Keywords
Quality healthcare; Performance measure; Quality improvement; Perception
Introduction
During the last years, the improvement of the quality of health care became an absolute priority and a main objective for any health system all over the world [1-3]. Indeed, in 2000, the World Health Organization (WHO) in its report on the health in the world emphasized the improvement of the performances of the health systems of countries to reach three objectives of the millennium for development bound to the health [4]. In this context, the measure of performance in health care which is essential to improve the quality, to reduce the errors and to favor a bigger efficiency becomes essential [5]. However, the health system is a complex system and its complexity is characterized by: 1) Numerous processes, partially not standardisables and fast evolution. 2) multiple jobs and permanent evolution. 3) a particular sociology, in particular as regards the distribution of decision-making powers. 4) a quality of products of the freed difficult to arrest for the professionals and the patients. 5) difficulty for identifying and evaluating the effect of quality approaches [6].
Furthermore, the systems of health care are at present confronted with several formidable challenges: The increase of the demand of care, the emergence of an economic landscape in which the systems of care have to make more with less [3], a misuse of health services, lack of consciousness of the importance of the measure of the errors in the practice of health care [7].
In developing countries and especially in Africa, health systems have difficulty in filling effectively their functions because of their weakness and of their fragmentation [8]. The weakness of health systems is known by a number of factors which are worth knowing: Inadequacies at the level of the planning and of the forecast, the shortage of the human, financial and material resources, the insufficiency of the data to inform in an enlightened way the decision-making, the gaps of the institutional processes and the weaknesses of the follow-up of the performance and the impact of the interventions.
The measure, the evaluation and the comparison of the performances of the quality of the care have three main objectives: 1) To give responsibilities to the persons receiving benefits of health, 2) to develop better adapted politics and 3) to allow the persons receiving benefits and the other stakeholders to exchange their knowledge [9].
However, the quality of the care is a concept difficult to seize because of the complexity of its evaluation [10]. It is necessary to notice that the dynamics give a complex of the service of health care, the various levels of evaluation of the care and the various perspectives of the key participants of the system are adequately represented. Because the quality of the healthcare dresses multiple dimensions and can be arrested according to various points of view [3].
The Health care quality dresses multiple dimensions and can be attested according to various points of view. According to the question on the consensus between the various views points on the Health care quality to do what? Quality approaches are articulated around two big dimensions of the quality: On one hand, the objectification of a quality deficit thanks to the measure of spread with regard to reference tables beforehand defined. On the other hand, the implementation of initiatives of continuous improvement of the quality resting on tools and approaches which are showed on the ground (Accreditation, certification, audit and Competition quality).
Morocco, as all the countries of the world, did not escape this wave of the Health care quality which accompanied political, institutional, economic and social reforms during ninety’s years [11]. Several projects implemented the activities of Quality assurance by the various structures of the Health Ministry of, such as Hospital Audits, Team Approach for the problems resort, the elaboration of the standards, the accreditation of hospitals, certification of analysis laboratories and institution of cycles quality according to the approach of management integrated by the quality which focuses its interventions on the process of continuous improvement of the quality. All this was concluded by a conference on the quality of health in 2002 and a number of recommendations were emitted: 1) To show a political will and to bring the necessary support for the implementation of a system of accreditation. 2) To identify and to standardize the existing mechanisms of normalization and to set up new mechanisms. 3) To create a national organ of accreditation. 4) To strengthen the system of information and of documentation about the quality of care. 5) To develop, to adapt, to revise and to spread the national reference tables. 6) To implant, to support, to generalize the steps of Quality assurance in the sanitary structures. 7) To train, to inform, to make sensitive the actors of health and partner on the system of accreditation [12].
The governance centered on the quality requires the evaluation of health systems to know if they are able of supplying care effective and centered on the patient. This governance is dependent on information on the quality of the health care which aims at: 1) To improve the coherence and the coordination of the care, 2) to predict the disease, 3) to do this so that the sick receive the care which they need. 4) to guarantee the efficiency of the care, 5) to guarantee the safety(security) of the care, 6) to reward the persons receiving benefits (providers) of health who provide medical care of quality and 7) to develop health systems towards a mode of governance based on the results(profits) and governed by the quality [3] .
