Keywords
Rheumatoid arthritis; Social work; Psychosocial problems; Psychosocial treatment; Somatic healthcare
Introduction
The importance of social work in healthcare is often underestimated even though social work can provide knowledge and skills that healthcare organizations and institutions could use to help their patients. Patients with health problems often experience personality and social environment difficulties while trying to manage their disease, especially chronic diseases. The overall goal of social work in healthcare is to prevent and reduce negative social and psychosocial consequences of diseases and to encourage and teach these patients how to use their own resources. This work includes helping individuals find strategies to cope with the difficulties of living with a chronic disease [1].
Social case work was introduced by Mary Richmond (1922) in the early 1920s, but lately the case work approach has been a forgotten theoretical ground of social work [2,3]. In social case work, the focus is on a ‘social diagnosis’ identifying the social process of personality adaptation based on the continued interaction with social environment [4]. Today, the biopsychosocial model of health is generally accepted within humanities and health professions [5,6]. Engel who introduced and developed this model, concluded that illness and health are the result of an interaction between biological, psychological, and social factors [7]. This recognition that these interactional factors influence health has contributed to valuing social aspects in rehabilitation and care.
Rheumatoid arthritis
Affecting more women than men, rheumatoid arthritis (RA) is a chronic inflammatory disease with a prevalence of about 0.5-0.7% in the adult Swedish population [8,9]. Over the past 20 years, treatment for people with early RA has improved dramatically as a result of early interventions with diseasemodifying anti-rheumatic drugs (DMARDs) and new biological medications [10]. Nevertheless, patients with RA face several challenging problems, such as pain, stiffness, fatigue, and decreased muscle strength [11]. Today’s strategies of early treatment and new drugs have led to reduced disease activity and less disability. However, disability and restrictions are still present in RA [12-14].
Rheumatoid arthritis and psychosocial consequences
RA is often associated with psychosocial problems and reduced quality of life [15-17] showed that almost 50% of newly diagnosed RA patients had psychosocial problems directly related to the disease. In addition they found that RA diagnosis at a young age was associated with psychosocial problems although other studies found that being diagnosed with RA at a younger age was not a risk factor for psychosocial problems. Research has also shown that depression and anxiety are more common in patients with RA compared with the general population [18-20]. In addition to the experienced psychological problems mentioned, depression is a well-known complication of RA and is more common than in the general population [21]. These studies suggest that social, psychosocial and psychological consequences of RA remain in spite of the progress in medical treatment. In a recent study of emotions and participation restriction in early RA [22], men and women were asked about their negative emotions (e.g. hopelessness and sadness) when trying to perform daily activities. These participants experienced anger or irritation related to domestic and employed work. The study participants also reported being unable to continue valued activities. Some of them noted that they were angry with their health professionals, managers, or work colleagues for not understanding the extent of their challenges [22]. Research also shows that both men and women may find it difficult to share their emotions, especially as they relate to intimate relationships, about living with RA and this reluctance to share their emotions includes their interactions with their health care providers [23,24].
Living with a chronic disease means learning to live under new circumstances and has a significant impact on daily life and family life [25]. The psychosocial implications of RA are similar to those of other chronic diseases, including the difficulty of maintaining social roles and relationships. A recent study showed that emotional reactions such as coping patterns and psychosocial consequences seemed to be quite similar when comparing RA and diabetes, however, the risk of depression was found higher in early stages of RA [26]. Lack of social support was found to be a predictor of depression and anxiety in people with RA, so researchers suggest that social support may buffer distress in early RA [27,28].
Social work in healthcare
Social work in healthcare is performed in a medical context; that is, the medical social worker needs to collaborate with the medical professionals who usually treat patients. Social work in healthcare is also regulated by healthcare legislation and not solely by social laws [29]. Social work in healthcare in Sweden is performed by medical social workers trained in crisis treatment, psychosocial treatment, counselling, law, how to handle traumas and how to provide social assistance, emotional support, and instrumental support [30].
The interventions used by medical social workers in healthcare include counselling using psychological methods or psychosocial treatment, social support, and social guidance. Most often the prefix “psycho” and not the word “social” alone is used to reflect the complexity of the professional knowledge used even though patients’ problems most often derive from a mix of social, psychological and medical circumstances interacting with each other [6]. However, psychological methods include a focus on intra-psychic processes, whereas psychosocial treatment focuses more on the social situation and the context. Psychosocial treatment may also include interventions where information is delivered to the patient as well as the patient’s relatives [31]. This concept has been extensively discussed in the National Board of Health and Welfare. From this perspective, Öjehagen and Fahlke [32] describe psychosocial treatment as a systematic, structured approach to work with current life problems manifested socially and/or psychologically (e.g. difficulties in relationships or social problems) with the aim to make changes. A Swedish definition of psychosocial treatment is systematic and targeted measures conducted with a psychosocial approach are intended to prevent or to treat the patients in their own context. These interventions are often done by a medical social worker and are theoretically grounded in network and system theory and psychodynamic theory [33]. However, psychological treatment in Sweden is often done by psychologist or psychotherapists based on cognitive behavioural theory or psychodynamic theory [32] or working with families using a network and systemic perspective. In Sweden, professionals such as medical social workers, psychologists, physicians, and nurses can specialize in a particular theoretical perspective by continuing their education in psychotherapeutic techniques that can eventually result in a psychotherapist certification.
