Keywords
Exocrine Pancreatic Insufficiency; Randomized Controlled Trials as Topic; Therapeutics
Abbreviations
FACT: Functional Assessment of Cancer Therapy; CGIDS: clinical global impression of disease symptoms; MedDRA: Medical Dictionary for Regulatory Activities
INTRODUCTION
In clinical routine a substantial number of patients suffering from acute pancreatitis experience abdominal symptoms when refeeding starts. Some of them suffer from pain, others experience flatulence or diarrhea and the intensity of these symptoms varies widely. Significant pancreatic exocrine insufficiency at the time point when refeeding starts could be one explanation of these symptoms. Data regarding exocrine pancreatic function in the early recovery phase from acute pancreatitis are rare and conflicting, ranging from abnormal values for 3 months to 4 years after acute pancreatitis [1, 2, 3, 4, 5, 6, 7]. The severity of pancreatic exocrine insufficiency is directly related to the severity of the disease: Patients with more extended necrosis have a more severe pancreatic exocrine insufficiency [1, 3, 4, 8, 9]. Interestingly, even in patients with mild, edematous acute pancreatitis, exocrine pancreatic function is impaired in the early course after acute attack but exocrine function recovers in the majority of these patients [3]. On the other hand, patients with necrotizing acute pancreatitis have persisting pancreatic exocrine insufficiency on long term follow up [2, 8]. However, there are data that functional impairement even after acute necrotizing pancreatitis is transient and recovers within a few years [10]. Different enzyme systems contributing to exocrine pancreatic function can be impaired, and undergo recovery, at different levels with persisting pancreatic lipase deficiency causing the most symptoms [2].
The influence of the underlying etiology on the development of pancreatic exocrine insufficiency is unclear. There are data indicating that patients with alcoholic acute pancreatitis have a more severe impairment of exocrine pancreatic function which also persists longer [1]. Whether this is related to preexisting chronic damage of the pancreas remains unclear, but seems probable.
Whether pancreatic enzyme supplementation has a beneficial effect on resolution of symptoms and the recovery after acute pancreatitis should be further investigated.
One randomized, placebo controlled study investigated the effect of pancreatic enzyme supplementation on pain, analgesic requirements and complications in an early phase of acute pancreatitis and could not show any beneficial effect [11].
Another clincical trial included 59 subjects with mild acute pancreatitis. It was shown that after five days of refeeding with additional pancreatic enzyme supplementation a significant improvement in exocrine pancreatic function occurred. After six weeks of treatment this difference finally disappeared [12].
Due to a lack of available data, a beneficial effect of pancreatic enzyme supplementation in patients with pancreatic exocrine insufficiency and during the refeeding phase after acute pancreatitis has not been established.
The objective for this study was to evaluate if pancreatic enzyme replacement therapy improves the recovery of exocrine pancreatic function (measured by fecal elastase) in subjects during refeeding after moderate to severe acute pancreatitis compared with placebo, as well as to explore the efficacy, safety and tolerability of enzyme replacement treatment in these patients.
PATIENTS AND METHODS
Design
A prospective double-blind, placebo controlled, randomized, parallel group study was conducted in three centers in Germany.
Selection of Patients
As no information about fecal elastase 1 levels was available in the literature, the sample size calculation was done by means of simulation techniques. One-thousand studies with two balanced arms were simulated, presuming that there were 0% responders at baseline and 100% responders at the end of treatment in both groups. Subjects were allowed to drop-out during the simulation, which leads to right-censoring of the measures. A mean of 8.9% censored values over the 1,000 studies was obtained. It was assumed that the number of responders follows a linear trend over time under placebo and that the responder rate under pancreatic enzyme supplementation is three times the one under placebo after three days of treatment and twice the one under placebo at each following assessment. Under these assumptions, a power of 92% was obtained at an alpha level of 5% if 40 subjects were included per arm. To compensate for the expected screen failures at baseline (30%), a total of 114 subjects was considered to be appropriate for this study.
Men and women, at least 18 years of age, were eligible for this study if they gave their informed consent and suffered from moderate to severe acute pancreatitis (defined as patients with C-reactive protein (CRP) greater than 120 mg/L and APACHE II score greater than 4). Patients with known chronic pancreatitis, pre-existing exocrine pancreatic insufficiency, earlier gastric or pancreatic resection, small bowel disease or known gastroparesis were excluded from the study.
The study was terminated with 56 patients randomized for treatment due to insufficient recruitment. Details regarding patient population are given in Table 1. One patient was excluded from the efficacy evaluation due to very early study termination on Day 3, with no data obtained for any analysis. Study termination in this subject was due to an adverse event, not related to study medication.