In spite of the efforts supplied regarding research on the quality of the care, a number of questions remain to be asked: How to measure the performance regarding quality of the care? How to introduce the strategies of improvement of the quality of the care into the public politics? Do quality approaches (CQ) improve the performance health care establishments?
Method
Qualitative research is increasingly common in health services research [13]. Physician–patient relationships and primary care [14]. Based on the conceptual frameworks for performance measurement of primary health care around the world and drawing mainly on the conceptual framework of the Moroccan quality competition, we have proposed a multidimensional framework for assessing the performance of health services through the health staff. In our analysis plan we followed the method of using the terminology proposed [15] by researchers, these three phases are presented: Condensation of the data; organization and presentation of data; and interpretation and verification of conclusions [16].
The internal validity of our research is its ability to establish relations between the different relationships of the theoretical model [17-21]. The transferability of the results is ensured by the constitution of the sample and its representativeness, meet the criterion of theoretical relevance in relation to the study situation; The second condition concerns the detailed description of the sample of the study as outlined [22]. This is among the few study to document the impact of accreditation on HCPE in Morocco. The congruence between our model of analysis and the observations collected previously [13,17,19] allows us to assert that the validity of this study is good.
In our research, we opted for the qualitative method based on the interpretative approach, this approach is used more and more in the health services research. Four main questions settle in the context of the collection of data on the Measurement of performance in the primary health care. It is about the complexity, the cost, the type of data of collecting and the quality of the collected data [23].
Our data analysis plan based on the statistical analysis that is essential to the validity of the study. Set the desired efficiency levels according to the scores assigned by the staff in each dimension, then add up the scores and convert it into a percentage. The performances are classified in 4 categories: Very weak (0- 25); low (525-50); satisfactory (50-75); and excellent (75-100). The analyses of qualitative data, where we make sense of the data collected allowed us to elaborate, validate, weight and structure the indicators and to build a modeling of the quality of care based on the theoretical models, this allowed us to group the indicators in terms of results, process or structure.
Hypothesis H1: Quality approach (CQ) favors the improvement of the performance of the quality of the care. There is a very narrow relation between quality approaches (CQ) and performance of the quality of the care. H2: The measurement of care quality performance causes no problems and the abstract frames of performance measurement of the care quality are uniform and easy to use.
Objectives
Evaluate the perception of health staff on the quality of care in the PHCE in Morocco; evaluate the performance management systems in the field of care in Morocco by analyzing the different dimensions and perspectives of the quality of health care.
Questionnaire
We used a questionnaire which contains 3 parts adapted according to the model of Donabedian (Structure, processes and results), including seven domains. The first part concerns the Structure dedicated for the planning of the quality and the leadership and the human resources management. The second part concerns the processes dedicated to the management of the processes, the monitoring and the analysis. The third part handles the results of the quality and the satisfaction of the users. Every domain contains 5 in 9 questions handling an aspect with a total of 46 questions. The questionnaire was sent to the concerned in an individual way either directly or through emails, by assuring the respondents a total confidentiality, by underlining the independence of the researcher of the direction and by proposing a right of revision on the held words, to establish a " relative reliable climate ". The answers are classified between ' not at all right ' with a score of (1) and 'completely all right' with a score of (5). This type of question offers the advantage to facilitate the collection and the perusal of the information (Figure 1).
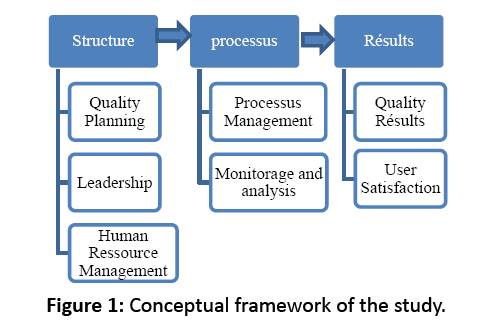
Figure 1: Conceptual framework of the study.
