Man Yee Merl1, Jia Li2, Muhammad Wasif Saif2
1Yale-New Haven Hospital and 2Yale Cancer Center, Yale University School of Medicine.
New Haven, CT, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Yale Cancer Center, Yale University School of Medicine, 333
Cedar Street, FMP 116, New Haven, CT,USA
Phone: +1-203.737.1569
Fax: +1-203.785.3788
E-mail: wasif.saif@yale.edu
Pancreatic cancer is sometimes called a "silent killer" because it is often not diagnosed until it is advanced. It remains the fourth leading cause of cancer-related death in the United States. Gemcitabine has been the front line therapy for advanced pancreatic cancer over the past 10 years. Over this time period, survival benefit has not been able to improve substantially from studies of gemcitabine-based combination therapy. A breakthrough to improve treatment options in this setting is needed. In the 2010 ASCO Gastrointestinal Cancers Symposium in Orlando, Florida, USA, several abstracts were presented to explore new agents or combinations as first-line therapy in locally advanced or metastatic settings. In this article, we review and summarize the findings from these studies
Keywords
gemcitabine; erlotinib; Pancreatic Neoplasms
Abbreviations
HER-1/EGFR: human epidermal growth factor receptor; HER2: human epidermal growth factor receptor 2; IGF- 1R: insulin-like growth factor-1 receptor
INTRODUCTION
During 2009 about 42,470 individuals are diagnosed with pancreatic cancer cases and 35,240 die from the disease in the United States. It is the fourth leading death of cancer among men and women [1]. Unfortunately, the majority of patients present with advanced disease (locally advanced unresectable or metastatic) at the time of diagnosis. The overall survival rate is less than 1% at 5 years with most patients dying within one year [2]. The primary goals of treatment in this setting are improved survival and palliation.
In 1997, Burris et al. reported results of a phase III trial comparing gemcitabine and 5-fluorouracil (5-FU) in untreated patient with advanced pancreatic cancer. Gemcitabine was associated with significantly improvements in median overall survival (5.65 months versus 4.41 months, one-year survival 18% versus 2%) and clinical response (23.8% versus 4.8%, P=0.0022) [3]. The results of this study led to the approval of gemcitabine as first-line therapy of advanced pancreatic cancer. Single-agent gemcitabine has been the standard therapy in advanced pancreatic cancer over the past decade. Subsequently, combinations of gemcitabine with fluorouracil, capecitabine, cisplatin, irinotecan, oxaliplatin, or pemetrexed produced no clear survival benefit [4]. Among the newer approaches, targeting human epidermal growth factor receptor (HER-1/EGFR) shows promise. In a phase III trial, the combination of gemcitabine plus erlotinib showed statistically significant improvements in overall survival compared to gemcitabine alone (median 6.2 months versus 5.9 months, one-year survival 23% versus 17%) [5]. Erlotinib in combination with gemcitabine was approved by FDA for first-line treatment of patients with advanced pancreatic cancer. Although the survival improvement with the combination was statistically significant, it is questionable the two-week improvement in survival is clinically meaningful. Studies for combinations of gemcitabine with cetuximab or bevacizumab, or the combination of bevacizumab with gemcitabine and erlotinib have failed to report an overall survival benefit [4]. A few new front line treatment approaches were presented at the 2010 ASCO Gastrointestinal Cancers Symposium. The findings of these studies are review and discussed.
Updates from the 2010 ASCO Gastrointestinal Cancers Symposium
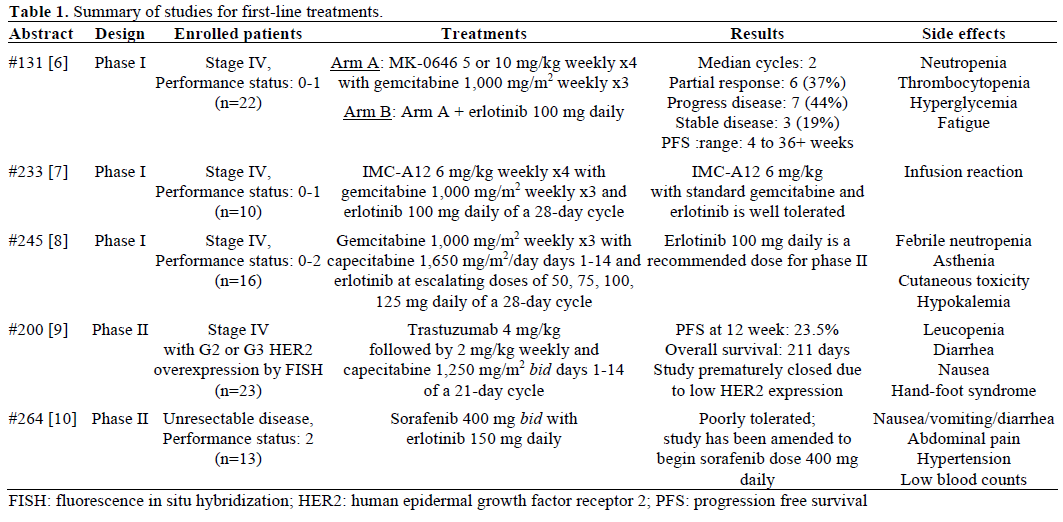
There were three phase I and two phase II studies in previously untreated patients with advanced pancreatic cancer and good performance status. Descriptions of each study are summarized in Table 1.