Study Medication
According to the double-blind parallel-group study design, subjects were individually randomized to receive either pancreatic enzyme supplementation (Creon® 25,000 Minimicrospheres (mms) capsules; Abbott Laboratories GmbH (previously Solvay Pharmaceuticals GmbH), Hannover, Germany; lipase 25,000 European Pharmacopoeia (Ph. Eur.) Units; amylase 18,000 Ph. Eur. Units, protease 1,000 Ph. Eur. Units) orally or matching placebo capsules during a treatment period of 26-30 days. Two capsules were taken per main meal (three main meals a day) and one capsule per snack (one to three snacks a day).
Study Design
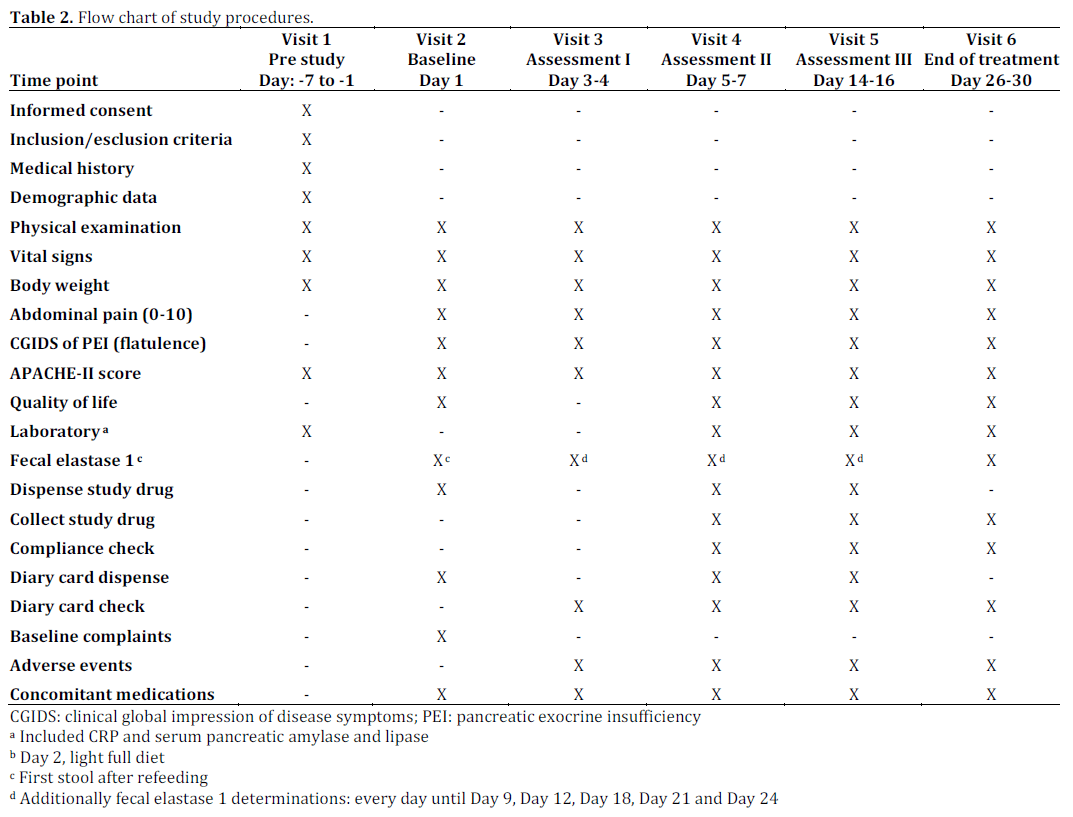
Patients were initially (after the acute phase of the pancreatitis) treated on an in-patient basis, and during follow up, as outpatients (Figure 1, Table 2).
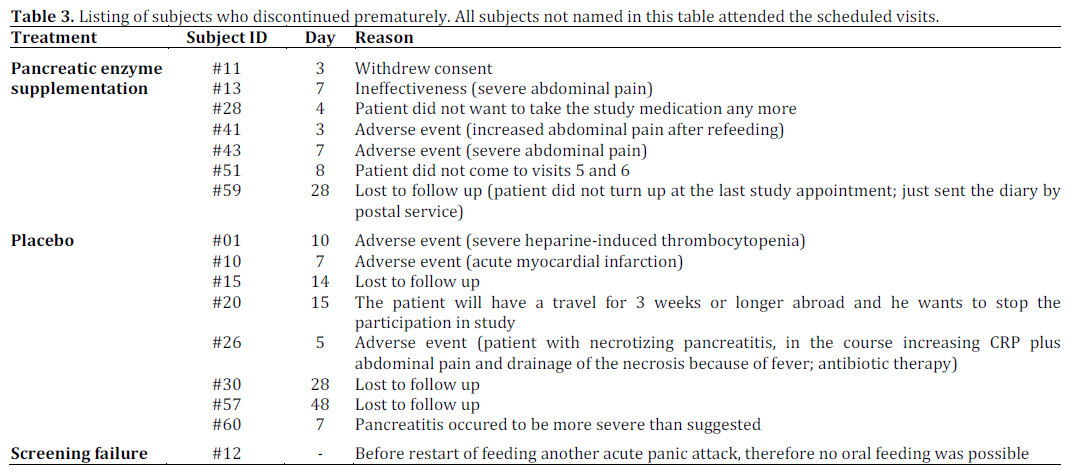
For evaluation purposes patients were divided into two separate samples. The first sample contained all patients randomized with at least one set of efficacy data available (total study population-sample; n=55) and a second data set was generated using all subjects with a fecal elastase level at baseline less than 200 μg/g stool (analysis sample; n=20). The listing of subjects who discontinued prematurely is shown in Table 3.
