Keywords
Pancreas; Pancreaticoduodenectomy; Postoperative Complications; Survival
INTRODUCTION
Pancreaticoduodenectomy (PD), or the Whipple procedure, is a complex high-risk surgical procedure performed for various malignant and benign diseases of the pancreas and periampullary region. The perioperative mortality associated with a PD has dramatically fallen over the last 80 years, from more than 25% to less than 3% [1-3]. This has been largely due to centralisation with specialisation of pancreatic surgery in large volume centres [4], improvements in preoperative care, and the availability of and advances in interventional radiology to help treat complications when they arise [5]. However, the morbidity rates associated with this procedure have remained stubbornly constant at around 40% [2,3]. Studies with complete follow-up of pancreatic ductal cancer patients report actual 5 year survival rates of 6.5% - 20% [3,6,7]. Periampullary tumours (ampullary adenocarcinomas, distal cholangiocarcinomas and duodenal cancers) are associated with more favourable survival rates [2,6,8,9]. Although the list of complications associated with PD is substantial, a pancreatic anastomotic leak with post-operative pancreatic fistula (POPF) is the single most common [10-12] and when uncontrolled, can lead to sepsis, haemorrhage and multi-organ failure which is devastating for patients [13].
The impact of postoperative leaks on recurrence rates and long-term outcomes has been reported in patients with colorectal cancer [14,15], oesophageal cancer, and in patients with gastric cancer [16]. There is, however, very little data on the impact of a pancreatic leak on long-term survival in pancreatic and/or periampullary tumours [9, 17-21]. The aim of this study was to analyse the impact of pancreatic leak/post-operative pancreatic fistula (POPF) or other complications on survival in patients who underwent a PD for ampullary, distal cholangiocarcinoma or pancreatic ductal adenocarcinoma.
METHODS
Patients
Prospectively collected data from 813 patients undergoing PD resections from 01 January 2002 - 31 December 2013 were examined. Patient medical records, a computer database and hospital computer electronic patient records were retrospectively studied identifying 455 patients who had PD performed for histopathologically confirmed pancreatic ductal, distal cholangiocarcinoma and ampullary adenocarcinomas, excluding 358 patients who had a PD for other pathologies. Of the 455 patients identified, there were 4 patients with incomplete data leaving 451 (ampullary adenocarcinomas (N=123); distal cholangiocarcinomas (N=98) and pancreatic ductal adenocarcinomas (N=230)) patients across the three cancer groups for the final analysis. Our primary endpoint was mortality. We did not look into disease free survival. Secondary study end points included assessment of postoperative complications.
Workup
Prior to PD, as we have previously described, all patients had high resolution multi-phase CT including a CT chest with or without endoscopic ultrasound (EUS) [22]. Preoperative anaesthetic assessment included cardiopulmonary exercise (CPEX) testing as we have shown that a low cardiopulmonary reserve was associated with increased risk of pancreatic leak following pancreaticoduodenectomy [23]. In addition prior to surgery, all patients were discussed in a multidisciplinary team meeting with consultant surgeons, oncologists and radiologists with specialist training and interest in HPB malignancy.
Surgery
Operations were performed with curative intent, i.e. in the absence of extensive local invasion and/or distant metastases. The standard surgical procedure consisted of a pylorus preserving pancreaticoduodenectomy with concomitant dissection of the regional lymph nodes at the anterior and posterior face of the head, around the common and proper hepatic artery, in the hepatoduodenal ligament and to the right of the superior mesenteric vein. If there was suspicion of tumour in-growth in the proximal duodenum, a classical Whipple procedure was performed. If intraoperatively minimal tumour ingrowth of the portal or superior mesenteric vein was found, a segmental or wedge resection would be considered as part of the procedure. Reconstruction consisted of a retrocolic jejunal loop with end-to-side pancreaticojejunostomy, hepaticojejunostomy and retro- but occasionally ante-colic gastro- or duodenojejunostomy. However, one of the five surgeons in our unit did perform his reconstruction differently, opting for a pancreaticogastrostomy instead. This was performed using single-layer invagination of the remnant pancreas into the posterior wall of the stomach. Stenting of the pancreatic anastomosis and fibrin glue sealant were not routinely used by all five surgeons. All patients had 2 or 3 surgical drains placed at or near the anastomosis. Patients undergoing a pancreaticoduodenectomy had drain fluid amylase measured on a daily basis until drain removal.