Psychological treatments usually rely on formalized theoretical perspectives when identifying or treating a patient’s symptoms. However, psychosocial treatments usually include cooperating with the user on the main goal of treatment and identifying the individual’s basic problems related to everyday life and the social situation. The relationship with the patient is in focus and theoretical and methodological aspects are tailored to the user instead of pre-determined by the professional, the approach of most psychological treatments [34]. In addition, psychosocial treatment focuses on helping the patient find the pre-existing strengths and resources to handle their disease or disability. Social guidance and information is not seen as a treatment but as complementary support systems to psychosocial treatment or psychological treatment [6]. Social guidance includes assessing living conditions, restoring social situations, and receiving help with authority or network contacts, information, and advice on welfare issues. In psychosocial counselling with people experiencing trauma, the individual receives support based on the theory of different stages of the crisis to facilitate the process of acceptance [35]. In addition, patients could receive psychosocial treatment that will help them cope with receiving a chronic disease diagnosis such as RA [36,37].
Social work with patients with chronic disease
When analysing psychosocial problems and chronic disease, psychosocial problems can be divided into two categories: problems that are caused by the disease and social and/or psychosocial problems that already exist before the onset of the disease and that become an obstacle to the adaption of living with the disease. Typically, patients diagnosed with RA also have other problems regarding their health and/or social situation, an observation that is line with previous research by Hawe and Shiell [38] they found a correlation between chronic disease and social problems. Obviously, clinical practice not only should identify whether patients have problems other than those directly connected to the actual diagnose but also should be aware of that the co-existence of multiple problems that might indicate that a patient is in need of different types of support using different strategies. Several population-based studies have shown that vulnerable individuals in one area (e.g. health problems and illness, limited financial resources, and weak social relationships) more often also have problems in other areas (SOU 2000:41 SOU 2000:41). Especially weak economic resources have turned out to be a strong indicator for the existence of problems within other areas and this pattern is particularly common among young people [39]. Taken together, there are several arguments for keeping biological, psychological and social problems as part of the same context and that patients can benefit from psychosocial treatment within healthcare.
This study examines whether a two year psychosocial treatment with patients identified as having psychosocial problems in an early stage of RA can prevent escalating difficulties and facilitate acceptance of the disease. This study describes the development of psychosocial needs and the efficiency of psychosocial treatment in individuals newly diagnosed with RA.
Issues
What type of psychosocial problems did the individuals in a group of patients newly diagnosed with RA have?
To what degree were the psychosocial problems related to the disease?
What type of psychosocial treatment did the patients receive?
To what extent were the psychosocial treatment goals achieved?
Materials and Methods
Patients (18-65 years old) with a new diagnosis of RA at the Department of Rheumatology at the Karolinska University Hospital in Stockholm were invited to participate in the study [16]. Those fulfilling the inclusion criteria (i.e., with a new diagnosis of RA according to the American College of Rheumatology (ACR) 1987 classification criteria) [40] were recruited. To be included in the study patients had to speak Swedish well enough to understand and complete several questionnaires and be able to participate in sessions with a medical social worker. Altogether, 123 patients (90 women and 33 men) were asked to participate in the study although 23 patients declined, so the final number of participants was 100 patients.
A structured interview was conducted to detect psychosocial problems among the patients. The interview and the clinical detection of problems were made by an experienced medical social worker who was not part of the study and who had extensive clinical experience in identifying and treating psychosocial problems. The interviewer, with the consent of the patient, assessed whether the patient had psychosocial problems. If problems were identified, they were further classified as originating primarily from his/her life conditions in general, as pre-existing (i.e., existing before RA diagnosis), or as difficult social and/or psychosocial conditions. Psychosocial problems were further classified into the following groups: (a) negative psychological reaction to the diagnosis that might affect the patient’s ability to adapt to living with RA and worsen the social consequences of the disease (e.g., family/partner relationships, and ability to work); (b) existing social and/or psychological problems with no direct relationship to RA; and (c) difficult social and/or psychosocial conditions that might be worsened by the consequences of RA. Psychosocial problems were separated into domains (e.g. family, work and personal finances).