Primary Objective
The primary objective was the evaluation of the recovery from pancreatic exocrine insufficiency in subjects during the refeeding phase after moderate to severe acute pancreatitis.
The main variable was the time to response, which was defined as the interval of time between the baseline assessment and the first visit where a human fecal elastase level above the response level was measured. A subject was considered to have recovered from pancreatic exocrine insufficiency if the level of human fecal elastase reached the threshold of 200 μg/g stool. The analysis of the primary variable was therefore performed in the analysis sample only.
Absolute Values of Fecal Elastase
Enzyme elastase 1 was determined in the first stool after start of refeeding, and thereafter every day until and including Day 9 and at all following visits. Further measurements were performed at Days 12, 18, 21 and 24. Elastase 1 was determined with the ScheBo-Tech test kit (Enzyme-Linked Immunosorbent Assay (ELISA)-Test with elastase 1 antibodies) [13, 14].
Secondary Objectives
The secondary objective was to evaluate the effect of pancreatic enzyme replacement on body weight, abdominal pain, patient symptoms, Acute Physiology and Chronic Health Evaluation (APACHE) II score, quality of life (QoL), as well as Creactive protein and serum pancreatic amylase and lipase. The analysis of the secondary variables was performed both for the total study populationsample and for the analysis sample.
Body Weight
Body weight was measured in light clothing without shoes at each study visit.
Abdominal Pain
For simplicity, abdominal pain was measured using a 11-point interval scale ranging from 0 (“no pain”) to 10 (“worst pain imaginable”) instead of a visual analogue scale (VAS) made by a continuous horizontal line.
Clinical Global Impression of Disease Symptoms (CGIDS)
CGIDS (flatulence) of pancreatic exocrine insufficiencywas rated by the investigator and subject as follows:
0: none (symptoms not present);
1: mild (symptoms present but not bothersome);
2: moderate (symptoms bothersome);
3: severe (symptoms interfere with normal activities);
4: incapacitating (symptoms prevent subject from continuing normal activities).
APACHE II score
APACHE II score was calculated as described elsewhere [15].
Quality of life (QoL)
Version 4 of the validated QoL questionnaire Functional Assessment of Cancer Therapy (FACT)- Pa (www.facit.org) was used to assess QoL [16, 17]. This questionnaire includes a total of 36 items (statements) covering physical, functional, social and emotional well-being, and specific items related to the underlying disease (additional concerns). The questionnaire (FACT-Pa) used in our trial was replaced by the holder of the copyright. The only available questionnaire evaluated for pancreatic diseases is now FACT-Hep. The validity of this questionnaire was published in 2012 by Cella et al. [18].
Summary scores were calculated for each subscale and the total questionnaire. A higher score generally reflects a higher QoL. The minimum possible value is zero for all summary scores. The maximum possible value is 24 for emotional wellbeing, 36 for additional concerns, 28 for all other subscales, and 144 for the total questionnaire.
C-Reactive Protein, Serum Pancreatic Amylase and Lipase
Enzymes were determined with standard laboratory biochemical methods by the local laboratories.
ETHICS
The study protocol was reviewed and approved by the ethical committees of the three participating centers. Written informed consent was obtained from each patient. The study protocol conforms to the ethical guidelines of the “World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008.
STATISTICS
Discrete data are reported as frequencies, while mean ± standard deviation or median and range (minimum and maximum) have been used to show scale variables.
Kaplan-Meier estimates of the proportion of subjects with recovery from pancreatic exocrine insufficiency (primary variable) were done and treatment groups (pancreatic enzyme supplementation vs. placebo) were compared by using a log-rank test.
