Keywords
sleep apnea, screening tools, heart failure
How this fits with quality in primary care
What do we know?
Heart failure patients are at risk for sleep apnea. This sleep disordered breathing may affect their survival and quality of life. Sleep studies are ordered as needed, but can be expensive.
What does this paper add
Describes the types of sleep apnea, the variety of screening tools for sleep apnea and provides evidence for advising providers to screen all patients with heart failure for sleep apnea with both a screening tool and pulse oximetry before ordering the gold standard sleep study.
Introduction
According to the Centers for Disease Control (CDC) approximately 5.1 million people in the United States have a diagnosis of heart failure and half will die within five years of diagnosis.[1] Heart failure is characterized by its high mortality, frequent hospitalizations and a reduced quality of life with estimates of costs to the nation reach $37 billion each year.[2] There is accumulating evidence that nocturnal breathing disorders are important modifiers of disease progression in patients with heart failure. Sleep-disordered breathing, or sleep apnea is the most common comorbidity in heart failure patients, occurring in over half of heart failure patients and can exacerbate the illness.[3,4]
Review of the Literature
A review of the literature using the keywords heart failure, sleep apnea, treatment, and screening in the CINAHL and PubMed databases was completed. Research studies that evaluated apnea screening and/or treatment were reviewed. Three major treatment modalities and three screening tools emerged for both types of sleep-disordered breathing.
Sleep apnea is defined as a combination of hypopnea (slow, shallow breathing for 10 seconds or more) and apnea (cessation of breathing for 10 seconds or more) that results in a decrease in blood oxygen saturation.[5] Improving morbidity and mortality in heart failure patients involves assessing factors such as sleep disordered breathing that impact the progression of the disease. Several types of sleep-disordered breathing have been identified in the heart failure population including obstructive sleep apnea, central sleep apnea, and complex sleep apnea syndrome. [6,4]
Types of Sleep Apnea
Obstructive sleep apnea affects approximately 35% of heart failure patients and is caused by partial or complete collapse or obstruction of the upper airway.[4] It causes a change in intrathoracic pressure and an increased sympathetic drive resulting in a cascade of physiological changes including decreased cardiac output, increased myocardial oxygen demand, vasoconstriction, hypertension, and activation of the renal renin-angiotensin system.
Central sleep apnea is more complex and difficult to treat, as its cause is the temporary withdrawal of the brainstemdriven respiratory drive.4 A distinct pattern of Cheyne-Stokes respiration is present in central apnea or hypopnea followed by hyperventilation in a cyclic crescendo-decrescendo pattern resulting in an oscillation of arterial carbon dioxide above and below the threshold for apnea.
Complex sleep apnea involves repeated episodes of central apnea during treatment with CPAP in patients who initially present with obstructive apnea. It is more difficult to treat and may need a higher level of ventilator support than CPAP such as adaptive sero-ventilation.[7] Identification of the type of sleep apnea and treatment in heart failure patients is critical to improving the outcomes. [8]
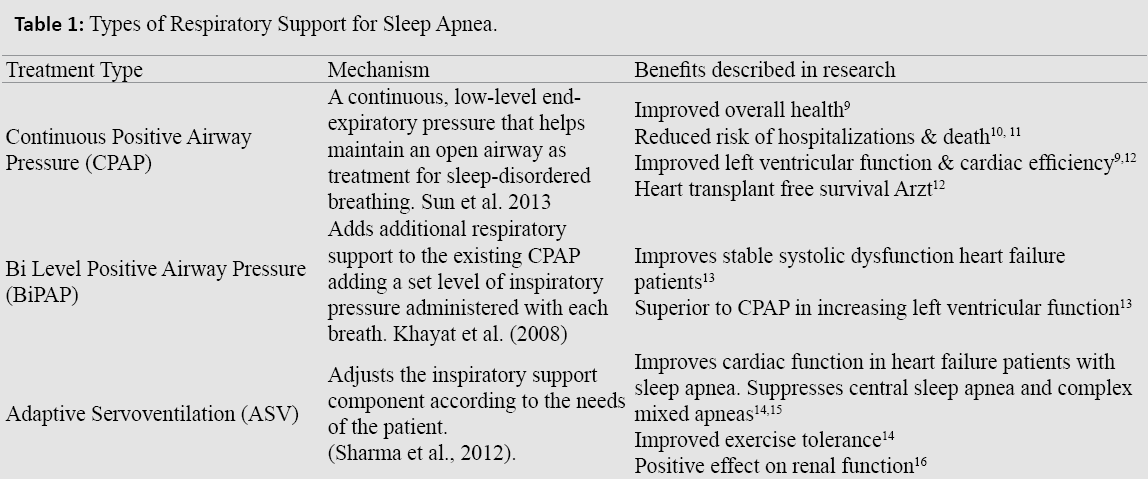
Continuous Positive Airway Pressure (CPAP)- The effects of CPAP is a continuous, low-level end-expiratory pressure to helps maintain an open airway as treatment for sleep-disordered breathing. A meta-analysis determined that CPAP improves left ventricular function (LVEF) in those patients with both obstructive sleep apnea and documented heart failure.[9]