Sampling
Our study concerns PHCE staffs who have already participated in the quality competition. Our sample was selected by random draw from PHCE staff who has already participated in the CQ. The survey affected 35 PHCE among 140 who participated in quality competition in 5 regions, in the order of 2 people by PHCE. The questionnaire is addressed to 70 people practicing in the 'PHCE' of 5 regions of Morocco, 62 questionnaires were got back filled. The profiles of the respondents are as follows: 24 doctors among whom 12 are head doctors of PHCE and 38 nurses among whom 18 are head nurses of the health centers who introduced a quality approach (Tables 1 and 2).
| Profil |
Doctor |
Nurses |
Total |
| |
With responsibility |
Total |
With responsibility |
Total |
With responsibility |
Total |
| Nombre |
12 |
24 |
18 |
38 |
30 |
62 |
Table 1: Distribution of people investigated according to the profile and the status screw opinion of the responsibility.
| |
|
Years of seniority in the system |
|
| |
|
0-10 years |
10-20 years |
20 years + |
Total |
| sex |
M |
4 |
14 |
8 |
26 |
| F |
6 |
24 |
6 |
36 |
| Total |
|
10 |
38 |
14 |
62 |
Table 2: Distribution of people investigated according to the age in the health system and the sex.
Presentation and Analysis of the Results
The global perception
The staff of the PHCE of our sample (57%) qualifies the quality in health care establishments as average, while 9% have a bad perception of the quality of the services, the tan record 34% have a good perception on the quality of their health system (Graph 1).
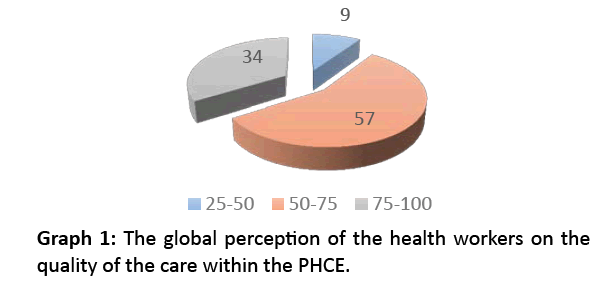
Graph 1: The global perception of the health workers on the quality of the care within the PHCE.
The answers of the staff are highly varied according to the dimensions and the vast enters the score min and the score max is much reduced (10 points) for the dimension result of the quality, while it is very wide (37 points) for the dimension planning of the quality. For the principles of the quality management according to the program National of quality assurance which are: Planning of the quality and the quality management, the leadership and the satisfaction of the users the average scores exceed the 70% (Table 3).
| Domains |
Min |
Moy |
Max |
Ecart |
| Planning quality |
42 |
65 |
77 |
37 |
| Monitorage and analysis |
52 |
60 |
67 |
15 |
| Leadership |
52 |
71 |
83 |
31 |
| Human ressources management |
47 |
58 |
72 |
25 |
| Processus Management |
42 |
56 |
67 |
25 |
| Quality Results |
73 |
79 |
83 |
10 |
| User Satisfaction |
63 |
74 |
80 |
17 |
| General average |
53 |
66 |
75 |
22 |
Table 3: The perception of the staff of the PHCE of the quality of health services according to the domains of the questionnaire.
The perception of the quality of the staff of the PHCE by domains
The domains are peeled in aspects.
Quality planning: The average score of this dimension is of (65%), Three aspects are successful namely: The preservation of the specific objectives to improve the quality of the services and the care, the implication in the development of plans of improvement of the quality of the services and the care and the participation of in the elaboration of action plans and the prioritization of the activities have a score of (77%). The score for the arrangement of time required to plan and test the improvements, the participation in the establishment of the priorities for the improvement of the quality of the services and the care is of (65%). While the participation of the partners (other health centers, community groups, hospitals, diverse bodies, etc.) in the establishment of the priorities for the improvement of the quality of the services and the care remains very low with a score of (42%) (Table 4).
| Planning Quality |
Score en % |
| The arrangement of the time required to plan and test the improvements. |
65 |
| The preservation of the specific objectives to improve the quality of the services and the care. |
77 |
| The implication in the development of plans of improvement of the quality of the services and the care. |
77 |
| The establishment of the priorities for the improvement of the quality of the services and the care by the staff |
65 |
| The partners Participate in a significant way in the establishment of the priorities for the improvement of the quality of the services and the care. |
42 |
| Domain mean |
65 |
Table 4: The level of perception of the performance level of the domain «planning of the quality by the staff.