Age and fecal elastase-1 levels at baseline were compared by means of ANOVA while ANCOVAs were applied to human fecal elastase 1 as well as the secondary efficacy variables: body weight, APACHE II score, QoL, CRP, as well as serum pancreatic amylase and lipase for the other comparisons. The difference from baseline to the subject’s last value of the respective parameter was used as dependent variable of the ANCOVAs and the model included treatment and center as factors and the respective baseline value as covariate. As an exploratory approach, a two-sided F-test was used to test the null hypothesis, that the baseline value had no influence on the difference from baseline to the subject’s last value. The P value of this test was below 0.025 for every secondary efficacy variable except for human fecal elastase 1, indicating that (except for human fecal elastase 1) it was very probable that the baseline value actually had an influence on the respective dependent variable.
Thus, the inclusion of the baseline value as covariate was fully justified.
The Wilcoxon rank test was used for analysis of subject’s assessment of CGIDS. The Fisher exact test was applied in order to compare gender between the two groups of treatment.
All tests were two-sided with a significance level of 5% and examined the hypothesis of “No difference between treatment groups” as appropriate. Subjects last values after start of treatment was the time point for main analysis. The SAS®, Version 8.2 (SAS Institute, Cary, NC, USA) statistical package was used for the analysis of data.
RESULTS
At baseline, 20 out of 56 patients suffered from pancreatic exocrine insufficiency based on fecal elastase values (n=11, pancreatic enzyme group; n=9, placebo group) and were used to generate the analysis sample. These patients only were evaluable for the primary end-point of the study.
Primary Objective
There was no statistically significant difference regarding the recovery from pancreatic exocrine insufficiency between the two treatment groups (oral pancreatic enzyme supplementation vs. placebo; P=0.641) in subjects with a fecal elastase level at baseline less than 200 μg/g stool (analysis sample). The median time to recovery from pancreatic exocrine insufficiency was 14 days in the pancreatic enzyme supplementation group and 23 days in the placebo group. The Kaplan-Meier estimate of the proportion of subjects who had recovered from pancreatic exocrine insufficiency by Day 28 was 48.1% in the oral pancreatic enzyme supplementation group vs. 76.7% in the placebo group (Figure 2).
Figure 2. Kaplan-Meier estimates of the proportion of subjects with a response (analysis sample: pancreatic exocrine insufficiency; elastase levels at baseline less than 200 μg/g stool). Both curves take a similar course and do not show any major difference from each other.
Secondary Objectives
The analysis of the secondary variables was performed both for the total study populationsample and for the analysis sample.
Body Weight
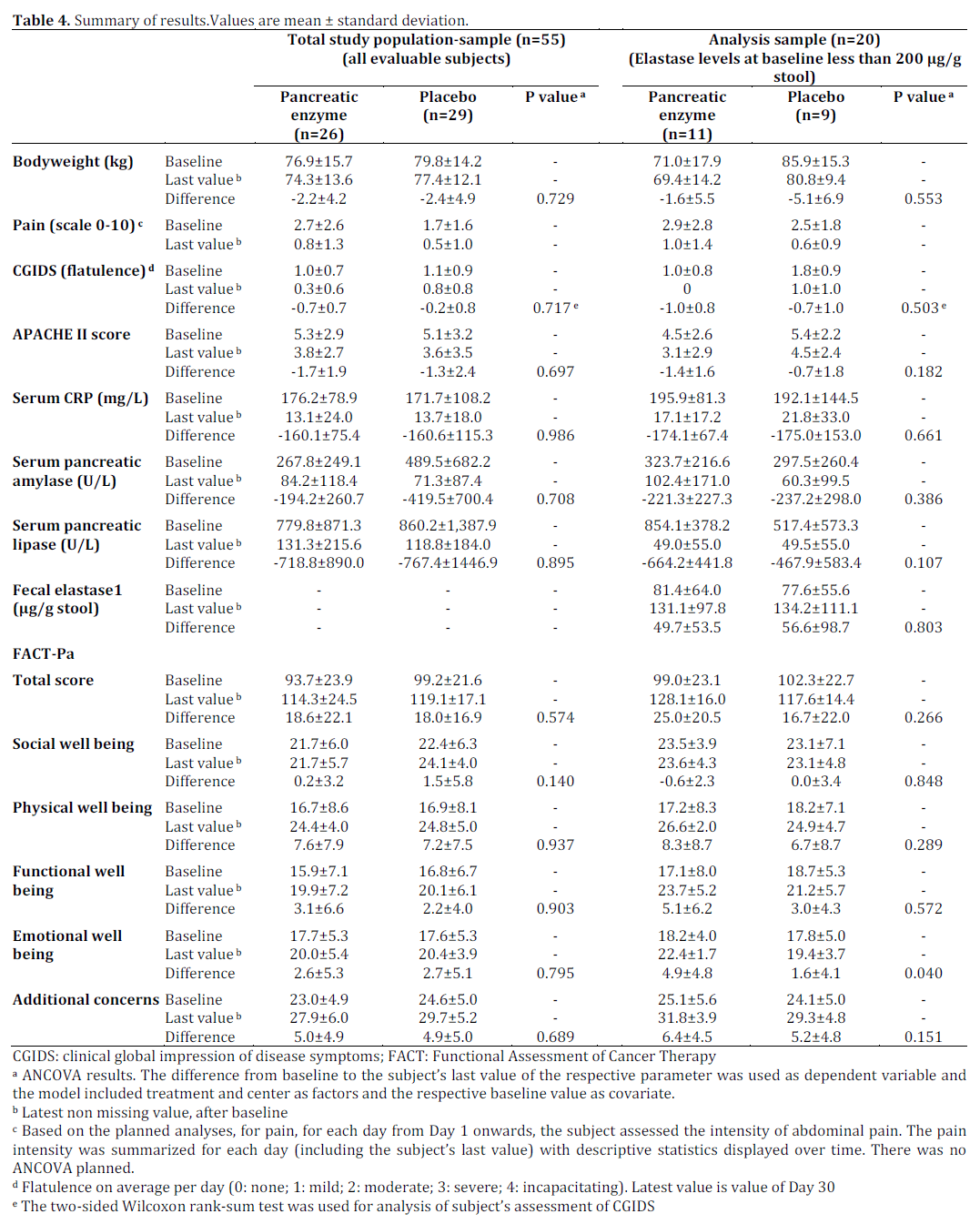
The mean change from baseline to the subjects’ last value was somewhat higher in the placebo group (- 5.1±6.9 kg compared to -1.6±5.5 kg in the oral pancreatic enzyme supplementation group; ) but the mean overall body weight was higher in the placebo group than in the oral pancreatic enzyme supplementation group at all visits (baseline: 85.9±15.3 kg vs. 71.0±17.9 kg; the patients last values were 80.8±9.4 kg vs. 69.4±14.2 kg, respectively. Thus ANCOVA results showed no significant differences between treatment groups regarding body weight mean changes (P=0.553). Details are given in Table 4.