Bi-level Positive Airway Pressure (BiPAP) -The benefit of this therapy is that it adds additional respiratory support to the existing CPAP adding a set level of inspiratory pressure administered with each breath. Khayat et al. (2008) compared the use of CPAP in treatment of obstructive sleep apnea to the use of BiPAP in improving stable systolic dysfunction heart failure patients and found it to be superior to CPAP in increasing left ventricular function.[13]
Adaptive Servoventilation (ASV) -Adaptive servoventilation (dynamic BiPAP) adjusts the inspiratory support component according to the needs of the patient. Although CPAP has been shown to improve cardiac function in heart failure patients with sleep apnea, it has been unsuccessful in suppressing central sleep apnea in nearly 50% of treated patients.[14] Research supports the use of ASV for the suppression of central sleep apneas as well as mixed apneas in the heart failure patient. Arzt et al. (2008) studied heart failure patients with central and complex sleep apneas and, ASV was found to have the greatest reduction in the apnea (Table 1).[17]
Screening Tools
Several screening tools have been designed to identify sleep apnea in a variety of populations. A review of the literature with specific emphasis on diagnosing sleep apnea in the heart failure population revealed three tools most commonly used: the Epworth Sleepiness Scale, the STOP-Bang Equivalent Model, and the Berlin Questionnaire (Appendices 1-3).
1. Epworth Sleepiness Scale (ESS) A review by Rosenthal & Dolan (2008) to assess the sensitivity of the ESS in identifying obstructive sleep apnea was conducted on patients screened with the tool with a subsequent sleep study.[18] Epworth scores were analyzed in comparison to apnea index greater than or equal to five and it was determined that the screening tool alone had a fair discriminatory ability as a screener for obstructive sleep apnea.
2. The STOP-Bang model was considered the simplest to use and score. A systematic review of obstructive sleep apnea screening questionnaires by reviewed 10 studies aimed at screening for SDB concluded that such screening tools are associated with promising results.[19] Farney et al. (2011) conducted a study using the STOP-Bang Equivalent model (SBM) and its ability to predict obstructive sleep apnea in comparison to the sleep study to further classify obstructive sleep apnea into categories ranging from none to severe.[20] With STOP-Bang scores of 6-8 there was a high probability of being diagnosed with obstructive sleep apnea via sleep study.
3. The Berlin Questionnaire (BQ) sleep apnea screening tool was evaluated as to its sensitivity and specificity compared to the gold standard PSG sleep study as a diagnostic tool. A retrospective review of 130 sleep-clinic patients to determine its effectiveness found the BQ to have moderate specificity and low sensitivity in correctly diagnosing sleep apnea.[21] A metaanalysis of multiple screening tests for obstructive sleep apnea found the Berlin Questionnaire to be one of the most accurate questionnaires.[22]
Combining both a sleep-screening tool and overnight pulse oximetry has proven useful. Garner & Traverse (2014) implemented an evidence-based protocol to screen for sleep apnea in a heart failure disease management clinic.[23] Utilizing a screening tool, and overnight pulse oximetry test was clinically beneficial and cost effective in this population. Another study found significantly favorable results in diagnosing apnea after confirmation by sleep study, in their patient population when compared to using the screening tool alone.[23] It was noted however, a high number of false negatives were found with all screens, including the BQ with the least accurate screen thought to be the ESS due to the plethora of other causative factors for daytime sleepiness.[21,22]
Synthesis of the Evidence
This review supports the need for screening, diagnosis, and treatment of sleep-disordered breathing in the heart failure population. Untreated severe sleep disordered breathing has been found to have a statistically significant increased risk of all cause mortality. [24] Although using an overnight sleep study in a sleep lab is considered the gold standard for diagnosis of sleep-disordered breathing, such a study can be time-consuming and costly.