Of the 100 patients, 41 (34 women and seven men) exhibited psychosocial problems and all of them were interested in meeting with a medical social worker although five patients decided not to meet one-on-one with a medical social worker but did agree to follow-up telephone calls. All the patients were offered regular sessions with the medical social worker, who was also psychotherapist for the project team, over a 24 month period. Before the sessions started, a treatment plan and goals were compiled in consultation with each patient and these needs determined the number of sessions for each patient. The treatment plan, the consultations, and other interventions were registered using a form specifically designed for the study. The patients who finally accepted to participate in the study provided informed consent. The 41 patients in this study are part of the original study group of 123 patients. Self–reported demographic and social background data of the patients in this study are shown in Table 1.
| Men |
7(17%) |
| Women |
34(83%) |
| Mean age, years (SD) |
44.4(11.2) |
| Marital Status |
|
| Married |
13(32%) |
| Unmarried |
15(37%) |
| Divorced/Widowed |
13(32%) |
| Living with Partner |
21(51%) |
| Living alone |
17(42%) |
| Living with other |
3(7%) |
| Educational Level |
|
| Compulsory School |
12(32%) |
| High School |
15(41%) |
| University |
10(27%) |
| Employment Status |
|
| Employed |
22(54%) |
| On early pension/Long term sick leave |
14(34%) |
| Other |
5(12%) |
Table 1: Self-reported demographic background of the 41 patients included in this study: Baseline.
All 123 patients were also asked to complete the following questionnaires: Epidemiological Investigation on Rheumatoid Arthritis study (EIRA), The Hospital Anxiety and Depression Scale (HADS), Sense of Coherence (SOC) and the General Coping Questionnaire (GCQ). The questionnaires were completed at baseline (three months after RA diagnosis) and after the treatment (24 months after first treatment session). The results of this part of the study are reported elsewhere [16]. After the study, the participants completed a follow-up questionnaire regarding their experiences and opinions about the social work consultations and their satisfaction with the treatment given by the medical social worker.
This study was approved by the Research Ethics Committee at Karolinska Institute in Stockholm (No. 00-065), ClinicalTrials. gov.identifier: NCT01066130, in accordance with the World Medical Association (WMA) Declaration of Helsinki. All data were presented on a group level to secure the anonymity of the participants and all personal information that could identify participants individually was destroyed when the data analyses were completed.
Results
Almost half (41 of 100) of the newly diagnosed RA patients experienced psychosocial problems. To address these problems, the patients received 24 months of psychosocial treatment and social guidance. The results show three patterns of mixed problems, including the accumulation of problems over time, and to which extent the psychosocial treatment goals were achieved and what social guidance they had received.
Described multi-problems
Most of the RA patients experienced more than one problem such as crisis reaction worries of the future, mental problems, family problems, work-related problems, economic worries or other types of health problems. Three patterns of mixed problems can be recognized among the RA patient’s descriptions: mixed problems related to RA, mixed problems related to the life situation and mixed problems related to a combination of the disease and the life situation. Half (80) of the described mixed problems was related to the newly received RA diagnosis and the other half (70) was related to the patient’s general life situation.
Several patients (17) described mixed problems due to a combination of the disease and their life situation or experienced problems only due to their problems related to RA (15). Nine patients described that the experienced mixed problems were related to their life situation. The type and number of multiproblems that the patients described are shown in Table 2.
| Type of problem |
Group (n=15) with RA related problems |
Group (n=9) with life situation related problems |
Group (n=17) with both RA/life related problems |
Number of problem of each type |
| Problems related to RA |
|
|
|
|
| |
|
|
|
|
| Crisis reaction |
5 |
|
8 |
13 |
| Concern for future |
15 |
3 |
10 |
28 |
| Mental |
2 |
|
1 |
3 |
| Family-related |
|
|
|
|
| Work-related |
8 |
|
5 |
13 |
| Financial |
3 |
|
4 |
7 |
| Other illness |
4 |
5 |
7 |
16 |
| |
|
|
|
|
| Total number of problems |
37 |
8 |
35 |
80 |
| |
|
|
|
|
| Problems before RA diagnosis |
|
|
|
|
| |
|
|
|
|
| Mental |
2 |
7 |
6 |
15 |
| Family-related |
1 |
7 |
14 |
22 |
| Work-related |
2 |
6 |
4 |
12 |
| Financial |
|
4 |
3 |
7 |
| Other |
3 |
5 |
6 |
14 |
| |
|
|
|
|
| Total number of problems |
8 |
29 |
33 |
70 |
Table 2: Type and number of multi-problems (n=150) in a group of newly diagnosed RA patients (n=41).
All of the patients that experienced that their mixed problems were related to the disease also described having concern for future. The patients that described mixed problems related to their living situations such as mental, family-related, work-related and economic problems seem to be problems that had been present before RA diagnosis. Only a few of these experienced living situation problems related to RA (Table 2).
Multi-problems related to RA
Eight patients who related their mixed problems to RA described three to four combined problems such as crisis reaction, mental problems, work-related problems, economic worries or other types of medical problems. These eight patients also experienced concern for future. One of these patients experienced six types of problems. Five patients reported workrelated problems due to RA, three reported economic problems, and three reported health problems other than RA or mental problems before diagnosis (one patient) and after diagnosis (one patient) or as a crisis reaction related to diagnosis (two patients). Moreover, two of these eight patients described having workrelated problems before diagnosis.