Monitoring and data analysis: The average score of this dimension is of (60%). The highest scores for this dimension are represented by aspects: The collection of data on the quality of the services and the care and the implication of the staff in the identification of the data to collect for the improvement of the quality of the services and the care by a score of (67%). The use of data on the quality of the services and the care, the improvement of the use of the data and the information on the quality of the services and the care and the check and the improvement of the reliability of the data on the quality of the services(departments) and the care with a score of (60%). The health center compares its data on the quality of the services and the care with other health centers with a score of (58%). The lowest score is for the improvement of the relevance of its data on the quality of the services and the care (52%) (Graph 2).
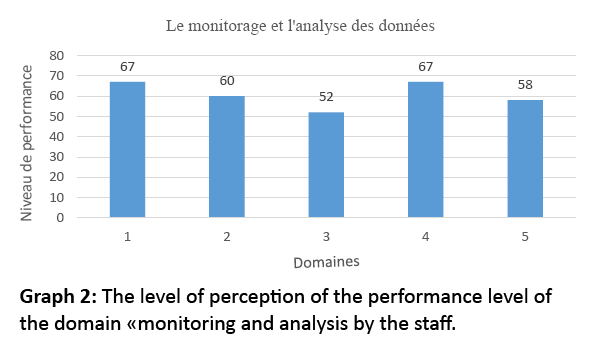
Graph 2: The level of perception of the performance level of the domain «monitoring and analysis by the staff.
1. The collection of data on the quality of the services and the care.
2. The use of data on the quality of the services and the care.
3. Look for the relevance of the data on the quality of the services and the care.
4. The implication activates in the collection of data for the improvement of the quality of the services and the care.
5. The notion to compare the data on the quality of the services and the care with other health centers.
Quality results: The average score of this dimension is of (79%). The most successful aspects which make up this dimension are the constant and measurable improvements of the quality of the services and the care with a score of (83%). Constant and measurable improvements of the results of the satisfaction of the users with a score (82%). For the notion of measuring of the improvements of the quality of her organization in a constant way is of (77%). The preservation of this improvement of the quality in spite of the multiple constraints is of (73%) (Table 5).
| Quality results |
Score en % |
| The improvements are constant and measurable of the quality of the services and the care. |
83 |
| The improvements are constant and measurable results of the satisfaction of the users. |
82 |
| The improvements are constant and measurable of the quality of the organization |
77 |
| A preservation of the improvement of the quality in spite of the multiple constraints. |
73 |
| Domain means |
79 |
Table 5: Le niveau de perception du niveau de performance de la dimension " résultats de la qualité " par le personnel.
Quality management processes: The average score of this dimension is of (56%). The performances of this dimension remain less successful generally: For the regular control equipment and materials to make sure that they satisfy the quality standards and the research for improvement of the approach quality and of (67%). Encouraging the use of indicators to measure quality is of (62%). The coordination of the efforts of the staff with the others to improve the quality of the services offered by the health center is of (58%). The use of the data stemming from partners, (other health center, community groups, hospitals, diverse body) for the elaboration of the plan of health center quality improvement is of (57%). The evaluation of the quality before being set up is of (50%). The health center has effective politics to support the development of the quality of the services and the care with a score of (45%). The collaboration with the partners (other health center, group’s community, hospitals, diverse body, etc.) to improve the quality of their products and services is of (42%).
The leadership: The average score of this dimension is of (71%). The scores of this dimension are very high. The leadership contributes to the improvement of the quality of the services and the care had the highest score of (83%). The persons in charge show a visible leadership by creating an environment favorable to the quality improvement the services and the care (80%). The staff encourages the efforts to improve the quality of the services and the care and participate actively in activities to improve the quality of the services and the care with a score of (77%). The staff takes in the information from the users and the families (needs, suggestions) to improve the quality of the services and the care (72%). The staff makes suggestions to improve the quality of the services and the care (70%). The clear vision to improve the quality of the services and the care with a score of (63%). The staff shows a skill to manage the changes (organizational, technological) necessities to improve the quality of the services and the care (62%). The staff has a thorough knowledge of the way of improving the quality of the services and the care (52%) (Table 6).
| Leadership |
% score |
| Maintain an environment favorable to the improvement of the quality of the services and the care |
80 |
| The participation activates in the activities to improve the quality of the services and the care. |
77 |
| Have a clear vision to improve the quality of the services and the care |
63 |
| Be smart enough to manage the changes (organizational, technological) necessities to improve the quality of the services(departments) and the care |
62 |
| Have a thorough knowledge of the way of improving the quality of the services and the care. |
52 |
| Encourage the efforts to improve the quality of the services(departments) and the care |
77 |
| Means |
71 |
Table 6: Le niveau de perception du niveau de performance de la dimension " leadership " par le personnel.
