Keywords
Diabetes core measures; Compliance; No show rate; Telephone reminders
Introduction
Diabetes mellitus is the seventh leading cause of death in the United States[1] and as its prevalence continues to grow, its economic burden continues to increase significantly. In 2007, the estimated total cost of diabetes-related care was $174 billion, versus $245 billion in 2012 (a 40.1% increase).[2] Additionally, due to the chronic nature of this disease, continuous and comprehensive monitoring is required for its effective management, i.e., screening patients based on the 2014 American Diabetes Association of Medical Care in Diabetes (ADA) guidelines (Appendix Table 1). These determinations are critical for consistently and effectively reducing patients’ risk and cost of long-term complications.[3] Consequently, adherence to diabetes core measures (DCMs), medications, lifestyle modifications, and follow-up appointments are crucial to disease management; such adherence, however, is often very difficult. When patients are noncompliant in undergoing their laboratory DCMs or do not attend their follow-up appointments, a gap in their medical management is created,[4] eventually leading to decreased quality of life, associated life-threatening diabetes-related complications and increased healthcare costs.[2,5]
Our resident clinic at Beaumont Health (Royal Oak, Michigan) has always struggled with a low compliance rate of diabetic patients with their laboratory diabetes core measures (29% to 36% compliance rate). Moreover, despite an automated dialing appointment reminder system (ADAMS) two days prior to their appointments, the clinic’s overall "no-show" rate is 23%, consistent with other residency programs.[6]
It is well accepted that automated telephone reminders or mailings have been effective in reducing patient "no-show" rates.[7-9] One systematic review revealed that automated telephone reminders reduced the baseline no-show rate by 29- 39%.[10] To our knowledge, however, no study has been taken to evaluate the effect of personalized, vs. mechanized, telephone reminders, for the direct purpose of providing DCMs and attending physician visits.
Previous research firmly indicates that patients with low socioeconomic status most frequently miss appointments.[11-14] Prior research has also demonstrated that "no-show" rates among patients with diabetes range from 4% to 40%.[4,15-19] In addition, numerous studies now demonstrate that diabetic patients with higher "no-show" rates have higher HbA1c levels, compared to patients who regularly attend follow-up appointments.[4,17,19-22] eventually leads gto uncontrolled diabetes mellitus, causing both microvascular and macrovascular complications.5 In fact, diabetes mellitus is the leading cause of kidney failure, non-traumatic lower-limb amputations, and new causes of blindness among adults in the United States,[23] all associated with increased hospitalizations, and poor quality of life.[2,5] Therefore, improving diabetes care is an urgent need, to reduce complications and healthcare-associated cost.
Rationale
The low compliance of diabetic patients with their laboratory DCMs, combined with high "no-show" rates, is a significant barrier to delivering quality medical care, potentially leading to diabetes-related complications and high healthcare-related costs. Thus, we hypothesized that preordering overdue laboratory DCMs and calling noncompliant patients to remind them of their appointments, and also ask them to undergo their overdue laboratory DCMs, would improve compliance with their laboratory DCMs and appointment attendance, allowing medication adjustments and better disease management at the time of the visit, based on the new HbA1c (and other) laboratory results.
Specific Aim
The purpose of this study was to assess our hypothesis that preordering overdue laboratory DCMs combined with personalized telephone reminders would increase patients’ compliance with laboratory DCMs, while also reducing "no-show" rates.
Methods
Study design
This was a cross-sectional, retrospective study that assessed diabetic patients’ compliance with laboratory DCMs, and “"no-show"” rates, between two groups (personalized telephoned vs. non-personalized telephoned).
Setting
Our university-affiliated internal medicine and combined internal medicine and pediatrics residency clinic at Beaumont Health (Royal Oak, Michigan) predominantly serves low-income patients (currently, 4300 out of 8356 total patients are enrolled in a Medicaid plan, representing 51.5% of our general clinic population). The total number of diabetic patients in our clinic is 840 (10% of total clinic population). Our resident clinic has a total of 9 teams, each consisting of 8-9 residents. Each resident has patients assigned to themselves and will also frequently take care of the diabetic patients from their team members. Throughout the three years of training, each resident might be taking care of an average of 100 diabetic patents. Through weekly-generated reports via electronic medical records (EPIC, Verona, WI), diabetic patients with an upcoming appointment were identified for each team. Each report consisted of an average of nine diabetic patients per week. One resident from each team, during their continuity clinic month, was assigned to review each chart from their report. Only patients that were overdue for their laboratory DCMs received a personalized telephone reminder, given by the resident assigned to that report, for that specific week. All overdue laboratory DCMs were preordered by the assigned residents. The patients that were successfully reached by phone were instructed to arrive a half-hour prior to their scheduled appointment, to have their overdue laboratory DCMs done. If a patient was unavailable, a voice message was left with the instructions mentioned above. All the telephone encounters were documented in the electronic medical record of the patients. The patients in both groups also received an automated telephone reminder two days prior to their upcoming appointment, only to remind them about the appointment date and time.
