Keywords
pay-for-performance, general practice/family practice, number of visits, health care outcomes.
How this fits with quality in primary care
What do we know?
The use of financial incentives to reward family doctors (FD) for improving the quality of primary healthcare services is growing. However, there is insufficient evidence to support or not support the use of financial incentives to improve the quality of primary health care.
There is evidence that payment for performance (P4P) increases workload for FDs and nurses.
The introduction of a major national P4P scheme for primary care in the UK was associated with a decrease in emergency admissions and modest cost-effective reductions in mortality and hospital admissions in some domains. FDs who achieved a good outcome in P4P have better continuity of care for chronic diseases. This situation also reduced the number of specialist consultations. There is a need for more research to determine the effects of payment for performance in healthcare.
What does this paper add?
This paper reflects recent data from Estonia, where P4P was introduced in 2006 and shows increased numbers of visits of FDs and also specialists. A good outcome in P4P reduced hospital bed occupancy and a poor outcome in P4P increased hospital bed occupancy for two chronic conditions (arterial hypertension and diabetes mellitus type 2).
Introduction
Background: Many countries are using financial incentive schemes and clinical quality indicators.[1,2] Payment for performance (P4P) financial incentive schemes reward doctors based on the quality and the outcomes of their treatment. [1-3] Financial incentive schemes are one approach by which the system may incentivise providers of health care to improve productivity and/or adapt to better quality provision.[1] There is still a great need for research to determine the effects, both positive and negative, of P4P in healthcare.[2,3]
In 2006 Estonia started P4P for FDs.2 The P4P was aimed at forcing FDs to pay more attention to prevention and monitoring chronic diseases.[3] P4P consists of three major parts: prevention, monitoring of patients with chronic diseases (hypertension, diabetes mellitus type 2, myocardial infarction, and hypothyroidism) according to national guidelines and additional skills (minor surgery procedures, observation of pregnancy, etc.). FDs fulfilling the criteria are entitled to extra payment. Coverage targets in P4P are universal to all FDs and are increasing stepwise every year according to the negotiations between the Estonian Society of Family Doctors and the Estonian Health Insurance Fund (EHIF). FDs who achieve the agreed targets earn certain points and additional funding accordingly. The maximum number of points FDs can achieve in P4P is 640. A good outcome is defined if an FD achieves more than 480 points (75% of the maximum) in P4P and a poor outcome if an FD has less than 479 points. If an FD achieves less than 479 points, no additional funding is foreseen for the FD.
Every FD in Estonia has their own list of patients, which size and other characteristics could vary, depending on the population density and average population age in the working area (city or rural area). The choice of FD is free for everyone and a person can change FD several times during one calendar year. The maximum number of patients in FDs list is 2,400 persons. FDs with a list of over 2,000 persons need to contract (or employ) another FD, who can work part or full time.
Several researchers have investigated the impact of P4P on quality in primary care.[4-8] Previous studies have investigated the effect of P4P on FD’s workload[4, 5] and on childhood immunisation coverage. [6-8] The introduction of a major national P4P scheme for primary care in the UK was associated with a decrease in emergency admissions and modest cost-effective reductions in mortality and hospital admissions in some domains. [6,7] FDs who achieved a good outcome in P4P have better continuity of care for chronic diseases. This situation also reduced the number of specialist consultations.[6]
The purpose of the study was to find out the impact of payment for performance on the number of family doctors visits, specialist consultations and hospital bed occupancy in Estonia.
Subjects and methods
Study design and period: For this longitudinal study we observed EHIF database data during one calendar year (01.01.2014–31.12.2014). The P4P outcome results for every single FD were collected from the EHIF database, which covers 96 per cent of the Estonian population. The database does not cover the data of those 4 per cent of the population who have no medical insurance. The database was created on the basis of the health service invoices submitted to the EHIF by FDs. These invoices contain detailed records of every physician visit and hospital admission for each patient, and all services provided to the patients (laboratory tests, investigations, counselling, etc.), including all visits to FDs and family nurses, as well as outpatient specialist visits and information about the hospitalisations. The diagnoses of the patients according to the International Classification of Diseases (ICD-10) are provided in these invoices as well. To find out the long-term impact we are planning to continue the study using the same design for a longer study period.
