Keywords
Carcinoma, Pancreatic Ductal; Pancreatic Neoplasms; Pancreaticoduodenectomy
Abbreviations
AJCC: American Joint Committee on Cancer; CSP: Cancer Surveillance Program; ICD: International Classification of Diseases; NCCN: National Comprehensive Cancer Network; NCI: National Cancer Institute; SEER: Survival Epidemiology and End Results
INTRODUCTION
Of the approximate 40,000 patients diagnosed in the USA with pancreatic cancer in 2008, nearly 41% of these patients presented initially with metastatic disease [1]. Unfortunately, the vast majority of all patients are expected to succumb to their disease with poor median survival of 5-6 months [2]. For the fortunate few patients, surgical resection remains a hope for the only means of cure for pancreatic adenocarcinoma. Specifically, curative-intent surgery (i.e., pancreatectomy) has been reserved for patients with localized disease [3, 4, 5, 6]. Palliative biliary or duodenal bypass remains an appropriate option and is reserved for symptomatic patients with locally advanced, unresectable disease; but pancreatic resection has been uniformly discouraged in patients presenting with metastases.
Previous institutional series have evaluated the role of pancreatic resection in the management of patients with metastatic disease; and no survival benefit from resection was reported [7, 8, 9]. Not surprisingly, many governing bodies have maintained strict guidelines discouraging the performance of pancreatic resection with known metastatic disease. Both the National Comprehensive Cancer Network (NCCN) and National Cancer Institute (NCI) treatment guidelines consider metastatic disease a contraindication to pancreatectomy and recommend all patients be referred for systemic therapy or enrollment in clinical trials [10, 11]. Despite such guidelines, the physicians in our tertiary referral center have anecdotally observed major pancreatic resection in patients with known metastatic disease. Our objective was to determine the incidence and subsequent outcomes of pancreatic resection in the setting of known American Joint Committee on Cancer (AJCC) Stage IV disease.
MATERIALS and METHODS
California Cancer Registry: Los Angeles County Cancer Surveillance Program
The Cancer Surveillance Program (CSP) of Los Angeles County [12] is the largest regional registry participating in the Survival Epidemiology and End Results (SEER) database and serves as a model for population-based cancer registries. This cancer registry has collected patient data from all facilities that diagnose or treat cancer for residents of Los Angeles County since 1972. In 1988, the registry became unique to SEER by expanding its data collection to include comprehensive cancer treatment information including chemotherapy and radiotherapy information. The CSP registry was queried to examine county-wide pancreatic cancer outcomes.
Patient Population and Study Design
Patients (n=9,634) diagnosed with histologically proven adenocarcinoma of the pancreas in Los Angeles County during the time period of 1988-2006 were identified from CSP. Patients less than 18 years of age or with absent surgical or staging data were excluded to yield the final study cohort of 8,549 patients. Patients were then categorized by the presence (n=4,649) or absence (n=3,900) of metastatic disease, which was determined by pathologic staging. The final study cohort was obtained after stratifying for patients who underwent pancreatic resection in the setting of known metastatic disease (n=92).
Tumor location, histology, staging and differentiation were coded according to the International Classification of Diseases (ICD) for Oncology [13]. Topography codes for pancreatic cancer included ICD site codes C25.0-C25.9 and were classified as head (C25.0), body (C25.1), tail (C25.2), and other or not otherwise specified (C25.3-25.9). Pancreatic adenocarcinoma histology codes included mucinous adenocarcinoma, adenocarcinoma with metaplasia, intraductal carcinoma, clear cell adenocarcinoma, papillary adenocarcinoma, granular cell (mixed cell) adenocarcinoma, tubular adenocarcinoma, and adenocarcinoma not otherwise specified. The site specific surgical codes included: partial pancreatectomy (with and without duodenectomy), total pancreatectomy (with and without subtotal gastrectomy with duodenectomy), extended pancreatectomy and pancreatectomy not otherwise specified. The CSP does not provide site specific surgical codes for metastatectomy, making data on the incidence and extent of such procedures unavailable for analysis. Prior to 2004, staging data was reported by CSP as local, regional or distant; from 2004, AJCC staging was available. Patients staged by CSP as either distant or M1 were considered metastatic; and patients with local, regional or M0 disease were considered non-metastatic. Receipt of chemo- and radio-therapies was categorized as positive or negative.
