Keywords
Effectiveness; Structured teaching program; Prevention; Depression; Elderly.
Abbreviations
df : Degrees of freedom
% : Percentage
S.D. : Standard deviation
f : Frequency
N : Number of subjects
NS : Non-significant
Introduction
Aging is a progressive state, beginning with conception and ending with death, which is associated with physical, social and psychological changes. The aging process is a biological reality that has its own dynamic, largely beyond human control. Depression among the elderly is relatively common; however, it is not often recognized and even when it is recognized it is often left untreated. Two inaccurate assumptions are commonly held; that, depression is inevitable in old age and therefore not worth treating, and that depression is a prodromal phase of dementia and therefore untreatable [1]. Epidemiological studies regarding depression in old age have shown that, on average, approximately 10% of individuals over 65 yrs old have clinical symptoms of depression. Estimates of major depression levels in elderly individuals living in the community range from less than 1% to 5%, but rise to 13.5% in those who require home care. Almost 50% of the world’s elderly live in Asia, of which 23% live in India [1]; therefore, health policy makers need to recognize this changing demographic pattern and plan for the prevention and control of diseases associated with old age.
Old age is often portrayed as a time of rest, reflection, and opportunities to do things that were delayed while raising families and pursuing careers [2]. Old age is a crucial phase during which physiological, psychological, and socio-cultural changes contribute to depression and anxiety. Late-life events including chronic and debilitating medical disorders, failing eyesight, hearing loss, and other physical changes, in addition to external pressures such as limited financial resources, often give rise to negative emotions such as sadness, anxiety, loneliness, and lowered self-esteem, which in turn lead to social withdrawal and apathy [2]. The prevalence of late-life depression in many population surveys does not appear to be due to the misattribution of depressive symptoms to physical disorders. Although it has been well established that dementia leads to depression, there is now increasing evidence that depression leads to cognitive decline and dementia [3].
Depression causes significant suffering and is commonly seen in primary care [4]. Since primary care providers sometimes fail to identify patients as depressed, systematic screening programs may be of use for improving outcomes in depressed patients. It is predicated that the identification of depression via screening programs will allow effective delivery of treatment, and that the benefits of treatment will outweigh the harm. Mental health disorders, including anxiety and depression, adversely affect physical health and the ability to function, especially in the elderly [5]. The World Health Organization projects that by the yr 2020, depression will remain a leading cause of disability, second only to cardiovascular disease [6]. Assessment of depression in homebound elderly individuals is crucial since depression affects quality of life, mortality, and health care costs.
The prevalence of depression in homebound elderly individuals is estimated to range from 26% to 44% [7] and is the most common psychiatric disorder in the elderly, who constitute 12.7% of the general population of the United States [8]. The aging individual’s adaptive coping strategies may be seriously challenged by major stressors, such as financial problems, physical illness, and changes in body functioning, and increasing awareness of approaching death. This treatable disorder currently robs millions of elderly Americans of the enjoyment of normal pursuits of late-life [9]. In addition, the rate of suicide is highest, and growing, in individuals aged 65 yrs or older, for whom suicide ranks as the 13th most common cause of death. It is estimated that the number of elderly individuals with mental illness will increase to 15 million by 2030; which was only 4 million in 1970 [10]. The Indian elderly population is currently the second largest in the world, and communitybased mental health studies have revealed that the prevalence of depressive disorders varies from 13% and 25% [10].
Roy’s adaptation model, based on general system theory, was applied to the present study (Figure 1). The focus of Roy’s model is a set of processes through which elderly individuals adapt to the environmental stimuli of depression. Each elderly individual is a unified biopsychosocial being in constant interaction with a changing external environment; when the demands of environmental stimuli are too great or the knowledge in elderly regarding the prevention of depression is too low, their responses are ineffective. This model views the individual as an adaptive system that functions as a whole through the interdependence of all its parts. The system consists of input, throughput (process, effectors), output, and feedback [11].