Participants: All working FDs in Estonia (N=803) were divided into two groups according to their outcome in the P4P. For the study we randomly selected 80 FDs (10% of all working FDs): 40 FDs (50%) with a good outcome and 40 FDs (50%) with a poor outcome, proportionally from the cities and rural areas, and from FDs with a median size of the patient in their lists. Patient lists varied from 1,500 to 2,400. We excluded FDs with big and small size lists. To the group of FDs with a good outcome we selected those who achieved more than 600 points and to the group of FDs with a poor outcome those with less than 200 points in the study period (Table 1). We selected FDs with high score and low score, to have more differences between study groups.

Patients with a diagnosis of hypertension and type 2 diabetes (confirmed by FDs according to ICD-10) and who had at least three hypertension or diabetes-related physician visits before the year 2014 were included to the study. There were no age restrictions in the study.
Study size: The number of patients in the study was 49,841. For the study we selected patients who remained with their FD during the whole study period and for that reason we excluded patients (N=1,921) who changed the FDs list (N=1,010) or died (N=911) during the study period.
All patients in the study got a unique ID for studying personal level data and we counted all patient visits to health care providers (HCP): FDs visits, all outpatient specialist visits and days in hospital (bed occupancy) with selected diagnoses (all stages of the hypertension and/or diabetes mellitus type 2) during the period 01.01.2014–31.12.2014 (Table 2).

To understand the impact of comorbidity, we observed different diagnoses (Table 3) and number of different diagnoses per one person in both groups (Figure 1).

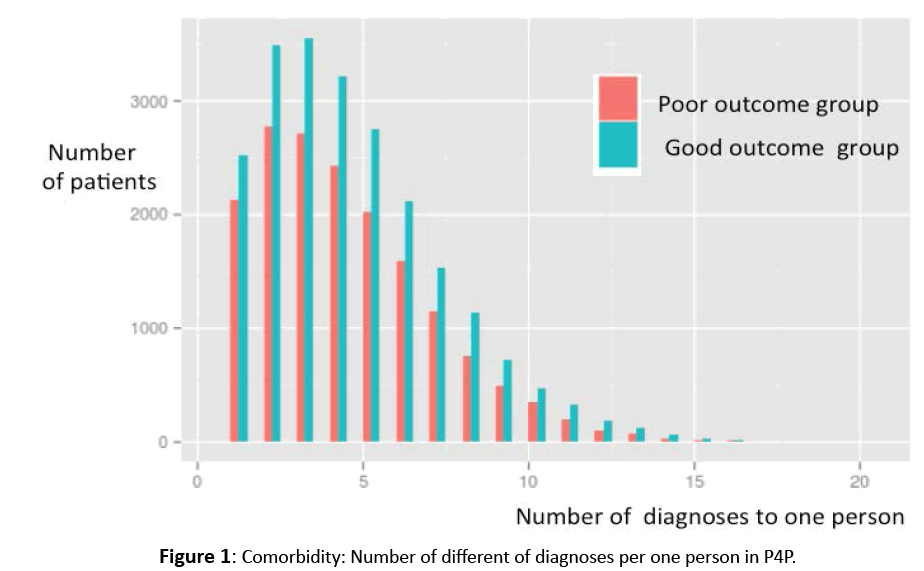
Figure 1: Comorbidity: Number of different of diagnoses per one person in P4P.
Variables: A visit was defined as one contact with an HCP – face to face consultation, telephone advice or e-mail-based consultation. All these types of visits are counted on EHIF invoices with special service codes.
We counted all visits to the FD and all specialist consultations, not only cardiologist or endocrinologist consultations. In addition, all numbers of hospital days during the study period and all reasons for hospitalisations (not only with hypertension or diabetes mellitus type 2) were counted. We selected all patients with all diagnoses of hypertension and/or diabetes mellitus type 2 and calculated their mean number of bed occupancy during the study period. We have not investigated the number of hospitalisations.


