354484]
- Ceroni M, Galindo J, Guerra JF, Salinas J, Martinez J, Jarufe N. Amylase level in drains after pancreatoduodenectomy as a predictor of clinically significant pancreatic fistula. Pancreas 2014;43:462-4. [PMID: 24622080]
- Hiyoshi M, Chijiiwa K, Fujii Y, Imamura N, Nagano M, Ohuchida J. Usefulness of drain amylase, serum C-reactive protein levels and body temperature to predict postoperative pancreatic fistula after pancreaticoduodenectomy. World J Surg 2013;37:2436-42. [PMID: 23838932]
- Kawai M, Tani M, Terasawa H, Ina S, Hirono S, Nishioka R, et al. Early removal of prophylactic drains reduces the risk of intra-abdominal infections in patients with pancreatic head resection: prospective study for 104 consecutive patients. Ann Surg 2006;244:1-7. [PMID: 16794381]
- Lim C, Dokmak S, Cauchy F, Aussilhou B, Belghiti J, Sauvanet A. Selective policy of no drain after pancreaticoduodenectomy is a valid option in patients at low risk of pancreatic fistula: a case-control analysis. World J Surg 2013;37:1021-7. [PMID: 23412469]
- Conlon KC, Labow D, Leung D, Smith A, Jarnagin W, Coit DG, et al. Prospective randomized clinical trial of the value of intraperitoneal drainage after pancreatic resection. Ann Surg 2001;234:487-93; discussion 93-4. [PMID: 11573042]
- Welsch T, Frommhold K, Hinz U, Weigand MA, Kleeff J, Friess H, et al. Persisting elevation of C-reactive protein after pancreatic resections can indicate developing inflammatory complications. Surgery 2008;143:20-8. [PMID: 18154929]
- Kanda M, Fujii T, Takami H, Suenaga M, Inokawa Y, Yamada S, et al. Novel diagnostics for aggravating pancreatic fistulas at the acute phase after pancreatectomy. World J Gastroenterol 2014;20:8535-44. [PMID: 25024608]
- Roberts KJ, Sutcliffe RP, Marudanayagam R, Hodson J, Isaac J, Muiesan P, et al. Scoring System to Predict Pancreatic Fistula After Pancreaticoduodenectomy: A UK Multicenter Study. Ann Surg 2015; 261:1191-7. [PMID: 25371115]
- Fuks D, Piessen G, Huet E, Tavernier M, Zerbib P, Michot F, et al. Life-threatening postoperative pancreatic fistula (grade C) after pancreaticoduodenectomy: incidence, prognosis, and risk factors. Am J Surg 2009;197:702-9. [PMID: 18778804]
- Balentine CJ, Enriquez J, Cruz G, Hodges S, Bansal V, Jo E, et al. Obesity does not increase complications following pancreatic surgery. J Surg Res 2011; 170:220-5. [PMID: 21514600]
- Sakoda M, et al. Indicators of complications and drain removal after pancreatoduodenectomy. J Surg Res 2011;170:e211-6. [PMID: 21816438]