Assessment and Treatment of Pancreatic Leak
The severity of pancreatic fistula was judged according to the ISGPF classification scheme [24]. According to this system, a pancreatic fistula is defined as any appreciable drainage from an operatively placed drain (or a subsequently placed percutaneous drain) with an amylase content greater than 3 times the upper limit of normal serum amylase level measured on, or after, postoperative day 3. Those below this level are designated as the “no leak” group. Patients with missing drain fluid amylase values were excluded from the study (N=4). The severity of pancreatic fistula is determined based on 10 clinical criteria and then stratified into 3 levels of impact on the patient: grades A, B, and C. As emphasised elsewhere, this classification can be accurately assigned only after the clinical course has reached its completion [24]. To summarise, grade A fistulas are transient, asymptomatic biochemical fistulas, defined by only elevated drain amylase levels. Grade B fistulas are clinically apparent, symptomatic fistulas that require diagnostic evaluation and therapeutic intervention. Finally, grade C fistulas render patients in a critical condition, with sepsis and/or organ dysfunction. They require more significant interventions, usually in an intensive care setting, or surgical reexploration for definitive management. Those who die as a result of the pancreatic fistula are appropriately assigned to this severe grade of fistula. Clinical practice varied slightly within the unit, as all surgeons except for one routinely used prophylactic Octreotide (Sandostatin®, Novartis Parmaceutical, Camberley, United Kingdom) for all patients. When administered it is given at a dose of 100 micrograms subcutaneously 3 times a day for 5 days, with the length of the course being extended when necessary. In our centre, as part of their treatment, all clinically significant fistulas had Octreotide commenced as a continuous IV infusion at a dose of 50 micrograms/hour and total parenteral nutrition instituted until the fistula stops or the amylase level in the fluid becomes less than 300U/L.
Other Complications
We also gathered data on patients who had any other complication apart from a pancreatic fistula. This included complications such as cardio-respiratory complications, wound infections, urinary tract infections, any other anastomotic leaks (apart from the pancreaticojejunostomy), postoperative bleeds and mortality. The severity of these complications was stratified using the Clavien-Dindo classification [25].
In this study, patients with pancreatic anastomosis leak/ post-operative pancreatic fistula ("POPF"- ISGPF A-C) were compared to those that had no pancreatic leak/ post-operative pancreatic fistula ("No POPF") or patients that had no complications. The POPF and No POPF groups included patients with complications other than a pancreatic leak. The no complication group had no POPF and/or no other complication.
Adjuvant Treatment
Initially postoperative chemo- or radiation therapy was administered only to a few patients who participated in ESPAC trials [26,27]. Following publication of ESPAC 3 results [26] adjuvant chemotherapy is now routinely offered to those who are eligible and fit enough for it. For cholangiocarcinomas the BILCAP trial started to recruit patients and recruitment ended in December 2014. BILCAP is a multi-centre prospective, randomised phase III trial investigating the role of adjuvant chemotherapy with oral fluoropyrimidine (capecitabine) in patients following potentially curative surgical resection of a biliary tract cancer. Patients who have undergone macroscopically complete surgical resection will be randomised to receive either adjuvant chemotherapy with capecitabine or observation. Currently ESPAC 4 trial is still recruiting patients with pancreatic ductal and ampullary tumours. It is a phase III, two arm, open label, multi-centre trial randomised trial comparing combination gemcitabine and capecitabine versus gemcitabine alone.