Statistical methods: We used descriptive statistics to analyse the data. The differences between the two groups (good outcome and poor outcome) were compared using the non-parametric Mann-Whitney U-test, as the data were not normally distributed; if P was lower than 0.05, the difference was considered statistically significant. Data were analysed using the analysing software IBM SPSS Statistics 19.
Results
We found significant differences in the mean number of FDs visits. FDs with a good outcome provided more visits to patients with all stages of the hypertension (HT) (either I, II, or III) and for patients with diabetes mellitus type 2 (DMT2) compared to poor outcome group.
In the study group of FDs with a good outcome, patients with hypertension stage I had less specialist consultations compared to patients with hypertension stage I in the group of FDs with a poor outcome.
In the study group with a good outcome, all patients with hypertension (including all stages of hypertension: stage I, II and III) had more specialist consultations compared to all patients with hypertension in the group of FDs with a poor outcome.
In the study group with a good outcome, all patients with hypertension and DMT2 had less days in hospital compared to all patients with hypertension and DMT2 in the group of FDs with a poor outcome (Table 2).
The mean number of different diagnoses per one person according the ICD -10 was 4.41 and this was not statistically different in the two study groups (in FDs with a good outcome 4.48 and in FDs with a poor outcome 4.31) (Figure 1).
Discussion
In this longitudinal study we investigated the impact of payment for performance on the number of family doctors visits, specialist consultations and hospital bed occupancy according to two chronic conditions (hypertension and diabetes mellitus type 2).
Several studies have investigated the role of primary care. Easier access to needed services, better quality of care, a greater focus on prevention, and early management of health problems are essential for primary care.6 7 8 The role of P4P is to link financial rewards to quality and performance[9], also to motivate FDs for activities to reduce specialist visits and avoid hospitalisations for chronic patients. Iezzi and authors showed that financial payment might help improve the quality of care and reduce hospitalisations.[10]
In our study, P4P had an impact on the number of visits to FDs and increased it. It is probably because FDs in the P4P system pay more attention to detect chronic diseases in their early stages, actively recall patients for general health checkups and this increases the number of visits, both of the FDs and the nurses.[11] The same was showed by Falzon and authors, that P4P had an effect on workload and work intensification.[12]
One of our earlier studies showed that the implementation of P4P reduced the rate of specialist consultations and hospitalisations[13], but in this study we have found that P4P increased the number of visits also of the specialists. [13] It shows that the effect and the purpose of P4P are not very clear. We expected that with more accurate monitoring of chronic diseases in primary care we can reduce the workload for specialists, but we could not prove it. One reason for this might be due to the short study period, so in our next studies we would like to prolong the study period and find out the long-term impact.

However, if we assume that better quality in primary health care means reduced workload of FDs and specialists, our study shows that simply measuring the performance indicators does not guarantee this.
It is interesting to note that P4P increases the number of specialist consultations. We have not investigated the type of specialist, so one can assume that one reason for more specialist visits could be the difference of the comorbidity of the chronically ill patients, but we did not find a significant difference in the number of different diagnoses per one patient between the two groups of the study.
Another expectation for our study was to find out how P4P affects the hospitalisations. Recent studies showed that P4P reduced the likelihood of diabetes-related hospitalisations for diabetic patients and we have similar findings.[14-16]
In our study, hypertensive patients were in hospital for fewer days. However, it is very difficult to conclude whether the decreased number of days in hospital was due to the P4P.
Despite some optimistic studies[14-20] at the beginning of the introduction of the P4P system into health care, some recent studies have doubts that there is little evidence that P4P programmes in their current form improve health outcomes or healthcare system quality.[15,16]
Our study did not erase the doubts and if we think about the increased workload in P4P, both for FDs and specialists, and only slightly reduced numbers of days in hospital, there is still a need to discuss the possible benefits of P4P.