Multi-problems related to the life situation
Nine patients reported that their mixed problems were related to their life situation. Five described having four or five mixed problems each. These five patients reported having mental and economic problems before diagnosis or familyrelated and work-related problems. Three patients had other health problems. Two described concern for future.
Combined problems due to RA and the life situation
Several patients (17) experienced a combination of mixed problems concerning both RA and their life situation. Eleven described three to four problems, and one described two problems. The remaining four patients described five problems each. Information is missing in one case. Sex problems were described by one patient of which four were related to RA and two to their life situation. Most the combined mixed problems were related to RA (11 compared to nine).
Psychosocial treatments, psychotherapy and social guidance
To help the RA patients cope with their mixed problems, the patients received psychosocial treatments, psychotherapy, crisis management and social guidance. Psychosocial treatment accommodates various methods. The National Board of Health and Welfare of Sweden [31] defines psychosocial treatment as "treatment that aims to reduce the patient's problems by integrating the individual's experience and handling of his situation with the use of structured scientific methods and if necessary to include social measures". The social interventions included information and guidance related to social insurance issues, work life and economics. The different types of psychosocial treatment measures delivered to RA patients with mixed problems can be viewed in Table 3, most of the participants in this study received more than one treatment measure the total number were 78. For instance psychosocial treatment was received by 32 of the included 41 patients and 28 of the patients received social guidance.
Problem clusters for the eight patients describe
3-4 problems related to RA |
|
| Problems related to RA |
|
| Crisis reaction |
2 |
| Concern for future |
8 |
| Mental |
1 |
| Work-related |
5 |
| Financial |
3 |
| Other illness |
3 |
| Problems before RA diagnosis |
|
| Mental |
1 |
| Work-related |
2 |
| Other |
2 |
Problem clusters for the five patients describe 4-5
problems related to life situation with RA |
|
| Problems before RA diagnosis |
|
| Mental |
5 |
| Family-related |
4 |
| Work-related |
4 |
| Financial |
5 |
| Other |
1 |
| Problems related to RA |
|
| Concern for future |
2 |
| Other illness |
3 |
Problem clusters for the four patients describe 5
problems related to RA and life situation |
|
| Problems related to RA |
|
| Crisis reaction |
4 |
| Concern for future |
2 |
| Mental |
1 |
| Work-related |
1 |
| Other illness |
3 |
| Problems before RA diagnosis |
|
| Mental |
3 |
| Family-related |
4 |
| Financial |
2 |
Table 3: Problem clusters of the 41 patients included in this study.
Psychosocial treatments of multi-problems related to RA
Most (13 of 15) of the patients with mixed problems related to RA received psychosocial treatment. Five of the 15 were in need of crisis management. Six of 15 received a combination of psychosocial treatment and social guidance. Nine patients only received social guidance.
Psychosocial treatment of multi-problems related to the life situation
Of the patients who had reported problems related to the life situation seven received psychosocial treatment, three received psychotherapy and one received a combination of both. Seven of these patients also received social guidance.
Psychosocial treatment of combined problems due to RA and the life situation
Most of the patients (17) described combined problems related to RA and their life situation. The information on treatment method is missing in one case, but the other 16 reported having received psychosocial treatment and 12 received social guidance. Six patients received crisis management, three psychotherapy and one family counselling and most received these treatments in combination with psychosocial treatment. Seven patients received a combination of psychosocial treatment and social guidance.
The treatment goals
Of the 15 patients who related their mixed problems to RA, 14 had completely reached and one had partly reached their goals by the end of their treatment. Only three of the nine patients who related their problems to their life situations reported that their treatment goals were met; four reported that their goals were partly met, and one reported being referred to another caregiver. In the group of patients that related their problems to a combination of RA and their life situation, seven reported that the treatment goals were met, and seven reported they were partly met and three reported that the goals were unmet (Figure 1).