Participants
Study subjects were patients with type 1 or 2 diabetes mellitus, 18 years of age or older, who were overdue for laboratory DCMs per 2014 ADA guidelines, and had a scheduled appointment in our internal medicine and combined internal medicine/pediatrics resident clinic at Beaumont Health, Royal Oak, Michigan, anytime from January 2014 to January 2015. All appointment types were included (e.g. physical exam, follow-up, etc.). Patients younger than 17 years of age, patients with type 1 or 2 diabetes mellitus that were up to date with their laboratory DCMs and patients with appointment cancellations, were excluded from the study.
All the available reports and every eligible patient chart were reviewed in order from January 2014-January 2015; based on the electronic medical record documentation regarding the personalized telephone encounter, the patients were divided into two groups: those who did versus those who did not receive a personalized telephone reminder (Figure 1). The patients in each group were enrolled in chronological order based on medical records review until each group reached a total number of 75 patients.
The reasons why some participants did not receive a personalized telephone reminder, even though they appeared in the reports, were due to: e.g. the resident did not call; the patient’s phone number on record was invalid or disconnected, etc.
Intervention
Our intervention consisted of preordering overdue laboratory DCMs combined with a personalized telephone reminder given the week prior to their appointments.
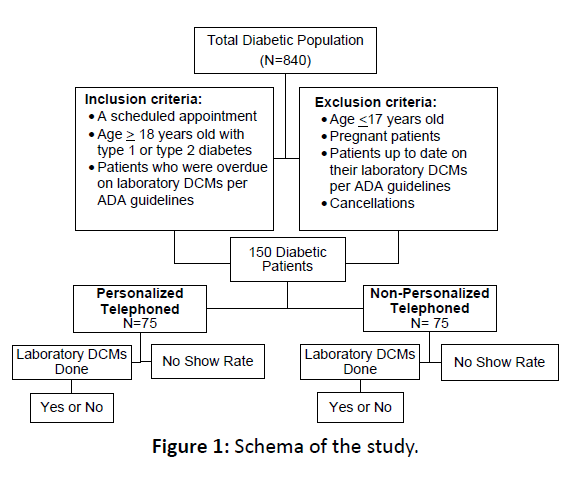
Figure 1: Schema of the study.
Variables
The primary outcome assessed was patient compliance with laboratory DCMs. Compliance was assessed as a “yes” or “no” for laboratory DCMs completed (Figure 1). The secondary outcomes assessed were “"no-show"” rates and HbA1c levels between the two groups. In addition, we reported the mean HbA1c levels and the likelihood of following up with appointments between three insurance groups: 1) governmentalsubsidized; 2) commercial; or 3) no insurance (a possible metric for socioeconomic status).
Data sources
The following data was manually collected via electronic chart review: gender, age, type of insurance, missed appointment(s), baseline HbA1c, and if their laboratory diabetes core measures: Hb1Ac level, fasting lipid profile, serum creatinine and urine microalbumin were done.
Bias
The study population was identified through weeklygenerated reports, thereby reducing the risk of selection bias.
Study size
A sample size of 75 participants in each group was calculated to achieve a power of 81%, with an alpha of <0.05 to detect a 22% difference in the primary outcome between the two (personalized telephoned vs. non-personalized telephoned) groups. This study was approved by Beaumont Health Institutional Review Board and no external funding was received.
Statistical analysis
Descriptive statistics involving the means, medians, standard deviations and proportions, of patient compliance factors, were used as exploratory analysis. Our primary outcome, patients’ compliance with laboratory DCMs, and the secondary outcome, "no-show" rate, among the two telephone contact groups, were assessed through a two-sample z test for proportions, and also were reported as odds ratios with 95% confidence interval via logistic regression analysis. HbA1c levels were compared between the two telephone contact groups, using nonparametric tests (Mann-Whitney), due to the absence of a normal distribution. In addition, Hb1Ac levels among the three insurance groups were compared through a Kruskal-Wallis test of equality of medians. A logistic regression analysis was conducted to determine the effect of insurance type on whether the patients showed up for their appointment or not.