ETHICS
City of Hope and State of California institutional review boards’ approval was obtained for query of the CSP database.
STATISTICS
The principal prognostic factor of interest was pancreatic resection. Extent of disease was categorized as metastatic (M1) or non-metastatic (local or regional). Differences in these clinical and pathologic factors were compared by Student’s t-test for continuous variables, Pearson chi-square test for nominal categorical variables, liner-by-linear chisquare test for ordinal categorical variables, and Fisher’s exact test for dichotomous variables. We performed an analysis to determine whether pancreatic resection impacted survival in patients with M1 disease. The primary outcome of interest was overall survival. Survival was calculated in months from the date of pancreatic cancer diagnosis until the date of death. Patients were censored at the last follow-up date (i.e., April 13th, 2008) or the date the patient was last known to be alive. Median survival was estimated using the Kaplan-Meier method [14], with comparisons made by Wilcoxon log-rank test. P-values were twosided and values less than 0.05 were considered to be statistically significant. We utilized SPSS version 12 (SPSS Inc., Chicago, IL) for our statistical analyses.
RESULTS
Patients with Pancreatic Adenocarcinoma in Los Angeles County
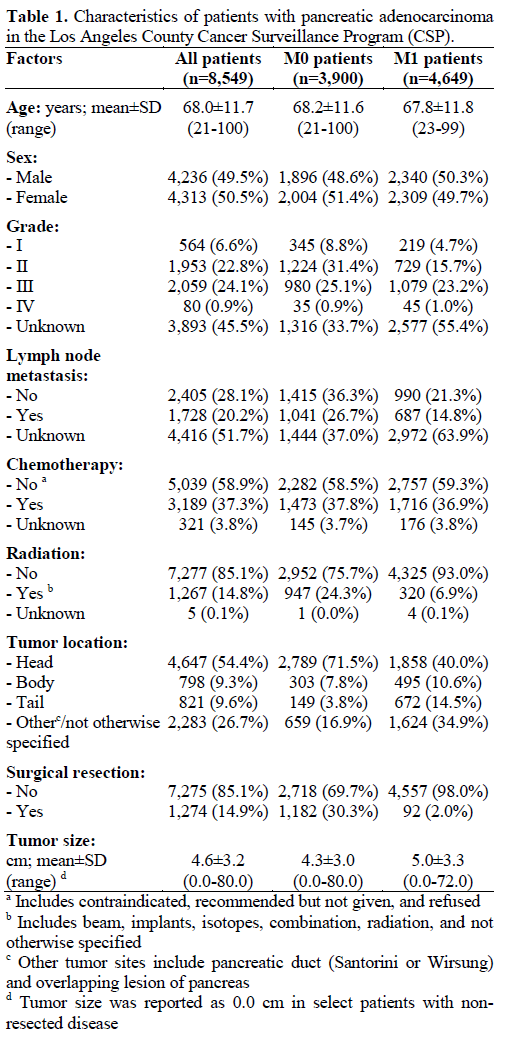
The characteristics of the 8,549 patients with pancreatic adenocarcinoma in Los Angeles County are presented in Table 1. Only 14.9% of these patients (n=1,274) underwent surgical resection in the management of their pancreatic cancer. This rate of surgery in Los Angeles County is consistent with national trends [6]. From the initial cohort (n=8,549), 4,649 patients (54.4%) presented with M1 disease. Two-percent (n=92) of patients with M1 disease underwent pancreatic resection, which comprises 7.2% of the 1,274 pancreatic resections performed for the initial cohort. Of these 92 patients, metastatic disease was determined preoperatively or intraoperatively, and confirmed by pathologic examination. Delivery of chemotherapy in conjunction with surgery was similar regardless of M status (entire cohort: 3,189, 37.3%; M0 cohort: 1473, 37.8%; M1 cohort: 1,716, 36.9%; P=0.716).