Follow-up
All patients were followed-up life-long in the surgical clinic on a three monthly basis in the first year and then subsequently on a six monthly basis. After five years follow-up was on a yearly basis. CA 19-9 levels were monitored and an elevation in the levels prompted a CT chest, abdomen and pelvis.
Statistical Analysis
The independent samples t-test was used to compare mean age between subgroups. The Mann-Whitney U test was applied to compare non-parametric ordinal data, and the chi-squared test or Fisher’s exact test was applied for analysis of categorical variables. Overall survival and survival of each variable were calculated with Kaplan- Meier formula. Univariate analysis of risk factors affecting survival was calculated with log-rank test and multivariate analysis was calculated with Cox-regression model. We defined significant data as a P-value < 0.05 and used IBM SPSS ver. 21.0 (IBM Co., Armonk, NY, USA) as a tool of statistical analysis.
RESULTS
A total of 451 patients were identified and included in the analysis. The median follow-up was 23 months. Table 1 depicts the general patient characteristics including mean age at time of surgery, sex distribution, tumour subtype, UICC cancer staging as well as lymph node status and perioperative mortality.
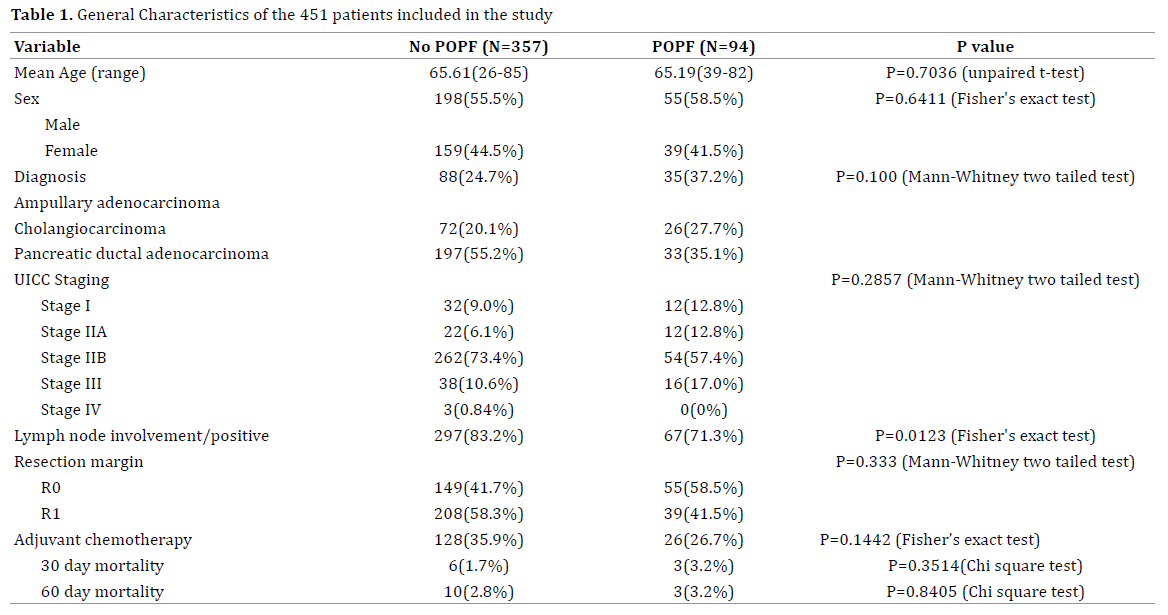
Ninety-four of the 451 patients had a POPF giving an overall pancreatic anastomotic leak rate of 20.8%. We found there to be a slight variation in the POPF rate between the tumour subtypes with ampullary adenocarcinomas (N=35 out of 123; (28.4%)) and cholangiocarcinomas (N=26 out of 98; (26.5%)) demonstrating a leak rate more than 10% higher than ductal adenocarcinomas (N=33 out of 230; (14.3%)). This is probably related to the higher incidence of concurrent pancreatitis in patients with ductal obstructing tumours and a more dilated distal duct for the anastomosis, and has been observed in a validated model for clinical risk of pancreatic fistula following proximal pancreatic resection [28]. Likewise, and probably for the same reason, the tumour staging was more advanced (Grade IIB, III and IV) in patients who did not have a POPF. Whilst patients in both the No POPF and POPF groups received adjuvant chemotherapy there was a slight difference in the proportion of patients (35/9% versus 26.7%) this was not found to be statistically significant (p=0.1442). Both the 30 day and 60 day mortality rates were also comparable.