Evidence-based screening tools such as The Epworth Sleepiness Scale (ESS) (Appendix 2), which measure subjective daytime sleepiness, or The STOP-Bang Questionnaire (Appendix 3), which assesses risk factors for obstructive sleep apnea, should be used to screen those at highest risk for sleepdisordered breathing in the heart failure population. Despite the research consensus that such screens have inconsistencies and a high rate of false-positive results, when used in conjunction with a secondary screen of higher sensitivity and specificity such as overnight oximetry identification of patients with a true diagnosis of sleep apnea becomes more likely.[18,20,21&25] These patients could then be referred for a formal sleep study if needed to confirm or refute sleep apnea based on a positive, multi-leveled screen.
Healthcare insurance companies are more likely to cover the cost of sleep studies in the presence of an oximetry study indicative of periods of hypoxia. Later confirmation of suspected diagnosis through PSG, the gold standard, has proven this screening protocol to be an effective method for identifying and diagnosing sleep apnea in the heart failure population.[23] Once the long-term goal of complete protocol screening has been implemented and treatment instituted, long-term compliance with sleep apnea treatment can be reinforced by noting the patients verbalization of improved symptoms, improved screening scores, or by means of repeat echocardiogram (ECHO) which could possibly show documented improvement of heart function.
Garner & Traverse (2013) studied the health behaviors and sleep apnea treatment adherence in the heart failure patient and found that non-compliance was highest in the elderly and in women for various reasons such as the prospect of an overnight sleep study outside of the home, being “too old” for evaluation and treatment, complications with other diagnoses, and cost.[27] For those who underwent PSG evaluation; but did not comply with the recommended CPAP treatment, common reasons given were mask intolerance, claustrophobia, and drying of the nose.[27] Ongoing disease education plays a large factor in addressing not only the modifiable risk factors for heart failure as a disease. The resulting compliance to treatment greatly impacts quality of life, heart failure disease progression, and ultimately morbidity and mortality.[28]
Discussion and Conclusion
The implementation and use an evidence-based sleep apnea screening tool, in conjunction with overnight pulse oximetry studies for those who are scored as high risk helps screen at risk patients before the more expensive sleep study and diagnosis of a sleep disordered breathing condition. Sleep apnea in the heart failure population should be approached as a co-existing chronic disease requiring long-term management.
The American Heart Association guidelines state that “Continuous positive airway pressure can be beneficial to increase LVEF and improve functional status in patients with heart failure and sleep apnea” 30
Unfortunately, sleep apnea is not part of the routine evaluation and management of heart failure, so it remains untreated in most patients. Medical providers can play an instrumental role in screening and identifying those patients at highest risk for sleep apnea using an evidence-based screening protocol. Once identified and diagnosed, providers can reinforce the need for disease management and construct an individualized educational plan to increase adherence with recommended therapies.
References
- Centers for Disease Control and Prevention (CDC) Website. 2013
- Aranda JM, Johnson JW, Conti JB. Current trends in heart failure readmission rates: Analysis of Medicare data. Clinical Cardiology 2009;32: 47-52.
- Kasai T, Bradley D.Obstructive sleep apnea and heart failure.Journal of the American College of Cardiology: 2011;57:119-127.
- Khayat R, Small R, Rathman L. et al. Sleep-disordered breathing in heart failure: Identifying and treating an important but often unrecognized comorbidity in heart failure patients. Journal of Cardiac Failure2013;19: 431-444.
- Spieker ED, Motzer SA. Sleep-disordered breathing in patients with heart failure: Pathophysiology, assessment, and management. Journal of the American Academy of Nurse Practitioners2003;15: 487-493.
- Baldwin CM, Ervin A, Mays M Z, et al. Sleep disturbances, quality of life, and ethnicity: The sleep heart health study. Journal of Critical Sleep Medicine2010;6:176-183.
- Allam JS, Olson EJ, Gay PC, Morgenthaler TI. Efficacy of adaptive servo- ventilation in treatment of complex and central sleep apnea syndromes. Chest 2007; 132:1839- 1846.
- Brenner S, Angermann C, Jany B, Ertl G, Stork S. Sleep-disordered breathing and heart failure: A dangerous Liaison. Trends in Cardiovascular Medicine 2008;18:240-247.