Comparison of Treatment Strategies for Patients with M1 Disease
We compared the clinical and pathologic characteristics of patients with M1 disease who underwent surgical resection with patients who were medically treated without surgical resection (Table 2). Treatment was unknown in 175 patients (3.8%) of the non-resection cohort. Out of the 4,382 non-resected patients, 2,606 patients (59.5%) were treated supportively without chemotherapy or radiation, and 1,683 patients (38.4%) received chemotherapy without surgical resection. Radiation therapy was delivered to a small minority of patients (n=300, 6.8%) in the nonresection cohort either with (n=207) or without (n=93) chemotherapy.
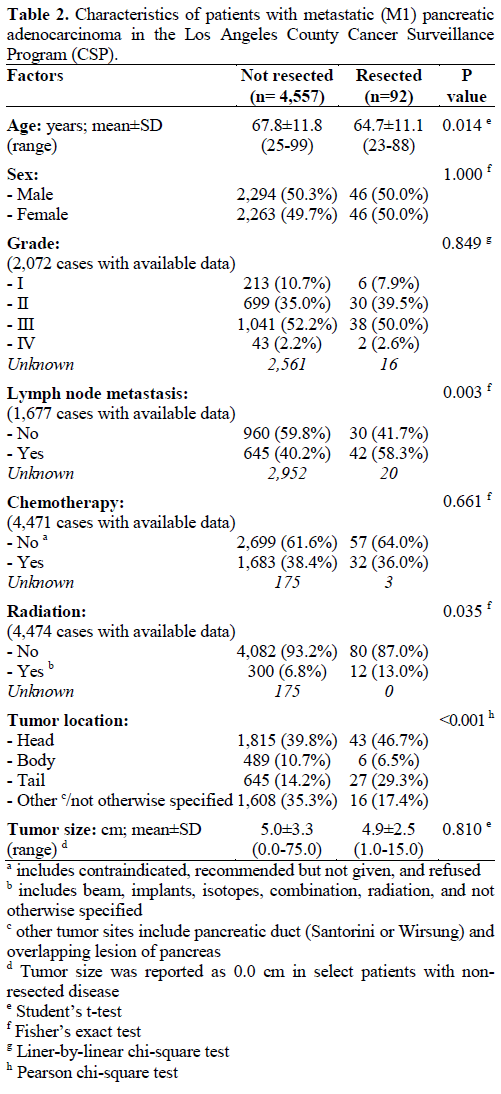
Patients who underwent pancreatic resection compared to no resection were significantly younger (64.7 vs. 67.8 years, respectively; P=0.014) and more likely to receive radiation therapy (13.0% vs. 6.8%, respectively; P=0.035). In addition, tumor location was more frequently in the pancreatic tail for patients who underwent pancreatic resection (29.3% vs. 14.2%, respectively; P<0.001). There was no significant difference in gender, tumor grade or tumor size between the two groups.
Survival of the M1 Cohort According to Therapy
Median survival for the entire M1 cohort was 2.6 months. Median survival in M1 patients not receiving chemotherapy or surgical resection (n=2,606) was 1.6 months. As seen in Figure 1, when stratified by treatment, median survival was 4.9 months for patients who received chemotherapy alone (n=1,683) versus 6.3 months for patients who underwent pancreatic resection with or without the addition of chemotherapy (n=92) (P<0.001). However, the median survival for surgical resection alone (n=57) was similar to the outcomes observed with chemotherapy alone (4.7 vs. 4.9 months, respectively; P=0.095, Figure 2). A small number of surgical resection patients (n=32) received additional chemotherapy and their median survival was 9.0 months. The addition of radiotherapy to surgical patients (plus/minus adjuvant chemotherapy: 12 out of 92 patients) did not impact survival (median survival: 6.1 vs. 6.3 months, respectively; P=0.742).
Figure 1. Survival analysis of M1 patients with pancreatic
adenocarcinoma who received chemotherapy alone (n=1,683) as
compared to patients who underwent pancreatic resection with or
without the addition of chemotherapy (n=92). (MS: median survival).
Figure 2. Comparison of survival in M1 pancreatic adenocarcinoma
patients who received either chemotherapy alone (n=1,683) or
surgical resection alone (n=57). (MS: median survival).