Symptom Assessment
Pain scores between the treatment groups were not statistically significantly different. Details are given in Table 4. The investigators and subjects assessment of CGIDS of pancreatic exocrine insufficiency reflected an improvement of symptoms over time: the mean severity of flatulence was considerably higher in the placebo group than in the oral pancreatic enzyme supplementation group without reaching statistical significance.
APACHE II Score
There were no statistically significant differences regarding the APACHE II scores between both treatment groups with lower values after treatment. Details are given in Table 4.
Quality of Life
The mean total score and all subscale scores increased over time indicating an improvement of QoL, but did not show any significant difference between treatment groups except with regard to one subscore. A statistically significant difference between treatment groups in the FACT-Pa subscale score ‘Emotional well-being’ was seen in favor of oral pancreatic enzyme supplementation (P=0.040). The total score and all subscores, except the score ‘Social well being’, were higher in the oral pancreatic enzyme supplementation group than in the placebo group. Details are given in Table 4 together with ANCOVA results for the changes in all FACT-Pa scores from baseline to the subject’s last value.
C-Reactive Protein
As expected, the mean observed CRP level in both groups (placebo and pancreatic enzyme supplemantation group) was remarkably higher at the baseline visit compared to all other visits. There was no significant difference between treatment groups; the mean CRP level was similar over time between the treatment groups. ANCOVA results for the change in CRP from baseline to the subject’s last value showed no statistically significant difference between treatments (Table 4).
Serum Pancreatic Lipase and Amylase
Both treatment groups have in common, that the mean serum pancreatic amylase value at baseline was remarkably elevated compared to the following visits, as was expected. No relevant difference between treatment groups was found in the analyses sample. In the total study populationsample, a baseline difference between the two randomized groups was observed: the mean and the median baseline serum pancreatic amylase levels were higher in the placebo group than in the pancreatic enzyme supplementation group. In both, the analysis sample and the total study populationsample, the mean serum pancreatic amylase level at post-baseline visits was similar in the both groups. Thus, ignoring the baseline values in the total study population-sample, there was no major difference between treatment groups.
As expected, the mean observed serum pancreatic lipase level in both treatment groups was remarkably higher at baseline compared to all other visits. In the analysis sample, there was a baseline difference between treatment groups: the mean and the median baseline serum pancreatic lipase levels were higher in the pancreatic enzyme supplematation group than in the placebo. However, with regard to the rather large standard deviations associated with these mean values, this was not considered as a relevant difference between treatment groups.
ANCOVA results for the change in serum pancreatic amylase and lipase from baseline to the subject’s last value showed no statistically significant difference between treatment groups (Table 4).