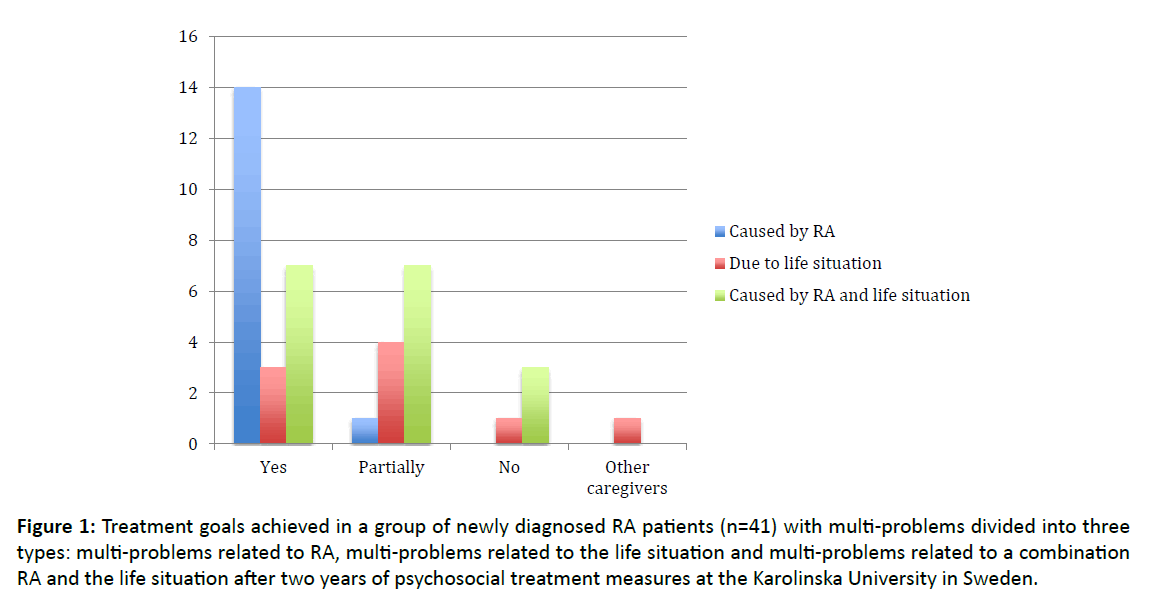
Figure 1: Treatment goals achieved in a group of newly diagnosed RA patients (n=41) with multi-problems divided into three types: multi-problems related to RA, multi-problems related to the life situation and multi-problems related to a combination RA and the life situation after two years of psychosocial treatment measures at the Karolinska University in Sweden.
Discussion
This study explores what kinds of problems patients with newly diagnosed RA reported and what kinds of psychosocial rehabilitation measures they received. The patients also had the possibility to evaluate whether their treatment goals were met. The patients were strategically sampled from a cohort of newly diagnosed RA in which multi-problems were reported by 41 of 123 at the onset of their disease.
The mixed problems reported were related to family, work, economics, psychological problems, or types of health problems other than RA, crisis reactions related to diagnosis, and concern for future. In this sample, three major groups were found based on the origin of the multi-problems experienced according to the patients’ perspectives: mixed problems related to RA, mixed problems related to their life situation, and problems related to a combination of RA and their life situation. Many patients experienced a collection of problems irrespective of the degree of difficulty or frequency of the problems. The psychosocial treatments and rehabilitation measures delivered seemed to be almost general irrespective of group and RA-related mixed problems seemed to be more treatable than problems with other origins from a patient perspective. All the psychosocial treatments focused on the individual’s interaction with the social environment [2-4]. After two years of psychosocial treatment, most of the established treatment goals were achieved for those patients who experienced problems directly related to the newly diagnosed RA. Patients who reported mixed problems due to a combination of RA and life situation also benefited from psychosocial treatment, but to a lesser extent (Table 4).
| Type of psychosocial treatment |
Group (n=15) with RA related problems |
Group (n=9) with life situation related problems |
Group (n=17) with both RA/life related problems. |
Number of social intervention of each type. |
| Psychosocial treatment |
13 |
7 |
12 |
32 |
| Crisis management |
5 |
|
6 |
11 |
| Psychotherapy |
|
3 |
3 |
6 |
| Family counselling |
|
|
1 |
1 |
| Social guidance |
9 |
7 |
12 |
28 |
Table 4: Type and number of psychosocial treatments (n=78) in a group of newly diagnosed RA patients (n=41).
Patients with long-term psychosocial illnesses benefit from treatment plans that establish treatment goals [41]. For Michalak and Holthforth [42], treatment goals should be formulated with the patient, a strategy that makes it more likely that long-term target specific and measurable goal will be achieved within a given time. That is, a good psychosocial care plan benefits all patients regardless of the origin of their problems. Developing treatment goals with patients encourages them to become actively involved in their treatment. Although some of the psychosocial problems of our participants were difficult to treat, all the patients seemed to benefit from establishing treatment goals. However, this study did not focus on disease duration or aggressiveness of the disease, two factors that could influence outcomes.
The present study indicates that RA patients also experience problems in areas that are not directly linked to the disease. We found that patients diagnosed with RA belong to a vulnerable group; they more often have problems in many areas at the same time and their “problem-panorama” is more complex, a finding evident in earlier research [43]. So far, our results cannot be said to be very controversial. On the contrary, they are very much in line with what other studies have concluded [44]. Our results can be related to what has come to be a central question when it comes to equality in living conditions: the dividing line between different diagnostic groups goes between those who experience welfare and satisfactory socioeconomic conditions and those who have a lack of resources and experiences combined with problems related to several life areas [44-46].
We found that some patients reported RA-related problems in their employment situation. This problem has been described before from a patient perspective on work-related dilemmas in early RA. Work-related dilemmas represented different societal perspectives on work related to acquiring, keeping, and terminating a job. Work dilemmas also represented participation priorities in economic self-sufficiency, self-care such as attending to treatment and healthcare, and avoiding social relationships and recreation in favour of work. Leisure time was influenced because work took energy and time, two resources these patients lacked [47].