- Sun H, Shi J, Li M, Chen, XImpact of continuous positive airway pressure treatment on left ventricular ejection fraction in patients with obstructive sleep apnea: A Meta-analysis of randomized controlled trials. PLoS ONE 2013;8: e62298.
- Hall AB, Ziadi MC, Leech JA, et al. Effects of short-term continuous positive airway pressure on myocardial sympathetic nerve function and energetics in patients with heart failure and obstructive sleep apnea. Circulation2014;130: 892-901.
- Kasai T, Narui K, Dohi T, et al. Prognosis of patients with heart failure and obstructive sleep apnea treated with continuous positive airway pressure. Chest 2008;133: 690-696.
- Arzt M, Floras JS, Logan A. et al Suppression of central sleep apnea by continuous positive airway pressure and transplant-free survival in heart failure: A post hoc analysis of the Canadian continuous positive airway pressure for patients with central sleep apnea and heart failure trial (CANPAP). Circulation 2007; 115: 3173-3180.
- Khayat RN, Abraham WT, Patt B, et al Cardiac effects of continuous and bi-level positive airway pressure for patients with heart failure and obstructive sleep apnea. Chest 2008; 134:1162-1168.
- Sharma BK, Baker JP, McSharry DG et al. Adaptive servo-ventilation for treatment of sleep-disordered breathing in heart failure. Chest 2012;145: 1211-1221.
- Traverse RD. Sleep-disordered breathing in heart failure: Developing an evidence- based screening protocol. Heart & Lung: The Journal of Acute and Critical Care2011;40:370-371.
- Owada T, Yoshihisa A, Yamauchi et al. Adaptive servo-ventilation improves cardio-renal function and prognosis in heart failure patients with chronic kidney disease and sleep-disordered breathing. Journal of Cardiac Failure 2013; 19: 225-232.
- Arzt M, Wensel R, Montalvan, S, et al. Effects of dynamic bi-level positive airway pressure support on central sleep apnea in men with heart failure. Chest 2008; 134: 61-66.
- Rosenthal LD, Dolan DC. The Epworth sleepiness scale in the identification of obstructive sleep apnea. The Journal of Nervous and Mental Disease2008;196: 429-431.
- Abrishami A, Khajehdehi A, Chung F. A systematic review of screening questionnaires for obstructive sleep apnea. Canadian Journal of Anesthesia 2010;57: 423-438.
- Farney RJ, Walker BS, Farney RM, Snow GL, Walker JM. The STOP- Bang equivalent model and prediction of severity of obstructive sleep apnea: Relation to polysomnographic measurements of the apnea/hypopnea index. Journal of Clinical Sleep Medicine: 2011; 7: 459-465.
- Ahmadi N, Chung SA, Gibbs A, Shapiro CM. The Berlin questionnaire for sleep apnea in a sleep clinic population: Relationship to polysomnographic measurement of respiratory disturbance. Sleep Breath 2008: 12: 39-45.
- Ramachandran SK, Josephs LA. A meta-analysis of clinical screening tests for obstructive sleep apnea. Anesthesiology 2009;110: 928-939.
- Garner SL, Traverse RD. Use of an evidence-based protocol to screen for sleep- disordered breathing in a heart failure disease management clinic. Journal of Nursing Care Quality 2014; 29: 230-236.
- Young T, Finn L, Pepperd PE, Szklo-Coxe M, Austin D, Nieto J, Hla M. Sleep disordered breathing and mortality: Eighteen-year follow-up of the Wisconsin Sleep Cohort. Sleep 2008: 31:1071-1078.
- Chung F, Liao P, Elsaid H. et al. Oxygen desaturation index from nocturnal oximetry: A sensitive and specific tool to detect sleep-disordered breathing in surgical patients. Anesthesia & Analgesia: 2012; 114: 993-1000.
- Sommermeyer D, Zou D, Grote L, Hedner J. Detection of sleep disordered breathing and its central/obstructive character using nasal cannula and finger pulse oximeter. Journal of Clinical Sleep Medicine: 2012;8: 527-533.
- Garner SL, Traverse RD.Health behavior and adherence to treatment for sleep breathing disorder in the patient with heart failure. Journal of Community Health Nursing 2013;30:119-128.
- Kazimierczak A, Krzesinski P, Krzyzanowski K, Gielerak G. Sleep-disordered breathing in patients with heart failure: New trends in therapy. BioMed Research International2013; 1-10.
- Yancy CW, Jessup M, Bozkurt B et al. ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology 2013; 62: e147-e239.