Conclusion
The P4P in Estonia is a motivation system with financial reward that forces FDs to achieve a good performance outcome. We found that the P4P system in Estonian primary health care increases the number of the visits to FDs as well as specialists. Although hospital bed occupancy was reduced in some circumstances, we could not see the clear effects of P4P for better outcomes for the health care.
Strengths and limitations of the study
• The strength of the study is that we have used data of the whole population and all FDs have been involved in the study and we made random sampling.
• A limitation of this study can be that the data obtained from the registry database can contain some data entry errors.
• Health service invoices that are electronically submitted to the EHIF are governed by specific rules. Previous studies on data quality in the Cancer Registry and Birth Registry have shown that although medical data in the registries are reliable, the descriptions of diagnoses can be erroneous or inadequate. We assumed that any inaccuracies were distributed evenly all over the Estonian population.
• Chronically ill patients are included into FDs’ P4P observation list only if the same patient has the same diagnosis a minimum of three times, to exclude data entry errors and misdiagnosis.
Acknowledgement
Ethical approval
The Ethics Committee of the University of Tartu approved the study.
Authors’ contribution
Eero Merilind has made substantial contributions to the conception, coordination and design of the study, also analysis and interpretation of data, has been involved in drafting the manuscript and revising it critically for important intellectual content, and has given final approval of the version to be published.

Rauno Salupere performed the statistical analysis.
Katrin Västra and Reet Põldsam have made substantial contributions to the acquisition of data.
Ruth Kalda has been involved in drafting the manuscript and revising it critically for important intellectual content, and has given final approval of the version to be published.
References
- Allen T, Mason T, Whittaker W. Impacts of pay for performance on the quality of primary care. Risk ManagHealthc Policy. 2014; 2: 7113– 7120.
- Riigikogu.[Description of work for FDs].RiigiTeataja 2001 Nov 29. Estonian.
- Aaviksoo A. Performance Payment for Family Physicians. Health Policy Monit 2005 Oct6
- Merilind E, Västra K, Salupere R, et al. The impact of pay-for-performance on the workload of family practices in Estonia. Qual Prim Care 2014; 22:109–14.
- Smolkovic L, Kujundžic-Tiljak M, Tiljak H. Trends in General Practitioners/Family Doctors Workload in Croatia in Period 1995–2012. CollAntropol. 23, 2015;3819–3824.
- Starfield B, Shi L, Macinko J. Contribution of Primary Care to Health Systems and Health. Milbank 2005; 83:457–502.
- De Maeseneer J. et al. Primary health care as a strategy for achieving equitable care.Health Systems Knowledge Network of the World Health Organization’s Commission on Social Determinants of Health, 2007.
- Somers AR. And who shall be the gatekeeper? The role of the primary physician in the health care delivery system.Inquiry 1983;301–313.
- Mannion R, Davies HT.Payment for performance in health care.BMJ 2008;336:306.
- Iezzi E, Bruni M, Ugolini C. The role of GP’s compensation schemes in diabetes care: Evidence from panel data. J Health Econ [serial on the Internet]. n.d. [cited November 25, 2015];34104–34120. Available from: Science Citation Index.
- Merilind E, Västra K, Salupere R, et al. The impact of pay-for-performance on the workload of family practices in Estonia. Qual Prim Care 2014; 22:109–114.
- Falzon P, Nascimento A, Gaudart C, Piney C, Dujarier M, Germe J. Performance-based management and quality of work: an empirical assessment. Work (Reading, Mass.) 2015; 41: 13855–3860.
- Kalda R, Västra K. The effect of continuous monitoring of hypertension and type 2 diabetes mellitus on the number of visits to medical specialists and hospitalization: a retrospective study. Medicina 2013; 49:490–96.
- Doran T, Fullwood C, Gravelle H, et al. Pay for performance programs in family practices in the United Kingdom. N Engl J Med 2006;355:375–384.
- Wright M. Pay-for-performance programs Do they improve the quality of primary care?.AustFam Physician
- Scott A, Sivey P, Ait Ouakrim D, et al. The effect of financial incentives on the quality of health care provided by primary care physicians.Cochrane Database Syst Rev 2011