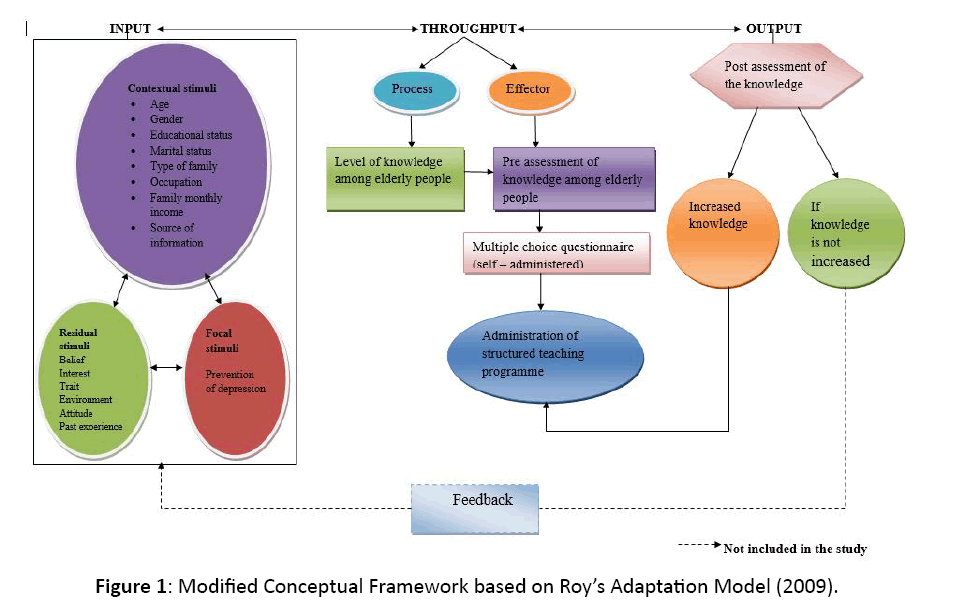
Figure 1: Modified Conceptual Framework based on Roy’s Adaptation Model (2009).
The purpose of the present study was to assess the effectiveness of a structured teaching program on knowledge regarding the prevention of depression among the elderly, with a view to ensuring that adequate education can be given to promote mental health and to prevent mental illness. In the present study we assessed and compared the pre- and post-test knowledge of elderly individuals regarding the prevention of depression. Moreover, we investigated the relationship between knowledge and selected demographic variables such as age, gender, educational status, marital status, family type, occupation, monthly family income, and source of information.
Methods
A quasi-experimental research approach was adopted to assess the effectiveness of a structured teaching program on knowledge regarding the prevention of depression among the elderly in the selected village of Moga, Punjab, India. This approach involved manipulation but lacked a control group.
Sample and sampling technique
A village known as Darapur in Moga was selected using a simple random sampling technique (Lottery method); [12], and the investigator carried out a survey of the village, producing a sampling frame of 180 elderly individuals. Subsequently, the investigator selected a sample of 60 elderly individuals by the systematic random sampling technique using the formula; K=number of subjects in target population/size of sample i.e. 180/60=3 [13]. Thus, every third individual in the list was selected as a sample for the study.
Description of the tool
A self-structured multiple-choice questionnaire was prepared to assess the knowledge regarding the prevention of depression in the elderly. The final tool consisted of the following parts:
Part I-Self-structured questionnaire related to sample characteristics
This part consisted of items with which to obtain personal information regarding the subjects, such as: age, gender, educational status, marital status, family type, occupation, monthly family income and source of information.
Part II-Self-structured questionnaire related to knowledge in the elderly
This part consisted of multiple-choice questions regarding the prevention of depression. A total of 30 questions were included, with each right answer carrying one mark and each incorrect answer carrying 0 marks. Thus, the maximum score was 30 and the minimum score was 0.
Data collection procedure
Data collection was performed during February 2012. The questionnaire was translated into the Punjabi language for the subject’s convenience. Prior to administering the questionnaire, the investigator gave instructions to the elderly individuals and explained the purpose of gathering the information. They were assured that their responses would be kept confidential and used for research purposes only. The sample consisted of 60 elderly individuals. At the beginning, the personal information of all the elderly individuals was taken and a pre-test was given to assess their knowledge regarding the prevention of depression.
A structured teaching program was provided to the group by the investigator, with the help of audiovisual aids, following the administration of the pre-test regarding the prevention of depression. The time spent on the structured teaching program was 45 min. Prior to the teaching program, a good rapport was established with the elderly individuals, and the necessary arrangements were made to effectively convey the material. At the end of the program, any questions were answered and any misunderstandings were clarified. A post-test was subsequently administered to the elderly individuals after a gap of two days of information retention.
Data analysis
Analysis of the data was conducted in accordance with the objectives. The SPSS statistics software version 11.1 was used to provide descriptive statistics including the range, mean, and standard deviation, paired and unpaired t-tests, F-test, ANOVA, inferential statistics, and correlation coefficients.