Patients who identified mixed problems found that their RA issues were complicated by their pre-diagnosis life situation especially as it related to psychological, family or economic problems. Having experienced multi-problems earlier in life influences the possibility of recovery (i.e., meeting one’s treatment goals). Berkanovic et al. [43] found that people of lower socioeconomic status still have poorer health generally, and this is especially true for people diagnosed with RA. None of the patients that experienced four to five mixed problems described suffering from a crisis reaction. This response to RA diagnosis might be understood in light of the patient’s experience with pre-diagnosis problems. That is, the patient’s complex life situation might be worse overall than receiving a RA diagnosis, another unexpected, difficult life experience to manage added onto an already difficult life situation.
Most patients’ mixed problems were described as a combination of RA-related problems and the life situation. Of these situations, half of the problems concerned RA and half were related to a pre-existing strained living situation. The diagnosis and an already strained living situation seemed to mediate and complicate rehabilitation and adaptation. Most of the patients (14 of 17) who understood their problems as of a combined origin reported that they had experienced family problems even before the diagnosis of RA, and these kinds of problems were not as usual in any of the other groups. Even if the RA diagnosis caused a further strain on the existing fragile and strained life situation within the family, the RA diagnosis was seen as just another aspect of their already difficult situation.
It was obvious that the origin of the patient’s mixed-problems was important in terms of achieving treatment goals. After two years of psychosocial treatment, most of the established treatment goals were achieved among individuals whose mixed problems were directly related to the newly diagnosed RA. Individuals who reported problems due to a combination of RA and life situation also benefited from the psychosocial treatment, but to a lesser extent. For the patients experiencing mixed problems due to a life situation, a few believed their treatment goals were achieved. For these patients, the disease in itself may not have been the main problem as RA may have only been an additional source of stress in an already strained life situation.
Targeting goals and goal setting are effective components of treatment in long-term illness [41]. Michalak and Holthforth [42] argue that when targeting long-term specific goals that are achievable within a given time, the goals need to be formulated by the patient. A measurable and objective goal has been shown to affect a patient's willingness to become actively involved in treatment. Although a healthcare professional might define a patient's problems related to rehabilitation, recovery, and adaption to society, patients need to define their treatment goals. Even within healthcare the understanding of diseases differs as either essentially biomedical or social or psychological [29]. The present study indicates that patients with RA experiencing mixed-problems of a combined origin were more difficult to treat successfully in terms of achieving treatment goals. However, this study did not measure disease duration and aggressiveness nor did it weigh the experienced mixed-problems.
The results of this study found that RA patients with diseaserelated mixed-problems should be given priority and the help they receive should be based on achievable treatment goals (Figure 1). On the other hand, some patients with combined problems might need to be transferred to social workers or psychologists with areas of expertise other than medical social work. This study suggests that social work in healthcare is most successful with people whose problems originate from the disease and whose daily life problems were related and were affected by the disease. Individuals with pre-existing vulnerable social situations where the disease implies an extra social burden and causes more external social pressures are much more difficult to successfully treat, a finding also in line with this study’s findings. We found that psychosocial treatment goals seem to be easiest to achieve among RA patients with disease-related problems. Mizhrahi and Berger [48] discussed that the patient’s needs should always be the primary focus of an intervention, and the dilemma for the social worker is that social work is often called to address more than one agenda.
The results of this study highlighted the effect of psychosocial treatment in medical social work for patients with early RA and who experience diseases related to psychosocial problems. Similarly, Dorstyn et al. [49] showed that early psychosocial treatment in patients with chronic diseases prevented psychosocial problems. However, social work resources in the hospital setting are often limited and need to be used as efficiently as possible. In addition to specific professional knowledge, medical social workers need to have some knowledge in the medical field their clients require. Social work in healthcare has been established for more than 100 years and has developed into a major sector of the profession in countries around the world. As a part of the larger social service system and healthcare system, medical social workers are also affected by changes in national and local economics, political power and philosophy, and technology in the larger environment [50,51].
Medical treatment for patients with early RA has improved dramatically as a result of early interventions with diseasemodifying anti-rheumatic drugs (DMARDs) and new biological medications [10]. However, the patients in the present study were treated before this new RA medication, so the positive effect cannot be explained by improved medical treatment, but rather by the psychosocial treatment received shortly after the RA diagnosis. One limitation of the study is of course to discuss about the new effective drugs against RA also affected the individual's problem clusters. To discuss this need a new study, conducted which studies differences and similarities in terms of clusters of problems before and after the DMARDs and new biological medications.We do not know if the patient’s problem clusters have been changed but we assume that as long as the disease is not possible to cure the type of problems will remain, however less comprehensive in the long run.