Fecal Elastase 1
Mean observed human fecal elastase 1 showed no apparent trend, but varied substantially over time. Most of the tabulated mean values in both groups (pancreatic enzyme supplemantation group vs. placebo) in the two samples were associated with remarkably large standard deviations, which were potentially due to the high number of missing values on most target days (5 or less cases in the majority of days). The majority of the tabulated mean changes from baseline were greater than zero. This indicates, that - on most target days, and on average over all subjects - human fecal elastase 1 had increased from baseline. Mean changes from baseline varied over time, revealing no apparent trend. As expected from the above findings, neither a trend nor a major difference between treatment groups in the two samples were visible. ANCOVA results for the human fecal elastase 1 change from baseline showed no statistically significant difference between treatment groups in both samples (Table 4).
Safety Evaluation
No subject died during the study. However, one subject, who had received placebo, died 18 days after withdrawal due to myocardial insufficiency.
Three subjects experienced five serious adverse events (Medical Dictionary for Regulatory Activities (MedDRA) preferred terms: heparin-induced thrombocytopenia, acute myocardial infarction, neck pain, back pain, melaena). All serious adverse events were treatment emergent and occurred under placebo. All serious adverse events were regarded as unrelated to study medication.
Two subjects in the oral pancreatic enzyme supplementation group and three subjects in the placebo group discontinued prematurely due to treatment emergent adverse events (Table 3). The three events that led to discontinuation in the placebo group (MedDRA preferred terms: heparininduced thrombocytopenia, acute myocardial infarction, abdominal pain) were considered unrelated. The two events in the oral pancreatic enzyme supplementation group (MedDRA preferred term: both abdominal pain) were regarded as probably related to study medication or as unlikely related, respectively.
No relevant difference was observed between treatment groups with regard to laboratory abnormalities, vital signs, and the results of the physical examination (data not shown).
In summary no safety concerns arose from the study results with respect to severity, seriousness and overall frequency of adverse events, findings in laboratory parameters, vital signs and physical examination, respectively, during the treatment period.
DISCUSSION
The primary objective of this study was to evaluate the efficacy of oral pancreatic enzyme supplementation (Creon® 25,000 Minimicrospheres (mms) capsules; Abbott Laboratories GmbH (previously Solvay Pharmaceuticals GmbH), Hannover, Germany) versus placebo in patients during the refeeding phase after moderate to severe acute pancreatitis. The recovery from pancreatic exocrine insufficiency was measured using the time to response, defined as an increase of human fecal elastase to a value greater than 200 μg/g stool, as the main variable.
Data from animal studies and from clinical studies in humans have shown that pancreatic exocrine function during and early after acute pancreatitis is impaired [3, 4, 5, 7, 8, 9, 19, 20, 21, 22, 23]. Severity of, and recovery from, pancreatic exocrine insufficiency appear to depend on the severity of acute pancreatitis, the extent of pancreatic parenchymal necrosis and possibly on the etiology of acute pancreatitis, especially when comparing biliary vs. alcoholic acute pancreatitis [1, 24, 25, 26]. Less severe acute pancreatitis may explain the low rate of pancreatic exocrine insufficiency (20 out of 56 patients; 35.7%) seen in this study as the mean APACHE II score at baseline indicated rather moderate acute pancreatitis (median of 6).
Data about the beneficial effect of pancreatic enzyme treatment in subjects during the refeeding phase after moderate to severe acute pancreatitis are rare but show a significant improvement of pancreatic exocrine function if pancreatic enzymes are supplemented in the early phase of recovery [12, 27].
The primary efficacy variable was defined as the number of days between start of refeeding and the first day when a fecal elastase level of more than 200 μg/g stool was reached. However, recovery was 14 days in the oral pancreatic enzyme supplementation group vs. 23 days in the placebo group (P=0.641). The determination of fecal elastase levels to measure the extent of pancreatic exocrine insufficiency was used due to its easy application in clinical routine and the known accuracy of this parameter in pancreatic exocrine insufficiency [14, 28, 29].
There was no statistically significant difference regarding the time to response between the two treatment groups (oral pancreatic enzyme supplementation vs. placebo).
The failure to show a significant influence of oral pancreatic enzyme supplementation on pancreatic exocrine insufficiency can most probably be related to the low number of patients evaluable, since only 20 instead of the planned 80 patients were evaluable for the primary analysis. The low number of cases within the study population who had pancreatic necrosis to an extent greater than 50% may also be related to this failure, as it is known that lower extent of necrosis is associated with lesser extent of pancreatic exocrine insufficiency [24]. In our study this even potentiates the effect of the small study population. Therefore, we failed to obtain any definitive data supporting our hypothesis regarding the primary endpoint.
When evaluating the secondary study objectives, there are some notable differences between the two treatment groups.