Results
A 150 study participants were included in the statistical analysis, split into two groups of 75 (Figure 1). The average age of patients was 55.96 years, with an SD of 12.25 years. Among the study participants, 42% were male and 58% were female; the majority of patients had governmental-subsidized insurance (72%). Overall, the two groups were similar in terms of baseline demographics (Table 1). Statistical analysis showed a significant increase for laboratory DCMs, 77.33% vs. 14.66% (p<0.001), in the personalized telephoned group vs. non-personalized telephoned group (OR 19.82; 95% CI, 8.59-45.86). The “noshow” rate was also significantly different (18.66% vs. 61.33%, p <0.001) in the personalized telephoned group, compared to non- personalized telephoned group (OR 6.91; 95% CI, 3.28- 14.54).
The mean HbA1c levels were not statistically significant between the two groups: 8.2% (66 mmol/mol) in the personalized telephoned group, vs. 8.45% (69 mmol/mol) in the non-personalized telephoned (p=0.514) (Figure 2). Comparison of Hb1Ac levels among the three insurance groups (private, governmental, or none), as assessed by the Kruskal-Wallis test of equality of medians, was not statistically significant different (p=0.217). Logistic regression analysis of the effect of insurance type on whether the patients’ “no showed” for their appointments yielded a p-value of 0.075, suggesting that at a 5% significance level, there was no correlation between insurance type and the “no-show” rate in this patient population.
Participants in the personalized telephone group were also more likely to have overdue laboratory DCMs ordered by the residents, compared to the non-personalized telephoned group (100% vs. 38.6%, P<0.01).
Discussion
To our knowledge, this study is the first to report a statistically significant impact of preordering laboratory ADA diabetes core measures (DCMs) combined with personalized telephone reminders on obtaining laboratory ADA diabetes core measures (DCMs), while concurrently decreasing the “no-show” rate. Our results showed that patients who had their laboratory DCMs preordered and received a personalized telephone reminder the week prior to their scheduled appointment had a nineteen times higher odds to be compliant with undergoing their laboratory DCMs, and six times higher odds to “show-up” to their appointments, compared to patients who did not receive a personalized telephone reminder.
| Demographics |
Personalized Telephoned Group, N. (%) |
Non-Personalized Telephoned Group, N. (%) |
P value |
| Female, No. (%) |
45 (60%) |
42 (56%) |
0.70 |
| Male, No. (%) |
30 (40%) |
33 (44%) |
0.74 |
| Mean Age |
56.11 |
55.81 |
0.884 |
Insurance
•Governmental
•Private
•Self pay/none |
55 (73.33%)
16 (21.33%)
4 (5.33%) |
53 (70.66%)
10 (13.33%)
12 (16%) |
0.066 |
Table 1: Patient demographics (N=75 per group).
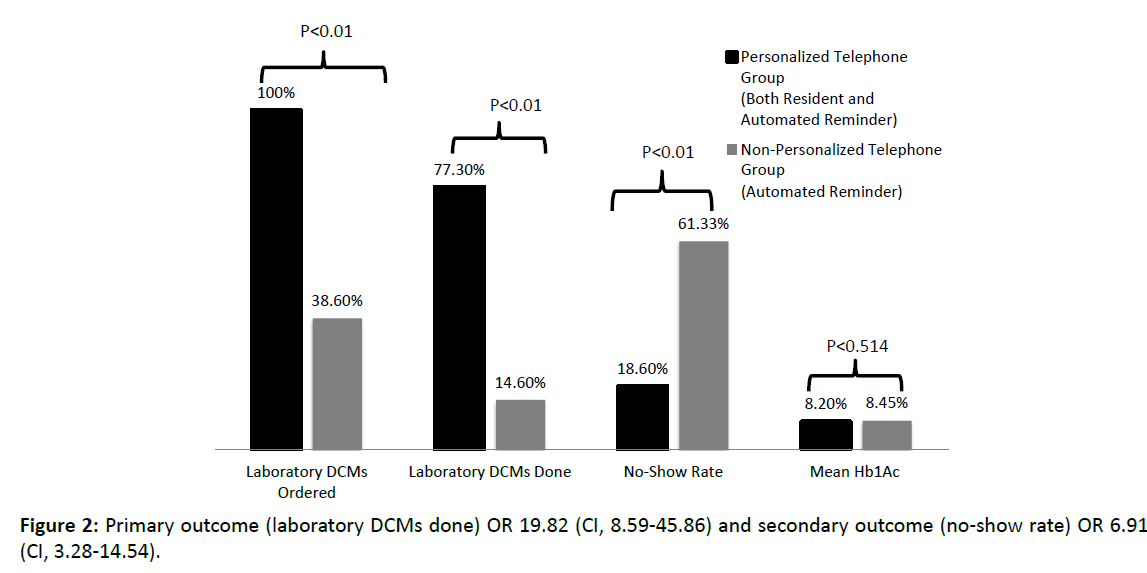
Figure 2: Primary outcome (laboratory DCMs done) OR 19.82 (CI, 8.59-45.86) and secondary outcome ("no-show" rate) OR 6.91 (CI, 3.28-14.54).