Because we were unable to compare performance status using the CSP, we evaluated 30-day mortality as a surrogate for treatment tolerance and level of function. In patients who underwent neither surgery nor chemotherapy, 30-day mortality was 34.1% (921/2,699) while in the chemotherapy alone cohort the 30-day mortality was 5.8% (98/1,683; P<0.001). Interestingly, in the surgery cohort, 30-day mortality of the surgery alone and surgery with chemotherapy cohorts was 17.5% (10/57) and 0% (0/32), respectively (P=0.012).
DISCUSSION
Given the dismal prognosis of patients with metastatic pancreatic adenocarcinoma, aggressive attempts to eradicate disease have been reported [7, 8, 9]. Here, we identified 4,649 CSP patients who presented with metastatic pancreatic cancer during our study period. median survival of this cohort was a mere 2.6 months with, and only 37% of patients received systemic chemotherapy. The surprisingly low utilization of systemic chemotherapy in M1 patients with pancreatic adenocarcinoma is consistent with national trends. In an evaluation of the National Cancer Database over a 10-year period, Sener et al. reported a 23% incidence in chemotherapy administration among patients with metastatic pancreatic adenocarcinoma [15]. These treatment patterns highlight the prevailing nihilism towards patients with this disease and the typical poor performance status of patients with advanced pancreatic adenocarcinoma. The apparent increase in chemotherapy delivery in our patient population as compared to the National Cancer Database likely represents changes in chemotherapeutic options over the two study periods. In Sener et al.’s study, 100,313 patients spanning all stages of pancreatic adenocarcinoma were evaluated from 1985 to 1995 [15]. Our study period of 1988-2006 is likely more representative of the current national treatment patterns for chemotherapy delivery. Prior to 1997, fluoropyrimidine based therapies were the standard of care for patient with M1 pancreatic adenocarcinoma, despite marginal improvements in survival over supportive therapy. In 1997, Burris et al. reported a randomized controlled trial of 126 patients with advanced pancreatic adenocarcinoma randomized to bolus 5-FU versus gemcitabine and established superiority of gemcitabine over 5-FU in terms of clinical benefit response and progression free survival with a marginal improvement in overall survival [16]. Unfortunately, despite numerous studies which have attempted to improve upon the results of gemcitabine monotherapy for advanced pancreatic adenocarcinoma using either cytotoxic combination therapy or the addition of biologic therapy, the 5.65 month median survival with gemcitabine monotherapy in Burris’s report has not been improved [17, 18, 19, 20, 21, 22, 23, 24, 25, 26]. This is consistent with the 4.9 month median survival of M1 patients receiving chemotherapy alone in our report.
In contrast to systemic agents, pancreatic resection has an established role in the treatment of localized pancreatic cancer and provides the only chance of cure [27, 28, 29, 30] Due to refinements in surgical technique and postoperative care over the past 20 years, pancreatectomy can be performed with acceptable morbidity and minimal mortality [4, 5, 30]. The arguable rationale behind proposing pancreatic resection for patients with metastatic disease may include the improved perioperative outcomes following pancreatic surgery and the continuing frustration with failures of systemic therapy. A growing international experience of metastatectomy for non-colorectal gastrointestinal malignancies, as well as, the apparent success of palliative pancreaticoduodenectomy in the presence of gross residual disease [31], have also been cited as rationale for pancreatectomy with known metastatic pancreatic adenocarcinoma [7, 8, 9].
We have reviewed the published reports of pancreatic resection in the setting of metastatic pancreatic adenocarcinoma. Takada et al. [7] described their series of 11 patients with limited metastatic hepatic disease who underwent simultaneous hepatic resection with pancreaticoduodenectomy and compared them to a matched cohort who did not undergo aggressive therapy. They observed no difference in survival between the two groups (median survival 6 vs. 4 months, respectively, P NS). In a similar casecontrolled study, Gleisner et al. [8] identified 22 patients who underwent pancreatic resection and concomitant hepatic metastatectomy for metastatic periampullary cancer. The median survival of this cohort was 6.9 months. Finally, Shrikhande et al. [9] reported their series of 29 patients with metastatic pancreatic adenocarcinoma to either liver, peritoneum, or the aortocaval node basin who underwent pancreatic resection and metastastectomy. Overall survival was 13.8 and 15.8 months in the surgery only and surgery plus adjuvant chemotherapy groups, respectively. These results, however, remain an outlier and are significantly longer than any report evaluating potential therapies for metastatic pancreatic cancer.