Table 2 summarises the severity of the leak according to the ISGPF classification scheme for each of the tumour subgroups. There were less ISGPF Grade C fistulas in the ampullary subgroup when compared to the cholangiocarcinomas or ductal adenocarcinoma groups although this difference did not reach significance.

The actuarial 1, 3 or 5 year survival of each tumour subgroup is summarised in Table 3 and Figures 1-3 show the actuarial Kaplan-Meier survival plots for the same cohort of patients. There was no statistically significant difference in the median survival of patients who had a pancreatic anastomosis leak when compared to those that did not have POPF or those with no complications.
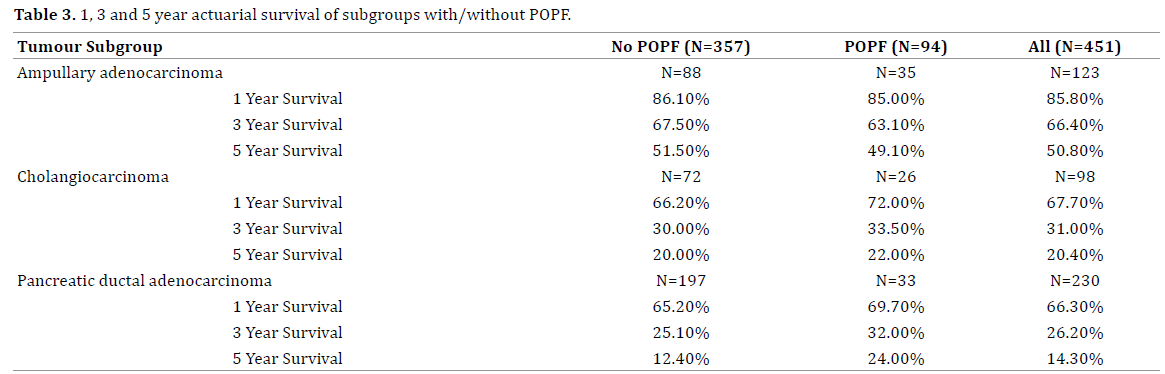
Figure 1. Survival curves for ampullary tumours. (Log-rank test P=0.580, df=2). Median survival for no POPF was 61 months versus 58 months for those
that had a POPF versus 62 months for those that had no complications.
Figure 2. Survival curves for distal cholangiocarcinomas. (Log-rank test P=0.5099, df= 2). Median survival for no POPF was 20 months versus 26 months
for those that had a POPF versus 20 months for those that had no complications.
Figure 3. Survival curves for pancreatic ductal cancers. (Log-rank test P=0.0357, df=2). Median survival for no POPF was 19 months versus 25 for those that
had a leak versus 24 months for those that had no complications.
Table 4 summarises the complication severity (Clavien- Dindo Grade) and Table 5 the details of complications that occurred in these patients. Table 6 shows the actuarial 1, 3 and 5 year survival for each of the three cancer subgroups comparing patients who had a complication other than a POPF to patients in the same subgroup who did not have any complications. Figures 4-6 show the actuarial Kaplan- Meier survival curves for the same cohorts. Patients with ampullary or pancreatic ductal adenocarcinoma, who suffered a complication other than a POPF, had a significantly reduced long term survival. This was not the case in those patients with a distal cholangiocarcinomas.