The strengths of the study included prognostically balanced groups in terms of demographics, median HbA1c levels, and insurance groups. Also, the sample size provided large enough power to show an effective difference of 22% between the two groups. Thus, the risk of selection bias was minimal, because the two groups were assigned based on the first 150 patients meeting the inclusion/exclusion criteria.
Some limitations of our study exist. One was that we did not extensively assess reasons for no-show, including lack of transportation, “last-minute” time conflicts (for other activities), anxiety over the blood draw, etc. Moreover, while we did examine the effects of insurance status on compliance with laboratory DCMs, we found no significant impact, this could be due to small sample size and possible type II error, as our study was not powered to detect this effect (nor did we include expensive “out-of-pocket” copayments assessment). Since insurance type is not a precise determination for socioeconomic status; therefore we cannot make a definite determination regarding the association. Further studies with adequate power should evaluate the likelihood of this association.
While prior studies reported a decrease in “no-show” rates with various interventions (e.g. telephone reminders, mailings, etc.), we are not aware of any studies specifically looking at personalized telephone reminders, to improve diabetes management. However, prior studies reported a 10% reduced “no-show” rate when comparing clinic staff to automated appointment reminders.9 Our study reports a 42.67% reduction in the “no-show” rate in the diabetes population. While it remains unknown why personalized telephone reminders were effective; perhaps this might associate with one group actually being reminded by two (automated plus human) vs. one (automated only) telephone calls. Additionally, the reminder call was in the previous week, versus two days for the automated call (providing patients more lead time to check time conflicts, etc.) Thus, more extensive study is warranted, with the inclusion of these other variables.
We were very surprised to find a high “no-show” rate (61%) in our diabetic patients, which is much higher than our average clinic “no-show” rate (23%) and diabetes “no-show” rates reported in the literature.[4,15-19] This finding supports our conjecture that diabetic patients may be less compliant with follow-up than the general population. Our higher than average “no-show” rates could possibly be related to location-specific socioeconomics, distinct patient-related barriers (e.g. poor public transportation, crime-prevalent neighborhoods, other comorbidities, and/or lack of current symptoms, etc.), confounding factors worthwhile of investigation in future studies.
Interestingly, we found that residents were more likely to identify and order overdue laboratory DCMs for patients in the personalized telephoned group, compared to the non-personalized telephone group (Figure 2). This finding could be related to the clinical complexity of the office visit for these patients, leading residents to miss the opportunity to order the necessary laboratory diabetes core measures (perhaps related to haste, concurrent duties, etc.). This represents another interesting finding of our study, possibly addressing the issue of “clinical myopia,” a term used to describe the combination of patient non-compliance and healthcare-provider “inertia”.[24]
Although, the cost of personally telephoning patients was not considered in this study, our results are consistent with previous research suggesting that telephoning patients lowers the “no-show” rate and/or increases cancellation, leading to open appointments for other patients.7,8 Moreover, another study (using Medicare and Medicaid reimbursement data) showed that all types of reminder interventions decreased the net (fiscal) loss of 18%, by 3.8-10.5%.25 Thus, nearly all previous studies of this topic demonstrated significantly reduced fiscal loss, due to decreased “no-show” rates facilitated by telephone reminder interventions, resulting in an overall cost benefit and a significant net revenue.[8]
Conclusion
Our study demonstrates that a simple intervention (i.e., preordering DCMs combined with a personalized telephone reminder) had a significant impact on increasing patients’ compliance with laboratory DCMs, while also substantially decreasing “no-show” rates. These parameters are crucial to the chronic management of diabetes mellitus, for the improvement of quality-of-life and decreased complications and mortality. This cost-effective intervention could potentially be implemented at a national level to all medicine residency programs that serve low-income patients. While other prospective studies remain needed to determine if this simple intervention improves HbA1c levels, and has an impact on clinically significant patient outcomes, our current findings hold promise that this approach will lead to improved management of this chronic and lifethreatening disease.
Acknowledgement
The authors thanks Dr. Curt Balch (Bioscience Advising, Ypsilanti, MI) for assistance in preparing the manuscript, and Dr. Vincent Agboto for conducting the statistical analysis. This work was presented at the Society of General Internal Medicine Regional Meeting, September 2016. Cleveland, OH, Michigan Summit on Quality Improvement & Patient Safety Statewide Meeting, June, 2016. Troy, MI and the regional American College of Physicians Meeting, September 2015. Traverse City, MI.