User’ satisfaction: The average score of this dimension is of (74%). The aspects of this dimension are: the study of the complaints of the users is used to prevent the repetition of the same problems (80%), the contribution to solve quickly the complaints of the users (78%). The use of the data stemming from users to improve the services (77%). The evaluation in a satisfactory way, the needs for the users and their expectations as well as the data on the users are widely broadcast with the staffs of the health center with a score of (73%). The evaluation in a satisfactory way of the satisfaction of the professionals of the health center the respect of the services (63%) (Table 7).
| User Satisfaction |
% score |
| The evaluation the needs for the users and their expectation. |
73 |
| The contribution to solve quickly the complaints of the users. |
78 |
| The prevention of the repetition of the same problems. |
80 |
| The distribution of the data with the staffs of the health center. |
73 |
| The evaluation of the satisfaction of the professionals of the health center towards the services. |
63 |
| Means |
74 |
Table 7: The level of perception of the performance level of the dimension satisfaction of the users by the staff.
Human resources management: The average score of this dimension is of (58%). The aspects of this dimension: The motivation to improve the quality of the services and the care with a score of (73%). The arrangement of an effective system so that the staff makes suggestions to the persons in charge on the way improve the quality of the services and the care (72%). Training in other methods which rest the improvement of the quality of the services of the care. Communication, management of the CS (58%). The services cooperation to improve the quality is supported and encouraged (55%). The organization of the training on the quality management of the services of the care and the professional autonomy for will improve the quality of the services and the care with a score of (50%). The organization of the necessary training to improve the professional skills and the performance (47%) (Graph 3).
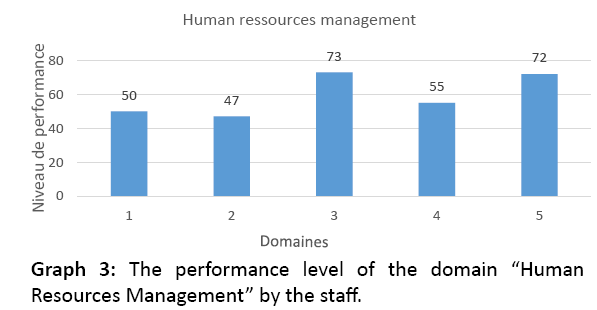
Graph 3: The performance level of the domain “Human Resources Management” by the staff.
1. The staff training on the management by the quality of the services of the care.
2. The necessary training to improve the professional skills and the performance.
3. The motivation of the staff to improve the quality of the services and the care.
4. The cooperation inter services to improve the quality is supported and encouraged.
5. An effective system is implanted so that the staff makes suggestions to the persons in charge on the way
Discussion
Several studies were interested in the search on the efficiency of the certification and the measure of performance [19,24-28] other studies explored the impact of these programs on the accredited bodies [19,29] others tried to analyze the performance of the certification by examining their structure and their process [25,29]. What shows of the complexity of the problem and not unification of the methods of research on the health care quality and the performance measurement?
The frame of evaluation of this study rests on a Synthesis (a warning) between Donabedian paradigm of the health care quality, who binds the structure, the process and the results, on an abstract frame of the performance evaluation of the primary health care based on the CQN frame, associated with a synthesis of the other frames quoted in the literature [30,31].
However, even if these studies take into account numerous indicators to analyze health systems, they use them by adding simply the scores obtained in each of the indicators. This aggregation of indicators reduces the information available on only one global score, without taking into account really the interdependence between indicators and relations which can exist between them. Besides, by using a global score to analyze the performance of health systems, it is not possible to know in which indicators we obtain the best and the least good scores [32].
Our plan of discussion of the results will be organized in 2 levels. Generally Impact and Impact by domains.