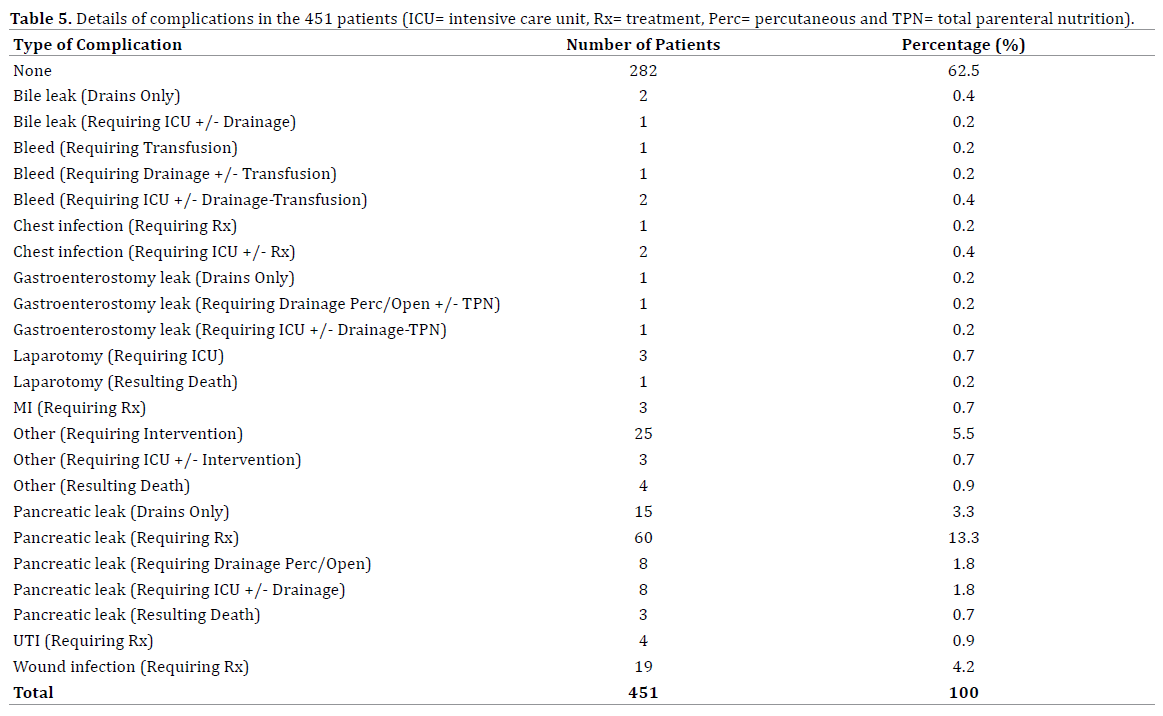
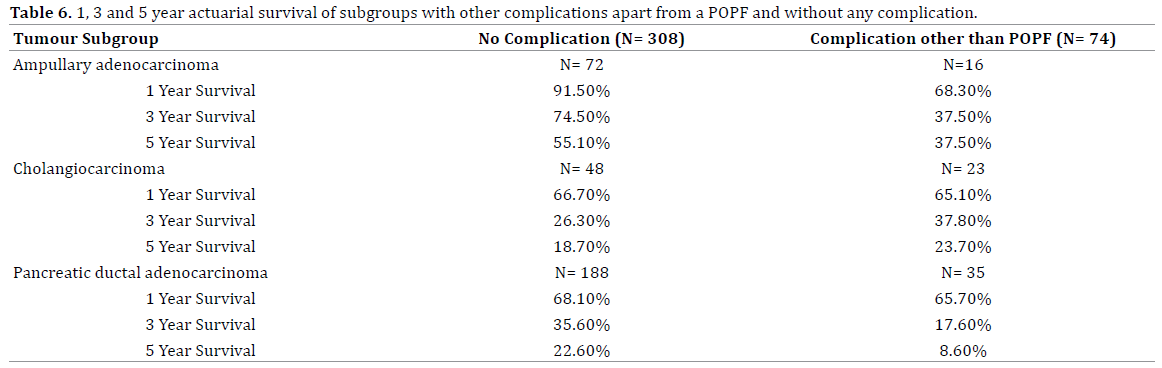
Figure 4. Survival curves for ampullary tumours any other complication versus no complications (Log-rank test P=0.079,). Median survival for those that
had any other complication was 20 months versus 62 months for those that had no complications.