The mean severity of flatulence was higher in the placebo group than in the oral pancreatic enzyme supplementation group (although non significant). While this phenomenon was restricted to the patients with pancreatic exocrine insufficiency, we hypothesize that flatulence is directly related to impaired pancreatic exocrine function. Pancreatic enzyme supplementation brings about a significant improvement of carbohydrate metabolism. A deficiency of pancreatic amylase activity leads to impaired digestion of carbohydrates in patients with pancreatic exocrine insufficiency. A surplus of undigested carbohydrates reaches the large intestine and is broken down by bacteria rather than being absorbed. The lower amount of undigested carbohydrates leads to a clinically relevant decrease in bacterial carbohydrate metabolism in the colon resulting in less gas (H2 and methane) production and therefore in a reduction in flatulence. A less severe body weight loss was observed in the oral pancreatic enzyme supplementation treated patients as well. Interestingly, the QoL measurement did show slight differences in patients’ well being in favor of enzyme supplementation, whereas clinical assessment (CGIDS) showed no difference. QoL measurement may be thus a measure of efficacy by which differences between treatment groups can be more readily distinguished than with global clinical assessment.
Only limited data are available about QoL after acute pancreatitis, and those studies are mostly directed at long term outcome, and indicate a longer persistence of QoL impairment [6, 30, 31]. As no questionnaire evaluated specifically for QoL measurement in patients with acute pancreatitis is available, a questionnaire was used that was previously evaluated for pancreatic cancer based on the similarity of the disease status with respect to symptoms (pain, pancreatic exocrine insufficiency, disturbances in endocrine function, weight loss) [16, 17]. The QoL data indicate that there is a tendency for a positive effect of enzyme supplementation in patients with acute pancreatitis. In addition to the overall assessment, all subscores showed a positive tendency in favor of the enzyme treatment group, with one subscale (emotional well-being) reaching statistical significance. This can probably be seen in the context of less weight loss and less intense flatulence but certainly in relation to an improvement of disease severity.
In conclusion, our study provides indication for a positive impact of enzyme supplementation therapy to the benefit of patients after acute pancreatitis. However, this effect is limited to those patients with impairment of pancreatic exocrine function (fecal elastase less than 200 μg/g stool).
In clinical routine, even at the beginning of refeeding, the severity of pancreatic exocrine insufficiency is not known. In cases of doubt, the clinician will probably decide to supplement enzymes early at the beginning of refeeding, as this can improve the course of the disease and patients symptoms [1, 3, 4, 8, 9]. Especially if enteral feedings are being used in patients with severe acute pancreatitis, enzyme supplementation should be added to the treatment regime [32].
While a clear benefit on time to recovery could not be demonstrated, data discussed here suggest the benefit of pancreatic enzyme supplementation especially on QoL in patients with pancreatic exocrine insufficiency after moderate to severe acute pancreatitis. Enzyme supplementation leads to an improvement of the general course of the disease and in the global health status (less weight loss, less flatulence, improved QoL). It can be argued that improvement of carbohydrate metabolism, but probably also improvement of fat and protein metabolism, may explain most of the findings presented here. Enzyme supplementation is well tolerated and can be safely administered from the first day of refeeding after acute pancreatitis. The results of this study encourage further studies in adequate sample size to prove these findings.
Conflict of interest
The authors have no potential conflict of interest
References
- Migliori M, Pezzilli R, Tomassetti P, Gullo L. Exocrine pancreatic function after alcoholic or biliary acute pancreatitis. Pancreas. 2004;28:359-363.
- Bozkurt T, Maroske D, Adler G. Exocrine pancreatic function after recovery from necrotizing pancreatitis. Hepato-Gastroenterol. 1995;42:55-58.
- Glasbrenner B, Buchler MW, Uhl W, Malfertheiner P. Exocrine pancreatic function in the early recovery phase of acute oedematous pancreatitis. Eur J Gastroenterol Hepatol. 1992;4:563-567.
- Gullo, L., Sarles, H., and Mott, C. B. Functional investigation of the exocrine pancreas following acute pancreatitis. Rendiconti di Gastroenterologia 1972; 4:18-21.
- Mitchell CJ, Playfourth MJ, Kelleher J, McMahon MJ. Functional recovery of the exocrine pancreas after acute pancreatitis. Scand J Gastroenterol. 1983;18:5-8.
- Fenton-Lee D, Imrie CW. Pancreatic necrosis: assessment of outcome related to quality of life and cost of management. Br J Surg. 1993;80:1579-1582.
- Uomo G, Galluci F, Madrid E, Miraglia S, Manes G, Rabitti PG. Pancreatic functional impairment following acute necrotizing pancreatitis: long-term outcome of a non-surgically treated series. Dig Liver Dis. 2010 Feb;42(2):149-52.