The impact on the health care system generally
There are divergent and contradictory opinions as for the incidence of quality approaches on the results of the customers. The existing researches do not contain rigorous and thorough analysis of the process of Accreditation/certification and its relation with the performance, the results and the improvement of the quality and the safety of the patients [33]. Ovretveit and Al. revealed that the document retrieval contained relatively few proofs concerning the global efficiency of the quality interventions and the quality standards in health care [28].
Several bodies of accreditation/Certification introduced, developed, incorporated and checked the indicators of clinical quality in the organizations of health care. As a consequence, improvements were apparently observed in the results of these organizations regarding care on the infrastructure and the performance of control of the infections of hospitals [29]. The results of the care describe the effects and the consequences of the services on the population health [34].
The relevant results for the primary health care systems are bound to the health, to the equity, to the patient satisfaction and the persons receiving benefits, to the costs and to the efficiency. The studies revealed links with the governance, the access, the continuity, the coordination, the efficiency and the strength primary care [35]. Within the framework of the primary health care the same advantages are brought back between our study and the literature [36]: 1) A better quality control by the achievement of a minimum quality level of the service. 2) A better regulations by respecting the legal rules and of safety. 3) The continuous and long-lasting improvement of the quality. 4) The supply of information to the patients, what confers a confidence in the supplied services and allows them to take informed decisions. 5) To establish a positive image insists on the aspects of practice and service standards in the primary health care centers. According to Pomey and al. the results of the search on the certification tend to demonstrate that it is an effective form of professional control that can have a positive impact on the values and the organizational culture [20].
The results of our study revealed a statistically significant correlation between the results of the quality and the other dimensions (the leadership, the strategic planning of the quality, the quality management). This result is coherent with the previous searches made by Marie [37], which, indicated that the dependent variable (quality results) was positively correlated in the leadership, in the commitment and in the support, the development of the staff, the use of the variables of data. Besides, they added that the leadership, the commitment and the support were significantly associated to quality results, which indicate that the high direction was strongly committed to the accreditation in their hospitals [38,39], what is not the case for our study or the commitment of the direction appears among the weak points of the CQ.
The impact by domains
Process management: Be concerned with the measurement of care processes in relation to outcome measurement, on the pretext that improving clinical outcomes necessarily involves improving care processes. One of the risks of process optimization is that performance gains can be lost once the project is completed if it is not supported by other mechanisms [40], this was formulated in our study as one participant pointed out: "The sustainability of the achievements is not guaranteed, the discontinuity in the work by the large number of programs". The average score for this dimension is 56%, the quality assessment before being put in place is to 50%, The health center has an effective policy to support the development of quality of services and care with a score of 45%, collaboration with partners (other health centers, community groups, hospitals, other organizations, etc.) to improve the quality of their products and services is 42%.
Monitoring and data analysis: According to Brasure et al. [40] difficulties in collecting data and meeting accreditation standards were identified as the main obstacle [29]. It is important to note that the use of data in the accreditation process can help hospitals track improvement activities, measure performance and provide evidence of compliance with accreditation standards [39]. The process of "Monitoring and Data Analysis" of 60% and is only the 52% for the relevance of its data on the quality of services and care The PHCE compare their data on the quality of services and care among them only in (58%); Few studies have succeeded in building a conclusive data collection tool that empirically explains how adopting the above practices improves the health system [41,42].
The safety of the care: Safety of care is the priority dimension on which the quality approach focuses its efforts, it relies on several risk management methods (process analysis, problem solving, etc.) and the continuous improvement of care. To guarantee safety in patients. There are a number of challenges in this area, some of which have their origins in PHC such as low participation and commitment of individuals, lack of support from higher levels, lack of recognition or understanding of errors and lack of resources. On the other hand, the external difficulties, one notes the complaints for medical negligence which lead to avoid the recording of the errors and faults in the systems, in addition to the costs that generate the maintenance of the system [43].
The impact on the change of professional practices: A majority of studies indicate that accreditation has a positive effect on improving professional practice [44]. The study by Douguet and Muñoz [45] on the impact of accreditation and quality of care measures on the activity of health care workers concluded that many of the staff questioned had a negative image. Accreditation/Certification, for our case (68%) has this image that varies between medium and low on the Quality Competition. The perception by health professionals of the tools of the total quality is also uncertain, even if several studies have shown a good adherence of health professionals to this type of approach [46]. According to El Jardali et al et al. [47], staff involvement was significantly associated with higher quality results, but our sample staff is concerned about "insufficient staff motivation" and "non-adherence to everything "in the QC process.