Here, we identified 92 patients with metastatic pancreatic adenocarcinoma from the heterogeneous Los Angeles County population who underwent pancreatic resection in the management of their disease. This is the largest series of patients reported to have undergone resection in the presence of metastatic pancreatic adenocarcinoma. In our series, the outcomes following surgical resection (median survival 6.3 months) are consistent with the survival data reported from trials investigating systemic chemotherapy in patients with metastatic pancreatic cancer [16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26].
The most pertinent comparison in this series is between patients who underwent pancreatic resection in the presence of metastatic disease and patients who received systemic chemotherapy alone for their metastatic disease. These two cohorts likely represent a patient population with relatively comparable performance status. When these two groups were compared, surgical resection provided improved survival for a period of 5 weeks. When one considers the prolonged recovery from pancreatic resection necessary to tolerate subsequent chemotherapy coupled with the significant perioperative mortality associated with pancreatic resection, this survival difference, while statistically significant, becomes clinically irrelevant. The 30-day mortality of 18% in the surgery alone cohort emphasizes the challenges associated with proposing aggressive surgical therapy in the setting of metastatic pancreatic adenocarcinoma. Patients receiving both chemotherapy and surgery had a 4- month increase in survival over those treated with chemotherapy alone, along with no 30-day mortalities. These 32 patients likely represent a highly selected population with low volume metastatic disease and outstanding performance status. However, it must be noted that 57 patients were unable to receive chemotherapy in addition to pancreatic resection. Unfortunately, we were unable to determine what factors contributed to the failure to receive chemotherapy in this cohort. Considering the morbidity associated with pancreatic resection and the high perioperative mortality in this cohort, we suspect that postoperative morbidity limited subsequent treatment options. When the 57 patients who underwent surgery alone were compared to those receiving chemotherapy alone, no survival benefit existed with neither cohort having a median survival greater than 5 months.
We acknowledge inherent limitations in our current database investigation. For example, we were not able to determine the site or extent of metastatic disease, nor were we able to specifically identify the surgical approach (if any) taken towards the metastatic disease. Furthermore, we cannot specify whether the diagnosis of metastatic disease was known preoperatively or determined intraoperatively or if metastatectomy was performed in conjunction with pancreatic resection. It is likely that patients undergoing surgery for metastatic pancreatic adenocarcinoma had more limited disease and better performance status than those treated with systemic therapy or supportive care alone.
We were unable to quantify the performance status of our cohorts. It is expected that only patients with optimal performance status were offered pancreatic resection, and this limits the relevance of direct comparison between the surgical cohort and the other cohorts. While we evaluated 30-day mortality as a surrogate of performance status and treatment tolerance, early mortality is only one of several parameters necessary to quantify performance status and can be affected by extent of disease as well. Nevertheless, the clinical importance of performance status in patients with M1 pancreatic adenocarcinoma cannot be overstated. In a meta-analysis evaluating the efficacy of gemcitabine combination regimens for patients with advanced pancreatic adenocarcinoma, Heinemann et al. not only verified that performance status is one of the most important determinants of survival, but also showed that performance status determined which patients would benefit from more aggressive chemotherapeutic regimens [24]. We should expect that the survival advantage of a surgical cohort with M1 disease relies as heavily on individual performance status as extent of disease. These limitations in selection bias give further credence to the conclusion that a modest 5-week survival advantage in the surgical cohort, while statistically significant, is likely the result of selection bias.
Our study results are also noteworthy in that a large number of patients received no form of therapy, resulting in a median survival of 1.6 months. Current improvement in median survival, has been shown to have palliative benefit in patients with metastatic pancreatic cancer [16]. Given the potential implications of not receiving systemic therapy for metastatic disease because of disabling complications from pancreatic surgery coupled with the perioperative mortality associated with pancreatectomy in the setting of metastatic pancreatic adenocarcinoma, the decision to offer surgical resection must be approached with considerable caution. It is certain that progress in the treatment of metastatic pancreatic cancer has been slow over the past few decades, but we cannot advocate the continued performance of aggressive, experimental strategies outside the confines of a clinical trial that bear no impact on this highly lethal disease. Our findings validate both the NCCN and NCI treatment guidelines for metastatic pancreatic cancer and suggest that clinician education remains critical in the proper management of patients with pancreatic adenocarcinoma.