Results
The data collected through the self-structured multiplechoice questionnaire regarding knowledge in the elderly were analyzed using descriptive and inferential statistics. In descriptive statistics, the mean, percentage and standard deviation were used to analyze the distribution of the elderly individuals according to their demographic characteristics. In inferential statistics, SPSS version 11.1 was used to perform a paired t-test and F-test. The data analysis was based on the study objectives and included: a) a description of the samples’ demographic characteristics; b) an assessment of knowledge in elderly individuals regarding the prevention of depression; and c) the relationship between knowledge and selected demographic variables such as age, gender, educational status, marital status, family type, occupation, monthly family income and source of information.
Sample characteristics
The elderly individuals were distributed into various categories according to age, gender, educational status, marital status, family type, occupation, monthly family income in Rupees, and source of information (Table 1), it shows that the majority of elderly individuals were in the 60–64 yrs old (46.7%) age group, and the least were 70 years old and above (20%); 50% were male and 50% were female; the majority were illiterate (30%) and the least were educated to a graduate level or above (10%); the majority were married (56.7%); and the least were divorced (3.3%); the majority belonged to a joint family (48%) and the least belonged to an extended family (23%); the majority were housewives (37%) and the least had a private job (12%); the majority belonged to the 15,001 Rs/mon and above income group (33.3%) and the least belonged to the less than or equal to 5,000 Rs/mon group (15%); and the majority obtained information from mass media (38.3%) and the least from friends (20%) and health professionals (20%).
| N=60 |
| CHARACTERISTIC S |
N |
% |
| 1. Age |
| 60–64 years old |
28 |
46.7 |
| 65–69 yrs old |
20 |
33.3 |
| 70 yrs and above |
12 |
20 |
| 2. Gender |
| Male |
30 |
50 |
| Female |
30 |
50 |
| 3. Educational Status |
| Illiterate |
18 |
30 |
| Primary |
14 |
23 |
| Matric |
14 |
23 |
| Secondary |
8 |
14 |
| Graduate and above |
6 |
10 |
| 4. Marital Status |
| Single |
9 |
15 |
| Married |
34 |
56.7 |
| Widow |
9 |
15 |
| Widower |
6 |
10 |
| Divorced |
2 |
3.3 |
| 5. Family Type |
| Nuclear |
17 |
29 |
| Joint |
29 |
48 |
| Extended |
14 |
23 |
| 6. Occupation |
| Retired |
10 |
16 |
| Private job |
7 |
12 |
| Housewife |
22 |
37 |
| Labourer |
9 |
15 |
| Farmer |
12 |
20 |
| 7. Monthly Family Income In Rs |
| ≤ 5,000 |
9 |
15 |
| 5,001–10,000 |
15 |
25 |
| 10,001–15,000 |
16 |
26.7 |
| 15,001 and above |
20 |
33.3 |
| 8. Source of Information |
| Relatives |
12 |
20 |
| Friends |
13 |
21.7 |
| Mass media |
23 |
38.3 |
| Health Professionals |
12 |
20 |
Table 1: Percentage distribution of the sample characteristics.
Assessment and comparison between the pre-and posttest knowledge data
In the pre-test, the majority of elderly individuals (45%) obtained an average knowledge score, 30% obtained a below average knowledge score, and 25% obtained a good knowledge score; while in the post-test, the majority of elderly individuals (80%) obtained a good knowledge score and 20% obtained an average knowledge score (Table 2). Thus, it can be concluded that most of the elderly individuals obtained an average knowledge score in the pre-test and a good knowledge score in the post-test, indicating that the structured teaching program was effective in helping the elderly individuals to increase their knowledge regarding the prevention of depression. The mean pre-test knowledge score was 17.25 and the mean post-test knowledge score was 23.42.
| N=60 |
| Knowledge Score |
| Level of Knowledge |
Score |
Pre-test |
Post-test |
| N |
% |
N |
% |
| Good |
23-30 |
15 |
25 |
48 |
80 |
| Average |
16-22 |
27 |
45 |
12 |
20 |
| Below average |
≤15 |
18 |
30 |
- |
- |
Table 2: Frequency and percentage distribution of pre- and post-test knowledge scores among elderly individuals regarding the prevention of depression according to the level of knowledge.