Leadership: The most important predictors of higher quality outcomes were leadership, engagement and support, data use, education and training, rewards and the recognition and benefits of accreditation [38]. Leadership plays a central role in the development and implementation of the strategy [48]. The average score for this dimension is (71%). Leadership contributes to improving the quality of services and care (83%). Managers demonstrate visible leadership by creating an environment conducive to improving the quality of services and care (80%).
Conclusion
In spite of the challenges which the Moroccan health system knows, we note that the perception of the performance the staff of care remains relatively high (exceed largely the 60%). The approaches of QCI are a good tool to improve the quality of the care, the high score of variables "quality results indicate that the staff perceived an improvement of the hanging quality and after the implementation of quality approaches. Even if the links are not established yet within the framework of a scientific research, quality approaches are generally recognized as essential tool to help establishments to improve the quality and the safety of the patients. Tools proposed in quality approaches remain an essential lever for the promotion of quality approaches. The current approach regarding measurement of performance of the quality is far from establishing an effective national system of measurement of performance and production of reports for the following reasons: The objectives are not well defined and are not accessible. The existing approaches produce measures which are inconsistent, complex and unstable, imposing to the persons receiving benefits of care the uncertainty and the burden of the contradictory measures. The primary care also faces certain important challenges, among which the epidemiological transition in the chronic diseases, the decentralization of the health system and the erosion of the financing of the health.
References
- Berwick DM. Lessons from developing nations on improving health care. BMJ 2004; 328:1124-1129.
- Belghiti A. The hospital reform in Morocco. Hospital Management Review, Paris 2008; 52-55.
- OCDE. Improving health care performance: How to measure their quality. Éditions OCDE 2011.
- WHO. World report on world health 2000 - for a successful health system. WHO, Genève 2000.
- Sharon J. Performance measure in primary care. Canadian Family Physician 2008; 54:9.
- Grimmer. An evidence-based framework to measure quality of allied health care. Health Research Policy and Systems 2014.
- Kohn LT. To err is human: Building a safer health system. A report of the committee on quality of health care in America, Institute of Medicine. National Academy Press, Washington, DC 2000.
- Amadou B. Strengthening health systems in the countries of the WHO African region: Responding to the challenge. WHO Regional Office for Africa, Health Systems and Reproductive Health, Brazzaville 2007.
- Veillard J. International health system comparisons: From measurement challenge to management too. Performance Measurement for Health System Improvement 2010.
- Piligrimiené Z. Different perspective on Health care quality is the consensus possible. Engineering Economics 2008.
- Belghiti A. Quality assurance in health for an integrated vision. 38th Conference of l’INAS 2013.
- Ministry of Health Morocco. Quality Conference Morocco. Marrakech 2002.
- Shortell SM, Jones RH, Rademaker AW. Assessing the impact of total quality management and organizational culture on multiple outcomes of care for coronary artery bypass graft surgery patients. Med care 2000; 38:207-17.
- Flocke SA, Miller WL, Crabtree BF. Relationships between physician practice style, patient satisfaction and attributes of primary care. J FAM Pract 2002; 51: 835-840.
- Miles MB, Huberman MA. Analyse des données qualitatives. De Boeck, Paris 2003.
- Mukamurera J, Lacourse F, Couturier Y Des avancées en analyse qualitative: Pour une transparence et une systématisation des pratiques. Recherches Qualitatives 2006; 26 :110-138.
- Contandriopoulos AP. A framework for overall assessment of the performance of health service systems: The mode EGIPSS, Reasersh Repport 2008.
- Shortell SM, O'Brien JL, Carman JM, Foster RW, Hughes EF, et al. Assessing the impact of continuous quality improvement/total quality management: Concept versus implementation. Health Services Research 1995; 30:377-401.
- Pomey MP, Contandriopoulos AP, François P, Bertrand D. Accreditation as a tool for organizational change. Int J Health Care Qual Assur 2004; 17:113-124.
- Paccioni AS Accreditation of front-line health services: The start of a new organizational culture? Society Science Journal 2009; 26:117-133.