Conflict of interest The authors have no potential conflict of interest
References
- Jemal A,Siegal R, Ward E, Hao Y, Xu J, Murray T, Thun M.
Cancer Statistics 2008. CA Cancer J Clin 2008; 58:71-96. [PMID
18287387]
- Nieto J, Grossbard M, Kozuch P. Metastatic pancreatic cancer
2008. Is the glass less empty? Oncologist 2008; 13:562-76. [PMID
18515741]
- Neoptolemos J, Stocken D, Freiss H, Bassi C, Dunn J, Hickey H,
et al. A randomized trial of chemoradiotherapy and chemotherapy
after resection of pancreatic cancer. N Engl J Med 2004; 350:1200-
10. [PMID 15028824]
- Winter J, Cameron J, Campbell K, Arnold M, Chang D,
Coleman J, et al. 1423 pancreaticoduodenectomies for pancreatic
cancer: a single institution experience. J Gastrointest Surg 2006;
10:1199-210. [PMID 17114007]
- Wagner M, Redaelli C, Lietz M, Seiler C, Friess H, Buchler
MW. Curative resection is the single most important factor
determining outcome in patients with pancreatic adenocarcinoma. Br
J Surg 2004; 91:586-94. [PMID 15122610]
- Shaib Y, Davila J, Naumann C, El-Serag H. The impact of
curative intent surgery on the survival of pancreatic cancer patients: a
U.S. population-based study. Am J Gastroenterol 2007; 102:1377-82.
[PMID 17403071]
- Takada T, Yasuda H, Amano H, Yoshida M, Uchida T.
Simultaneous hepatic resection with pancreato-duodenectomy for
metastatic pancreatic head carcinoma: does it improve survival?
Hepatogastroenterology 1997; 44:567-73. [PMID 9164539]
- Gleisner A, Assumpcao L, Cameron J, Wolfgang C, Choti M,
Herman J, et al. Is resection of periampullary or pancreatic
adenocarcinoma with synchronous hepatic metastasis justified?
Cancer 2007; 110:2484-92. [PMID 17941009]
- Shrikhande S, Kleeff J, Reiser C, Weitz J, Hinz U, Esposito I, et
al. Pancreatic resection for M1 pancreatic ductal adenocarcinoma.
Ann Surg Oncol 2006; 14:118-27. [PMID 17066229]
- National Comprehensive Cancer Network. NCCN Clinical
Practice Guidelines in Oncology (NCCN Guidelines™). Pancreatic
Adenocarcinoma. V.I.2010. Fort Washington, PA, USA. (Accessed
Oct 6, 2009).
- National Cancer Institute. Pancreatic Cancer Treatment (PDQ®).
Health Professional Version. Bethesda, MD, USA. (Accessed Oct 6,
2009).
- Kim J, Mailey B, Senthil M, Artinyan A, Sun C, Bhatia S.
Disparities in gastric cancer outcomes among Asian ethnicities in the
USA. Ann Surg Oncol 2009; 16:2433-41. [PMID 19582508]
- World Health Organization. ICD-O: International Classification
of Diseases for Oncology, 3rd Ed. (ICD-O-3). Geneva, Switzerland:
World Health Organization, 2000.
- Kaplan EL, Meier P. Nonparametric estimation from incomplete
observations. J Am Stat Assoc 1958; 53:457-81.
- Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic
cancer: a report of treatment and survival trends for 100,313 patients
diagnosed from 1985-1995, using the National Cancer Database. J
Am Coll Surg 1999; 189:1-7. [PMID 10401733]
- Burris H, Moore M, Anderson J, Green M, Rothenburg M,
Modiano M, et al. Improvements in survival and clinical benefit with
Gemcitabine as first-line therapy for patients with advanced pancreas
cancer: a randomized trial. J Clin Oncol 1997; 15:2403-13. [PMID
9196156]
- Sultana A, Smith C Cunningham D, Starling N, Neoptolemos J,
Ghaneh P. Meta-analyses of chemotherapy for locally advanced and
metastatic pancreatic cancer. J Clin Oncol 2007; 25:2607-15. [PMID
17577041]
- Yip D, Karapetis C, Strickland A, Steer C, Goldstein D.