The difference between the mean pre- and post-test knowledge scores was highly significant (p<0.001; Table 3). Therefore, the null hypothesis H0 (the mean post-test knowledge score after a structured teaching program in elderly individuals regarding the prevention of depression will be insignificant (p<0.05)) is rejected and the research hypothesis H1 (the mean post-test knowledge score in elderly individuals will be significantly higher than the pre-test mean (p<0.05) after a structured teaching program in the elderly regarding the prevention of depression) was accepted. This reveals that the structured teaching program had an impact on knowledge in elderly individuals regarding the prevention of depression.
| Knowledge Score |
| |
N |
Pre-test |
Post-test |
df |
t |
| Mean |
S.D |
Mean |
S.D |
| Knowledge Score |
60 |
17.25 |
3.88 |
23.42 |
2.77 |
59 |
22.82*** |
Maximum Score=30
Minimum Score=0
NS–Non-significant; *Significant; p<0.05; ***Significant; p<0.001 |
Table 3: Comparison of the mean pre- and post-test knowledge scores in elderly individuals regarding the prevention of depression.
Relationship between knowledge and selected demographic variables
The mean pre-test knowledge score in elderly individuals belonging to 60–64 yrs old age group was the highest (18.79), followed by that in the 65–69 yrs old (17) and the 70 yrs old and above (14.08) age groups, showing statistical significance (p<0.001 in an F-test) (Table 4). The mean post-test knowledge score in the elderly individuals belonging to 60–64 yr old age group was the highest (24.61), followed by that in the 65–69 yrs old (23.25) and 70 yrs old and above (20.92) age groups, showing statistical significance (p<0.001 in an F-test; Table 4). The mean difference between pre and post-test knowledge scores in elderly individuals was compared and shown to be highly significant (p<0.001). Therefore, age had some impact on knowledge and the structured teaching program had a definite effect on increasing the knowledge in elderly individuals regarding the prevention of depression.
| Knowledge Score |
| Age |
N |
Pre-test |
Post- test |
df |
t |
| Mean |
S.D |
Mean |
S.D |
| 60-64 yrs old |
28 |
18.79 |
3.50 |
24.61 |
1.87 |
27 |
7.77*** |
| 65-69 yrs old |
20 |
17 |
4.00 |
23.25 |
2.90 |
19 |
5.68*** |
| 70 yrs and above |
12 |
14.07 |
2.46 |
20.92 |
2.74 |
11 |
6.45*** |
| |
df |
F |
P |
F |
P |
| Variance within the group |
57 |
7.62*** |
0.001 |
9.73*** |
0.000 |
| Between the groups |
2 |
- |
- |
- |
- |
Maximum Score=30
NS–Non-significant; *Significant; p<0.05; ***Significant; p<0.001 |
Table 4: Comparison of the mean pre-test and post-test knowledge scores regarding the prevention of depression among elderly individuals, according to age.
The mean pre-test knowledge score in females was higher (17.37) than in males (17.13); however, the difference was not statistically significant (p<0.05 in an F-test; Table 5). The mean post-test knowledge in females was higher (23.43) than in males (23.40) however, the difference was not statistically significant (p<0.05 in an F-test; Table 5). The mean difference between pre- and post-test knowledge scores in elderly individuals were compared and shown to be highly significant (p<0.001). Hence, it can be concluded that gender had no impact on knowledge, but the structured teaching program had a definite impact on increasing knowledge in elderly individuals regarding the prevention of depression.
| Knowledge Score |
| Gender |
N |
Pre-test |
Post- test |
df |
t |
| Mean |
S.D |
Mean |
S.D |
| 60-64 yrs old |
28 |
18.79 |
3.50 |
24.61 |
1.87 |
27 |
7.77*** |
| 65-69 yrs old |
20 |
17 |
4.00 |
23.25 |
2.90 |
19 |
5.68*** |
| 70 yrs and above |
12 |
14.07 |
2.46 |
20.92 |
2.74 |
11 |
6.45*** |
| |
df |
F |
P |
F |
P |
| Variance within the group |
57 |
7.62*** |
0.001 |
9.73*** |
0.000 |
| Between the groups |
2 |
- |
- |
- |
- |
Maximum Score=30
Minimum Score=0
NS–Non-significant; *Significant; p<0.05; ***Significant; p<0.001 |
Table 5: Comparison of the mean pre- and post-test knowledge scores regarding the prevention of depression among elderly individuals, according to gender.
The mean pre-test knowledge score in elderly individuals educated to graduate and above level was the highest (23.00), followed by those educated to secondary level (22.13), matric (18.50), and primary (15.93), with the lowest being in the illiterate (13.22). The mean post-test knowledge score in elderly individuals educated to graduate and above level was the highest (26.50), followed by those educated to secondary level (26.45), matric (24.29), and primary (23.07), with the lowest being in the illiterate (20.61). Both mean the pre- and post-test knowledge score were statistically significant (p<0.001 in an F-test). The difference between the mean pre- and post-test knowledge scores in elderly individuals was highly significant (p<0.001; Appendix I).