Figure 5. Survival curves for cholangiocarcinomas any other complication versus no complications (Log -rank test P=0.4016). Median survival for those
that had any other complication was 26 months versus 20 months for those that had no complications.
Figure 6. Survival curves for ductal tumours any other complication versus no complications (Log-rank test P=0.0218). Median survival for those that had
any other complication was 15 months compared to 24 months for those that had no complications.
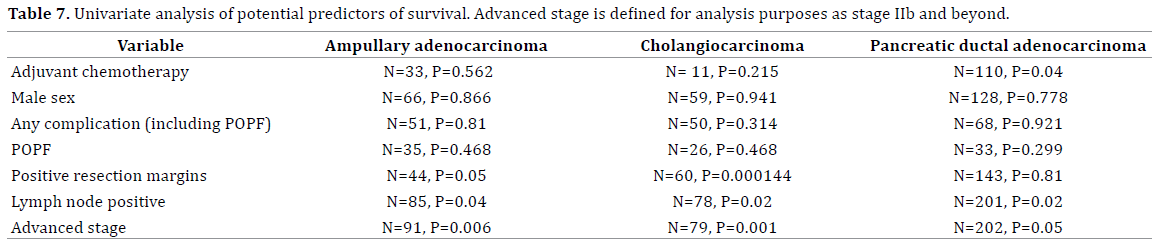
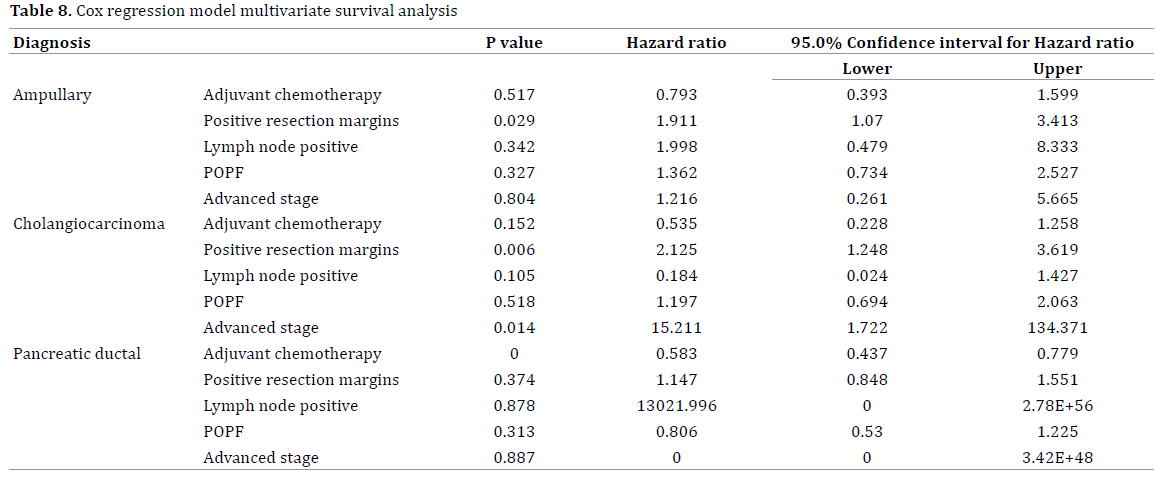
We performed a univariate analysis of different variables that we thought might have an impact on survival in the 3 histological subgroups and Table 7 summarises our findings. Of those lymph node positive status, positive resection margin, advanced stage of disease and adjuvant chemotherapy (significant only in pancreatic ductal cancers) were found to have a significant impact on survival. A POPF was not found to be a prognostic factor. A Cox regression multivariate analysis (as summarised by Table 8) also confirmed that a POPF has no impact on survival.