- Fadi El-Jardali, Diana Jamal, Hani Dimassi, Walid Ammar, Victoria Tchaghchaghian. The impact of hospital accreditation on quality of care: Perception of Lebanese nurses. International Journal for Quality in Health Care 2008; 20:363-371
- Pourtois JP, Desmet H. Postmodern education. Presses Universitaires de France 2002; 326.
- Adair C. Performance measurement systems in health and mental health services: Models, practices and effectiveness a state of the science review. Adair 2003.
- Ovretveit A. Evaluation of quality improvement programs. Qual Saf Health Care 2002; 11:270-275.
- David G, Jeffrey B. Health sector accreditation research: A systematic review. International Journal for Quality in Health Care 2008; 20:172-183
- Charles S. Evaluating accreditation. International Society for Quality in Health Care and Oxford University Press 2003; 455-456.
- Benson LA, Boyd A, Walshe K. Learning from CHI: The impact of healthcare regulation. MCHM, Manchester 2004.
- Ovretveit J. Leading improvement. Journal of Health Organization and Management 2005; 19.
- Devkaran S. International healthcare accreditation: An analysis of clinical quality and patient experience in the UAE. Edinburgh Business School, Heriot-Watt University, CPHQ 2014.
- Starfield B. Primary care and equity in health: The importance to effectiveness and equity of responsiveness to peoples' needs. Humanity & Society 2009; 33:56-73.
- Margaret E. Assessing health system performance in developing countries. University de Michigan 2008.
- Silva B (2011) For a holistic approach to assessing the use of health services: Concepts and measures. Pratiques et Organisation des soins volume 2011; 42.
- Greenfield D. Health sector accreditation research: A systematic review International Journal for Quality in Health Care 2008; 20:172-183
- Pineault R. Accessibility and continuity of health services: A study on the front line in Quebec. Reaserch report, Montréal 2008.
- Kringos DS, Boerma W, Hutchinson A, van der Zee J, Groenewegen P. The breadth of primary care: A systematic literature review of its core dimensions. BMC HSR 2010; 10:65-78.
- Bueton SA. Accreditation of general practices:challenges and lessons. Qual saf Health Care 2003; 2:129-135.
- Marie-Pascale P. Does accreditation stimulate change? A study of the impact of the accreditation process on Canadian healthcare organizations. Implementation Science 2010.
- Seada AM. Impact of hospital accreditation on quality of care as perceived by nursing staff in King Khaled Hospital in Najran at Kingdom of Saudi Arabia. J Am Sci 2012; 8:308-315.
- Radnor Z. Lean a failed theory for public service? Public Management Review 2012; 0:1-23.
- Brasure A. Quality oversight: Why are rural hospitals less likely to be JCAHO accredited? The journal of Rural Health 2000.
- Charron-latour J. Facteurs clés d’une démarche d’amélioration continue durable dans les établissements de santé du Québec. Université de Montréal 2014.
- Groene O. A systematic review of instruments that assess the implementation of hospital quality management systems. Int J Qual Health Care 2013; 525.
- Rodríguez R. Apport des systèmes de gestion de la qualité à la sécurité du patient : Revue internationale. Pratiques et Organisation des Soins 2012; 43:205-214.
- HAS. Analyse de la littérature sur l’impact des démarches de certification des établissements de santé. Paris 2010.
- Douguet and Muñoz (2005) Les effets de la mise en oeuvre de la politique d’amélioration de la qualité dans les établissements de santé: Entre certitude et contrainte Université de Bretagne Occidentale. Brest Atelier de Recherche Sociologique EA3149.
- Nabitz U. The EFQM excellence model : European and Dutch experiences with the EFQM approach in health care: European foundation for quality management. Int J Qual health care 2000; 191-201.
- El-Jardali F, Hemadeh R, Jaafar M, Sagherian L, El-Skaff R, et al. The impact of accreditation of primary healthcare centers: Successes, challenges and policy implications as perceived by healthcare providers and directors in Lebanon. BMC Health Services Research 2014; 14:86.
- Ovretveit J. An integrated health and social care organisation in sweden: Creation and structure of a unique local public health and social care system. Health Policy 2010; 97:113-121.