Divorced elderly individuals showed the highest (21.00) mean pre-test knowledge score, followed by those who were married (18.29), widowers (16.83), widows (15.11), and single (14.89). The mean post-test knowledge score in divorced elderly individuals was the highest (24.50), followed by those who were married (24.21), widowers (23.17), widows (22), and single (21.78). Both the mean pre- and post-test knowledge scores were statistically significant (p<0.05 and p<0.001, respectively; Appendix II). Therefore, it can be concluded that marital status had some impact on knowledge, but the structured teaching program had a definite effect on increasing knowledge in elderly individuals regarding the prevention of depression.
Similarly, the pre- and post-test knowledge scores and p-values related to employment and income statuses in elderly individuals are given in Appendices III and IV.
Discussion
The present study was conducted in Darapur, Moga, Punjab, India. A systematic random sampling technique was used to collect the sample of 60 elderly individuals. Prior to data collection, the investigators gave a brief introduction about themselves, the purpose of the study, and instructions regarding the filling of the questionnaire to put the elderly individuals at ease. In the present study 46.7% of the elderly individuals belonged to the 60–64 yrs old age group; 50% were female and 50% were male; 30% were illiterate; 56.7% were married and 33.3% had a monthly family income of 15,001 or above. These findings are consistent with a previous report in which 52.6% belonged to the 60–69 yrs age group and 36.0% were male and 64.0% were female [14]. In the present study, 40% of the elderly individuals were illiterate, the majority (61.2%) belonged to the 15,000–25,000 Rs/mon income group; and 56.3% were married. Moreover, in the present study 16.7% of the elderly individuals were retired and 28.3% lived in nuclear family, which is in accordance with previous reports in which 22.4% of elderly individuals were retired and 38% lived in nuclear families [15].
The first objective of the present study was to assess the pretest knowledge in elderly individuals regarding the prevention of depression. The majority of elderly individuals (45%) obtained an average pre-test knowledge score, 30% obtained a below average knowledge score, and 25% obtained a good knowledge score. These findings are similar to those reported by Wang, 2009, in which 35% of elderly individuals obtained a good pretest knowledge score. According to the second objective of the present study, 80% of elderly individuals obtained a good posttest knowledge score and 20% obtained an average knowledge score. Similar findings have been reported previously, in which 75% of elderly individuals obtained a good post-test knowledge score [16,17].
In the present study, the difference between the mean preand post-test knowledge scores was highly significant (p<0.001). These findings are supported by a prior study in which a highly significant difference between the mean pre- and post-test scores was found (24.45 ± 2.21 and 29.18 ± 4.00; p<0.001) [18].
The third objective of the present study was to investigate the relationship between knowledge and selected demographic variables such as age, gender, educational status, marital status, family type, occupation, monthly family income, and source of information. There was a statistically significant effect of all variables on the knowledge score, with the exception of gender and family type. This finding is supported by an earlier study showing that age, literacy level, occupation, marital status, monthly family income, and source of information had a significant impact on the knowledge in elderly individuals (p<0.05) [19].
The present study shows that age had no impact on the knowledge in elderly individuals regarding the prevention of depression, which is consistent with previous studies (p<0.001) [20,21]. Similarly, gender and family type had no impact on knowledge in elderly individuals regarding the prevention of depression in either the present or in a previous study [22].
Conclusion
The results of the present study suggest that the knowledge in the majority of elderly individuals regarding the prevention of depression was average prior to taking part in the structured teaching program; however, knowledge increased by 2-fold afterward. The difference between the mean pre- and post-test knowledge scores was highly significant (p<0.001); therefore, the null hypothesis H0 was rejected and the research hypothesis H1 was accepted; that a structured teaching program had a significant impact on the knowledge in elderly individuals regarding the prevention of depression. Our findings reveal that there is a need for extensive research regarding the prevention of depression among the elderly, such that these individuals can be given the necessary awareness to prevent depression, presenting an avenue for innovative methods of prevention of depression. However, there is a need for ongoing research in psychiatric and mental health nursing, such that the decision makers become more aware of the latest issues, and therefore, identify problems in the elderly sooner, reducing the mortality rate.