Conclusion
In conclusion, we found three different types of mixedproblems in this sample of RA patients: problems related to RA, problems related to life situation, and problems related to a combination of the disease and life situation. The patients also had different types and collection of problems irrespective of the degree of difficulty or frequency of the problems.
We also found that RA patients who reported multi-problems at time of the diagnosis received psychosocial treatment from a medical social worker irrespective of the mixed problems they experienced and that the disease-related mixed problems seem more treatable than the other problems. The patient’s evaluation of the origin of the mixed-problems was important in terms of achieving treatment goals. Based on the results of our study, it could be argued that mixed problems related to a chronic disease seem easier to manage than problems without a specific origin. Therefore, social work in somatic healthcare is most successful in patients with sicknesses related to social and psychosocial problems.
Declaration of Interest
The authors report no conflict of interest. The study was financially supported by the Swedish Rheumatism Association.
References
- Miller Fitzergald J. Coping with chronic illness: Overcoming powerlessness. FA Davis, cop, Philadelphia 2000.
- Richmond M. What is social case work? An introductory description. Russel Sage Foundation, New York 1922.
- Fjeldheim S, Levin I, Engebretsen E. The theoretical foundation of social case work. Nordic Social Work Research 2015; 5: 42-55.
- Richmond M. Social diagnosis. Russel Sage House, New York 1917.
- World Health Organization. ICF: International classification of functioning, disability and health. WHO, Geneva 2001.
- Serafino EP Smith TW.Health psychology: Biopsychosocial interactions. Wiley & Sons Inc., New York 2014.
- Engel GL. The clinical application of the biopsychosocial model. Am J Psychiatr 1980; 137: 535-544.
- Simonsson M, Bergman S, Jacobsson LT, Petersson IF, Svensson B. The prevalence of rheumatoid arthritis in Sweden. Scand J Rheumatol 1999; 28: 340-343.
- Söderlin MK, Borjesson O, Kautiainen H, Skogh T, Leirisalo-Repo M. Annual incidence of inflammatory joint diseases in a population based study in southern Sweden. Ann Rheum Dis 2002; 61: 911-915.
- Furst DE, Breedveld FC, Kalden JR, Smolen JS, Burmester GR, et al. Updated consensus statement on biological agents, specifically tumour necrosis factor a (TNFa) blocking agents and interleukin-1 receptor antagonist (IL-1ra), for the treatment of rheumatic diseases. Annals of the Rheumatic Diseases 2005; 64: 2-14.
- Krishnan E, Fries JF. Reduction in long-term functional disability in rheumatoid arthritis from 1977 to 1998: A longitudinal study of 3035 patients. Am J Med 2003; 115: 371-376.
- Neovius M, Simard JF, Klareskog L, Askling J, ARTIS study group. Sick leave and disability pension before and after initiation of anti-rheumatic therapies in clinical practice. Ann Rheum Dis 2011; 70: 1407-1414.
- Björk M, Thyberg I, Rikner K, Balogh I, Gerdle B. Sick leave before and after diagnosis of rheumatoid arthritis: A report from the Swedish TIRA project. J Rheumatol 2009; 36: 1170-1179.
- Björk M, Skogh T, Husberg M, Thyberg I. Reduced Sick leave in today’s early RA patients compared to 10 years ago, the Swedish TIRA project. EULAR, Madrid 2013.
- Geuskens GA, Burdorf A, Hazes JM. Consequences of rheumatoid arthritis for performance of social roles: A literature review. J Rheumatol 2007; 34: 1248-1260.
- Gåfvels C, Hägersten M, Nordmark B, Wändell PE. Psychosocial problems among newly diagnosed rheumatoid arthritis patients. Clin Rheumatol 2012; 31: 521-529.
- Dures E, Almeida C, Caesley J, Peterson A, Ambler N, et al. A survey of psychological support provision for people with inflammatory arthritis in secondary care in England. Musculoskeletal Care 2014; 12: 173-181.
- Dickens C, McGowan L, Clark-Carter D, Creed F. Depression in rheumatoid arthritis: A systematic review of the literature with meta-analysis. Psychosom Med 2002; 64: 52-60.
- Isik A, Koca SS, Ozturk A, Mermi O. Anxiety and depression in patients with rheumatoid arthritis. Clin Rheumatol 2007; 26: 872-878.
- Sharpe L, Sensky T, Timberlake N, Ryan B, Brewin CR, et al. A blind, randomized, controlled trial of cognitive behavioural intervention for patients with recent onset rheumatoid arthritis: Preventing psychological and physical morbidity. Pain 2001; 89: 275-283.
- Covic T, Cumming SR, Pallant JF, Manolios N, Emery P, et al. Depression and anxiety with rheumatoid arthritis: Prevalence rates based on a comparison of the depression, anxiety and stress scale (DASS) and the hospital, anxiety and depression scale (HADS). BMC Psychiatry 2012; 12: 1-10.