Phase I Studies
Javle et al. added MK-0646 to standard therapy [6]. MK-0646 is a humanized IgG1 monoclonal antibody that binds to insulin-like growth factor-1 receptor (IGF- 1R). It enhances gemcitabine activities and induces apoptosis through cell signing pathway. Patients received MK-0646 5 or 10 mg/kg and gemcitabine with or without erlotinib. The tolerated dose of MK- 0646 is at 10 mg/kg with gemcitabine and at 5 mg/kg with gemcitabine and erlotinib. Authors also reported encouraging results of 37% partial response and progression free survival range from 4 to 36+ weeks. Hematological toxicities were common. Philip et al. also added a new agent, IMC-A12, to the standard regimen of gemcitabine and erlotinib [7]. IMC-A12 is also a fully human IGF-1R monoclonal antibody that blocks a signaling pathway to enhance tumor cell proliferation and survival. IMC-A12 dose at 6 mg/kg/week was determined as phase II dose. This triple combination was well tolerated. Another phase I trial conducted by Francois et al. was to test the appropriate dose of erlotinib in combination to gemcitabine and capecitabine [8]. The maximum tolerated dose of erlotinib in this triple combination is 100 mg daily. The dose-limiting toxicities are febrile neutropenia and asthenia.
Phase II Studies
Geissler et al. conducted a phase II study using trastuzumab with capecitabine in patient with overexpression of the human epidermal growth factor receptor 2 (HER2) [9]. The study was closed prematurely due to low HER2 over-expression and unfavorable outcome of progression free survival and overall survival. Authors concluded that further investigation of anti-HER2 treatment for advanced pancreatic cancer is not needed. A phase II trial of sorafenib and erlotinib combination conducted by Backlund et al. demonstrated combining these agents with full dose is not safe, and further investigation of the combination with reduced dose of sorafenib is warranted [10].
Discussion
The use of various cytotoxic agents and targeted agents in combination with gemcitabine plus/minus erlotinib has not shown improvement in survival benefit. The addition of novel agents to standard therapy may provide a way to improve the outcome of current therapy. In the phase I studies of MK-0646 and IMCA12 demonstrated encouraging results of their activity in pancreatic cancer and were tolerable [6, 7]. These results indicate that inhibition of IGF-1R signing pathway may play a role in treatment of pancreatic cancer. These novel agents in combination of standard regimen should be further investigated to advance survival benefit. Using HER2 gene amplification to select populations for anti-HER2 therapy is not a good option based on Geisser et al. finding [9]. The results from these studies demonstrated gemcitabine plus/minus erlotinib remain backbone therapy in advanced pancreatic cancer.
Conflict of interest
Authors report no conflict of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, ThunMJ. Cancer Statistics, 2009. CA Cancer J Clin 2009; 59:225-49. [PMID 19474385]
- National Cancer Institute. Pancreatic Cancer Treatment (PDQ®). Accessed 04 Feb 2010.
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, ModianoMR, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J ClinOncol 1997; 15:2403-13. [PMID 9196156]
- Stathis A, Moore MJ. Advanced pancreatic carcinoma: current treatment and future challenges. Nat Rev ClinOncol 2010 Jan 26. [PMID 20101258]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J ClinOncol 2007; 25:1960-6. [PMID 17452677]
- Javle MM, Varadhachary GR, Bhosale P, Ukegbu L, OvermanMJ, ShroffRT, et al. Phase I study of MK-0646, a humanized monoclonal antibody against IGF-1R in combination with gemcitabine or gemcitabine plus erlotinib (E) for advanced previously untreated pancreatic cancer. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 131.
- Philip PA, Goldman BH, RamanathanRK, Lenz, Lowy AM, Whitehead RP, et al. Phase I trial of combination gemcitabine, erlotinib (NSC-718781), and IMC-A12 (NSC-742460) as first-line treatment in patients with metastatic pancreatic cancer: Southwest Oncology Group study S0727. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 233.
- Francois E, Bennouna J, Etienne-Grimaldi M, Follana P, Senellart H, Mari V, et al. Phase I clinical trial with gemcitabine (Gem), capecitabine (Cap), and erlotinib (E) combination in advanced pretreated pancreatic carcinoma. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 245.
- Geissler M, Hofheinz R, Moehler MH, Klöppel G, Bitzer M, BoeckSH, et al. Trastuzumab and capecitabine in patients with HER2-expressing metastatic pancreatic cancer: A multicenter phase II study of the AIO pancreatic cancer group (on behalf of the German AIO group [AIOPK-0204]). 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 200.
- Backlund DC, Goff LW, Chan E, Shyr Y, Conkright WA, Cornelius LA,et al. A phase II trial of sorafenib (S) and erlotinib (E) in unresectable pancreas cancer: Preliminary results. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 264.