Based on the present findings, we make the following recommendations:
1. The study should be repeated in a larger population to validate and generalize our recent findings.
2. The investigation should be conducted as a longitudinal study.
3. A comparative study should be conducted to assess the knowledge of elderly people regarding the prevention of depression in urban and rural areas.
4. A similar study should be carried out using other teaching strategies i.e. self-instruction or computerassisted instructions.
5. A similar study may be conducted that includes other mental health problems of the elderly such as mania and schizophrenia.
Declarations
Ethics approval and consent were obtained.
Ethical Considerations
The present study was carried out following ethical approval from the Ethical Review Committee of the University.
Acknowledgments
The authors wish to thank the Baba Farid University of Health Sciences faculty and staff for their assistance during the course of the present study. We thank Dr. Amarjit Kaur Singhera for her advice in preparing the original thesis, from which this manuscript is taken, and Mr. Ravinder Soni for his help in conducting the statistical analysis. We would also like to thank Dr. Ali Mallakin for his critical review and Dr. Natalie Anne Ward for editing this manuscript.
Availability of Data and Materials
The data analyzed during the present study are available from the corresponding author on reasonable request.
Declaration of Conflict of Interest
The authors declare no conflicts of interest. The authors alone are responsible for the content and writing of the present article.
Author Contributions
Data collection, study design, and drafting of the manuscript: RK; Acquisition of data: RS; Statistical analysis: RK; Critical review and revision of the manuscript: RK, AM, and NAW. RK performed the study and interpreted the data.
Consent for Publication
All authors have reviewed and consented to publication of the paper.
References
- Reddemma K. Depression in elderly individuals suffering with neurological disorders. Indian J Psychiatry Nurs 2012; 3: 38-39.
- Silk S. Depression and elderly. J American psychol 2010; 11: 193-197.
- Byrne GJ, Pachana NA. Anxiety and depression in the elderly: Do we know any more?. Curr Opin Psychiatry 2010; 6: 504-509.
- Connor EA, Whitlock EP, Gaynes B, Beil TL. Screening for depression in adults and older adults in primary care. Agency for health care research and quality 2009.
- Hughes F. Addressing mental health needs of older adults. J Psychol Aging 2009; 35-38.
- Doherty AM, Gaughran F. Psychology and Aging. Interface between physical and mental health care. Soc Psychiatry Psychiatr Epidemiol 2014; 673-682.
- Loughlin A. Depression and social support. J Gerontol Nurs 2004; 30: 24-27.
- Townsend MC. Psychiatric Mental Health Nursing. FA Davis publications 489, 727.
- Zubenko GS, Mulsant BH, Rifai AH, Sweet RA, Pasternak RE, et al. Impact of acute psychiatric inpatient Treatment on major depression in late life. American journal of psychiatry. Am J Psychiatry 1994; 151: 987-994.
- Barua A, Kar N. Screening for depression in elderly Indian population. Indian J Psychiatry 2010; 52:150-153.
- Roy C. The Roy adaptation model (3rd ed.). Hall Health. 2009.
- Burns N, Grove SK. The practice of nursing research. Conduct, critique and utilization; 5th edition. Philadelphia: WB Saunders. 2011.
- Clarke A. Qualitative research: Data analysis techniques. Prof Nurse 1999; 14: 531-533.
- Barua A. Screening for depression in Indian elderly population. Indian J Psychiatry 2010; 52: 150-153.
- Sharif F. Prevalence of depression among elderly people. J of gerontol 2008; 12 : 17-19.
- Wong JJ. Education support groups in changing caregiver’s psychological elder abuse behavior towards caring for elders. Adv Health Sci Educ 2009; 14: 377-386.
- Minardi HA, Blanchard M. Older people with depression: pilot study. Issues and innovations in nursing practice. J Adv Nurs 2004; 46: 23-32.
- Clark MJ. The effects of group reminiscence therapy on depression, self-esteem, and life satisfaction of elderly nursing home residents. J Nurs Res 2006; 14: 36-44.
- Sharif F. Prevalence of depression among elderly people. J Gerontol 2008; 17-19.
- Mantyselka P, Hartikainen S, Louhivuori LKA, Sulkava RO. Effects of dementia on perceived daily pain in home-dwelling elderly people. Age Ageing 2004; 33: 496-499.
- Beyer JL. Managing depression in geriatric populations. Ann Clin Psychiatry 2007; 19: 221-238.
- Ahmed I. Depression in the elderly: Does family system play a role? A cross-sectional study. BMC J Psychiatry 2007; 12: 7-10.