- Östlund G, Björk M, Valtersson E,Thyberg M, Thyberg I, et al. Emotions related to participation restrictions as experienced by patients with early rheumatoid arthritis: A qualitative interview study (The Swedish TIRA project). Clin Rheumatol 2014; 33: 1403-1413.
- National Rheumatoid Arthritis Society NRAS. Emotions, relationships and sexuality 2013.
- Östlund G, Björk M, Valtersson E, Sverker A. Lived experiences of sex life difficulties in men and women with early RA: The Swedish TIRA project. Musculoskeletal Care 2015; 13: 248-257.
- Andersson R, Bury M. Introduction in living with chronic illness, the experiences of patients and their families, the academic division of Unwin Hyman, London 1998.
- Gåfvels C, Hägerström M, Rane K, Wajngot A, Wändell PE. Coping strategies among patients newly diagnosed with diabetes or rheumatoid arthritis at baseline and after 24 months. J Health Psychol 2016; 29.
- Zyrianova Y, Kelly BD, Gallagher C, McCarthy C, Molloy MG, et al. Depression and anxiety in rheumatoid arthritis: The role of perceived social support. Ir J Med Sci 2006; 175: 32-36.
- Strating MM, Suurmeijer TP, van Schuur WH. Disability, social support and distress in rheumatoid arthritis: Results from a thirteen year prospective study. Arthritis Rheum 2006; 55: 736-744.
- Blom B, Lalos A, Morén S, Olsson M. Health and medical care - A central arena for social work in the book Social work in health and medical care; Terms of content and challenges. Nature and Culture, Stockholm 2014.
- Gåfvels C, Rane K, Wajngot A, Wändell PE. A Follow-up two years after diagnosis of diabetes in patients with psychosocial problems receiving intervention by a medical social worker. Soc Work Health Care 2014; 53: 584-600.
- The National Board of Health and Welfare. National guidelines: Care and support in abuse and dependence. Support for Management and Management 2015.
- Öjehagen A, Fahlke C. Support for differentiating psychosocial treatment and psychological treatment. In Investigation while working on national guidelines. Care and Support in Addiction and Addiction 2015.
- Bernler G, Johnsson L. Theory for pyschosocial work, Stockholm. Nature and Culture 2012.
- Bower P, Knowles S, Coventry PA, Rowland N. Counselling for mental health and psychosocial problems in primary care. Cochrane Database Syst Rev 2011; 7: CD001025.
- Cullberg J. Crisis and development, Fourth edn. Nature and Culture, Stockholm 2003.
- Lazarus RS, Folkman S. Stress, appraisal and coping. Springer Publishing Company, New York 1984.
- Michel PO, Johannesson KB, Lundin T, Nilsson D, Otto U. Psychotraumatology, Studentlitteratur, Lund 2010.
- Hawe P, Shiell A. Social capital and health promotion: A review. Soc Sci Med 2000; 51: 871-855.
- Angelin. The double power of attorney's logic: A study of long-term unemployment and social inclusion among young adults. Lund dissertations in social work, Lund University, Lund 2009.
- Levin RW, Park J, Ostrov B, Reginato A, Baker DG, et al. Clinical assessment of the 1987 American College of Rheumatology criteria for rheumatoid arthritis. Scand J Rheumatol 1996; 25: 277-281.
- Schwartz L, Drotar D. Defining the nature and impact of goals in children and adolescents with a chronic health condition: A review of research and a theoretical framework. J Clin Psychol Med Settings 2006; 13: 393-405.
- Michalak J, Holtforth MG. Where do we go from here? The goal perspective in psychotherapy. Clin Psychol Sci Pract 2006; 13: 346-365.
- Berkanovic E, Oster P, Wong WK, Bulpitt K, Clements P, et al. The relationship between socioeconomic status and recently diagnosed rheumatoid arthritis. Arthritis Care and Research 1996; 9: 257-262.
- Travers P, Richardson S. Living decently. Material well-being in Australia. Oxford University Press, Oxford 1993.
- Michael W. Pluralism and equality: A theory of just distribution (Pluralism and Equality). Daidalos, Gothenburg 1993.
- Sen A. Inequality re-examined. Harvard University Press, Cambridge/MA 1992.
- Sverker A, Thyberg I, Östlund G, Valtersson E, Thyberg M. Participation in work in early rheumatoid arthritis: A qualitative interview study interpreted in terms of the ICF. Disability and Rehabilitation 2014; 36: 242-249.
- Mizrahi T, Berger C. Effect of changing health care environment on social work leaders: Obstacles and opportunities in hospital social work. Soc Work 2001; 46: 170-182.
- Dorstyn DS, Mathias JL, Denson LA. Psychosocial outcomes of telephone-based counselling for adults with an acquired physical disability: A meta-analysis. Rehabil Psychol 2011; 56: 1-14.
- Rachman R. Community care; changing the role of hospital social work. Health Soc Care Commun 1995; 3: 163-172.
- Globerman J. Hospital restructuring: Positioning social work to manage change. Soc Work Health Care 1999; 28: 13-30.