Chemotherapy and radiotherapy for inoperable advanced pancreatic
cancer. Cochrane Database Syst Rev 2006; 3:CD002093. [PMID
16855985]
- Heinemann V, Boeck, S Hinke A, Labianca R, Louvet C. Metaanalysis
of randomized trials: evaluation of benefit from
gemcitabine-based combination chemotherapy applied to advanced
pancreatic cancer. BMC Cancer 2008; 8:82. [PMID 18373843]
- Moore M, Goldstein D, Hamm J, Figer A, Hecht J, Gallinger S,
et al. Erlotinib plus gemcitabine compared to gemcitabine alone in
patients with advanced pancreatic cancer: a phase III trial of the
National Cancer Institute of Canada Clinical Trials Group. J Clin
Oncol 2007; 25:1960-6. [PMID 17452677]
- Philip PA, Benedetti J, Fenoglio-Preiser C, Zalupski M, Lenz H,
O'Reilly E, et al. Phase III study of gemcitabine plus cetuximab
versus gemcitabine in patients with locally advanced or metastatic
pancreatic adenocarcinoma SWOG S0205 study. J Clin Oncol 2007;
25(18 Suppl):LBA4509.
- Kullmann F, Hollerbach S, Dollinger M, Harder J, Fuchs M,
Messmann H, et al. Cetuximab plus gemcitabine/oxaliplatin
(gemocet) in first-line metastatic pancreatic cancer: a multicentre
phase II study. Br J Cancer 2009; 100:1032-6. [PMID 19293797]
- Kindler HL, Niedzwiecki D, Hollis D, Oraefo E, Schrag D,
Hurwitz H, et al. A double-blind, placebo-controlled, randomized
phase III trial of gemcitabine plus bevacizumab versus gemcitabine
plus placebo in patients with advanced pancreatic cancer: a
preliminary analysis of Cancer and Leukemia Group B (CALGB)
80303. J Clin Oncol 2007; 25(18 Suppl):4508.
- Saif M. New developments in the treatment of pancreatic cancer.
Highlights from the '44th ASCO Annual Meeting'. Chicago, IL,
USA. May 30 - June 3, 2008. JOP. J Pancreas (Online) 2008; 9:391-
7. [PMID 18648128]
- Ko AH, Dito E, Schillinger B, Venook AP, Xu Z, Bergsland EK,
et al. A phase II study evaluating bevacizumab in combination with
fixed-dose rate gemcitabine and low-dose cisplatin for metastatic
pancreatic cancer: is an anti-VEGF strategy still applicable? Invest
New Drugs 2008; 26:463-71. [PMID 18379729]
- Van Cutsem E, Vervenne W, Bennouna J Humblet Y, Gill S,
Van Laethem J, et al. Phase III trial of bevacizumab in combination
with gemacitabine and erlotinib in patients with metastatic pancreatic
cancer. J Clin Oncol 2009; 27:2231-7. [PMID 19307500]
- Schelldorfer T, Ware A, Sarr M, Smyrk T, Zhang L, Qin R, et al.
Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg 2008; 247:456-62.
[PMID 18376190]
- Riall T, Cameron J, Lillemoe K, Winter J, Campbell, Hruban R,
et al. Resected periampullary adenocarcinoma: 5-year survivors and
their 6- to 10-year follow up. Surgery 2006; 140:764-72. [PMID
17084719]
- Ferrone C, Brennan M, Gohen M, Coit D, Fong Y, Chung S, et
al. Pancreatic adenocarcinoma: the actual 5-year survivors. J
Gastrointest Surg 2008; 12:701-6. [PMID 18027062]
- Balcom J IV, Rattner D, Warshaw A, Chang Y, Fernandez-del
Castillo C. Ten-year experience with 733 pancreatic resections:
changing indications, older patients, decreasing length of
hospitalization. Arch Surg 2001; 136:391-8. [PMID 11296108]
- Lillemoe K, Cameron J, Yeo C, Sohn T, Nakeeb A, Sauter P, et
al. Pancreaticoduodenectomy. Does it have a role in the palliation of
pancreatic cancer? Ann Surg 1996; 223:718-28. [PMID 8645045]