Author Contributions
F.A. and A.H. designed the study, collected data, wrote the manuscript and approved its final version. F.A. and A.H. are responsible for the integrity of this manuscript.
References
- Kochanek KD, Xu JQ, Murphy SL, Minino AM, Kung HCDeaths: Preliminary data for 2009- National vital statistics reportsHyattsville National Center for Health Statistics 2011; 59: 4
- Economic costs of diabetes in the U.Sin 2012Diabetes Care 2013; 36: 1033-1046
- American diabetes associationStandards of medical care in diabetes–2014Diabetes Care 2014; 37:S14-S80
- Schectman JM, Schorling JB, Voss JDAppointment adherence and disparities in outcomes among patients with diabetesJ Gen Intern Med 2008; 23: 1685-1687
- Michael J FowlerMicrovascular and Macrovascular Complications of DiabetesClinical Diabetes2008; 26: 77-82
- Hixon AL, Chapman RW, Nuovo JFailure to keep clinic appointments: Implications for residency education and productivityFam Med1999; 31: 627-630
- Stubbs ND, Geraci SA, Stephenson PL, Jones DB, Sanders SMethods to reduce outpatient non-attendanceAm J Med Sci 2012; 344: 211-219
- Parikh Amay, Kunal Gupta, Alan C WilsonThe effectiveness of outpatient appointment reminder systems in reducing no-show ratesAm J Med123: 542-548
- Hashim MJ, Franks P, Fiscella KEffectiveness of telephone reminders in improving rate of appointments kept at an outpatient clinic:A randomized controlled trialJ Am Board FamPract 2001; 14: 193-196
- Hasvold PE, Wootton RUse of telephone and SMS reminders to improve attendance at hospital appointments: A systematic reviewJournal of Telemedicine and Telecare 2011; 17: 358-364
- Barron WMFailed appointments: Who misses them, why they are missed and what can be donePrim Care 1980; 7: 563-574
- Smith CM, Yawn BPFactors associated with appointment keeping in a family practice residency clinicJ FamPract 1994; 38: 25-29
- Lacy NL, Paulman A, Reuter MD, Lovejoy BWhy we donâ€Âââ€Å¾Â¢t come: Patient perceptions on no-showsAnn Fam Med2004; 2: 541-545
- Frankel S, Farrow A, West RNon-attendance or non-invitation? A case-control study of failed appointmentsBMJ 1989; 298: 1343-1345
- Ciechanowshi P, Russo J, Katon W, Simon G, Lundman E, et al: Where is the patient? The association of psychosocial factors and missed primary care appointments in patients with diabetesGen Hosp Psychiatry2006; 28: 9-17
- Culica D, Walton JW, Prezio EACODE: Community Diabetes Education for uninsured Mexican AmericansProc (BaylUniv Med Cent) 2007; 20: 111-117
- Karter AJ, Parker MM, Moffet HH, Ahmed AT, Ferrara A, et alMissed appointments and poor glycemic control: An opportunity to identify high-risk diabetic patientsMed Care 2004; 42: 110-115
- Hardy KJ, Oâ€Âââ€Å¾Â¢Brien SV, Furlong NJInformation given to patients before appointments and its effect on non-attendance rateBMJ 2001; 323: 1298-1300
- Griffin SJLost to follow-up: The problem of defaulters from diabetes clinicsDiabet Med 1998; 15: S14-S24
- Samuels TA, Bolen S, Yeh HC, Abuid M, Marinopoulos SS, et alMissed opportunities in diabetes management:A longitudinal assessment of factors associated with suboptimal qualityJ Gen Intern Med 2008; 23: 1770-1777
- Rhee MK, Wrenn S, Ziemer DC, Culler SD, Cook CB, et alPatient adherence improves glycemic controlDiabetes Educ 2005; 31: 240-250
- Davidson MB, Karlan VJ, Hair TLEffect of a pharmacist-managed diabetes care program in a free medical clinicAm J Med Qual 2000; 15: 137-142
- Centers for Disease Control and PreventionNational diabetes fact sheet: National estimates and general information on diabetes and prediabetes in the United States 2011
- Reach GPatient non-adherence and healthcare-provider inertia are clinical myopiaDiabetes Metab 2008; 34: 382-385
- BergEstimating the Cost of No-Shows and Evaluating the Effects of Mitigation StrategiesMed Decis Making 2013; 33: 976-985