- Buchler MW, Hauke A, Malfertheiner P. Follow-up after acute pancreatitis: Morphology and function. In: Beger HG, Buchler MW, eds. Acute Pancreatitis. Berlin-Heidelberg: Springer-Verlag; 1987:367-74.
- Tympner F, Domschke W, Rosch W, Koch H, Demling L. The function of the hydrokinetic and ekbolic pancreas after acute pancreatitis. Z Gastroenterol. 1976;14:684-687.
- Symersky T, van Hoorn B, Masclee AA. The outcome of a long-term follow-up of pancreatic function after recovery from acute pancreatitis. JOP. 2006 Sep 10;7(5):447-53.
- Pantakar, R. V., Chand, R., and Johnson, C. D. Pancreatic enzyme supplementation in acute pancreatitis. HPB Surg. 1995; 8(3):159-162.
- Airey MC, McMahon MJ. The influence of granular pancreatin upon endocrine and exocrine function during reconvalescence from acute pancreatitis. In: Lankisch PG, ed. Pancreatic enzymes in health and disease. Springer-Verlag: Berlin-Heidelberg; 1991:129-38.
- Scheefers-Borchel, U., Scheefers, H, and Arnold, R. Pancreatic elastase1: Parameter for the diagnosis of chronic and acute pancreatitis. Lab med 1992; 16:427-432.
- Gullo L, Ventrucci M, Tomassetti P, Migliori M, Pezzilli R. Fecal elastase 1 determination in chronic pancreatitis. Dig Dis Sci. 1999;44:210-213.
- Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818-829.
- Cella DF, Tulsky DS, Gray G et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11:570-579.
- Bonomi AE, Cella DF, Hahn EA et al. Multilingual translation of the Functional Assessment of Cancer Therapy (FACT) quality of life measurement system. Qual Life Res. 1996;5:309-320.
- Cella D, Butt Z, Kindler, HL, Fuchs CS, Bray S, Barlev A, Oglesby A. Validity of the FACT Hepatobiliary (FACT-Hep) questionnaire for assessing disease-related symptoms and health-related quality of life in patients with metastatic pancreatic cancer. Quality Life Res 2013 Jun; 22(5): 1105-1112.
- Adler, G., Hupp, T., and Kern, H. F. Course and spontaneous regression of acute pancreatitis in the rat. Virchows Arch.A Pathol.Anat.Histol. 1979; 382:32-47.
- Saluja A, Saito I, Saluja M et al. In vivo rat pancreatic acinar cell function during supramaximal stimulation with caerulein. Am J Physiol. 1985;249:G702-G710.
- Niederau C, Niederau M, Luthen R, Strohmeyer G, Ferrell LD, Grendell JH. Pancreatic exocrine secretion in acute experimental pancreatitis. Gastroenterology. 1990;99:1120-1127.
- Evander A, Hederstrom E, Hultberg B, Ihse I. Exocrine pancreatic secretion in acute experimental pancreatitis. Digestion. 1982;24:159-167.
- Angelini G, Pederzoli P, Caliari S. Long-term outcome of acute necrohemorrhagic pancreatitis. Digestion. 1984;30:131-137.
- Boreham B, Ammori BJ. A prospective evaluation of pancreatic exocrine function in patients with acute pancreatitis: correlation with extent of necrosis and pancreatic endocrine insufficiency. Pancreatology. 2003;3:303-308.
- Tenner S, Sica G, Hughes M et al. Relationship of necrosis to organ failure in severe acute pancreatitis. Gastroenterology. 1997;113:899-903.
- Uhl W, Buchler MW, Malfertheiner P, Martini M, Beger HG. PMN-elastase in comparison with CRP, antiproteases, and LDH as indicators of necrosis in human acute pancreatitis. Pancreas. 1991;6:253-259.
- McMahon, M. J. Acute pancreatitis: when is enzyme treatment indicated? Digestion 1993; 54(2):40-42.
- Dominguez-Munoz JE, Hieronymus C, Sauerbruch T, Malfertheiner P. Fecal elastase test: evaluation of a new noninvasive pancreatic function test. Am J Gastroenterol. 1995;90:834-1837.
- Lankisch PG, Schmidt I, Konig H et al. Faecal elastase 1: not helpful in diagnosing chronic pancreatitis associated with mild to moderate exocrine pancreatic insufficiency. Gut. 1998;42:551-4.
- Leplege A, Hunt S. The problem of quality of life in medicine. JAMA. 1997;278:47-50.
- Soran A, Chelluri L, Lee KK, Tisherman SA. Outcome and quality of life of patients with acute pancreatitis requiring intensive care. J Surg Res. 2000;91:89-94.
- Al Omran M, Groof A, Wilke D. Enteral versus parenteral nutrition for acute pancreatitis (Cochrane Review). Cochrane Database Syst Rev. 2003;CD002837.