DISCUSSION
The difference in prognosis between the different subtypes of periampullary tumours has been extensively reported, and it has been suggested that cure from a pancreatic primary in terms of 5-year survival is exceedingly rare due to inevitable progression or recurrence [6]. This is why we chose to differentiate between ampullary, distal cholangiocarcinomas and ductal cancers when performing our analyses. Our median survival rates were comparable to those described in the literature from large volume centres [2,6,9,17,29]. Pancreatic anastomotic leaks following pancreaticoduodenectomy have an obvious negative impact on perioperative morbidity. However, it is less clear whether this effect extends itself to long term survival. The presence of a significant post-operative pancreatic leak could be associated with reduced immunity in the patient, thus leading to an increased risk of recurrence and poor survival. Some authors have demonstrated that post-operative drain fluid cytology from the pancreatic bed after ‘curative’ resection contained malignant cells and was related to long term outcome [30]. It has also been shown that exfoliated malignant cells have the potential to grow in-vitro and in immunosuppressed animal models [31].
In the literature only four other studies have looked specifically at the impact of pancreatic leaks on survival following pancreaticoduodenectomy [18-21]. In the first study [18] their results were similar to our study in that they found that a pancreatic leak following pancreaticoduodenectomy did not appear to affect long term survival. One of the main criticisms levelled at the authors has been that is was characterised by poor methodology, small sample size (N=9) and low event rate, the latter likely precluding the possibility to detect significant differences. The second study [19] included 31 patients (15 %) who developed postoperative POPF, and 179 (85 %) who did not. The 31 cases of POPF consisted of 27 grade B POPF and 4 grade C POPF. Overall 5-year survival rates for patients with and without POPF were 25 and 27% respectively. There was no significant difference in overall survival between the two groups (P=0.743). In their study, Assifi et al. [20] looked at 23 patients with pancreatic cancer who developed POPF and found that there was no significant difference in recurrence-free survival (P=0.4) and overall survival (P=0.3) for those with POPF vs those without POPF. Nagai et al. [21] compared the overall survival of patients without pancreatic fistula (POPF) and with grade B or C POPF. Survival of patients without POPF (n = 133) and with grade B or C PF (n = 46) was compared. Median survival time was 16.0 months for the no-POPF group, and 14.6 months for the grade B or C PF group. 1- and 3-year survival rates were 68 and 20% in the no-POPF group, and 57 and 24% in the grade B or C PF group. The difference did not reach statistical significance (P=0.830, log rank test).
However, a more recent study by Klein et al. [9] mentions POPF as a risk factor for decreased survival in a cohort of patients with periampullary tumours having a pancreaticoduodenectomy. A closer look at their methods reveals certain flaws such as not having drain fluid amylase levels on all their patients and a small sample size of 12 patients. Van der Gaag et al. [17] also looked at surgical complications following pancreaticoduodenectomy in patients with both pancreatic cancer and periampullary tumours. They included patients with ISGPF grade B and C only and discarded grade A leaks when performing their analysis. They concluded that complications (including pancreatic leaks) have a negative impact in pancreatic adenocarcinoma patients but not in those with other periampullary lesions. There is no mention on the exact number of patients with leaks in their paper. In all tumour subtypes, greater than 80 percent of the leaks in our series were ISGPF grade B and C.
Our initial hypothesis was that having a pancreatic leak would have a negative impact on long term survival. The delay in starting adjuvant therapy may allow any unresected cancer to grow and is often mentioned as one of the reasons why postoperative complications of any sort are to be avoided. We were, however, unable to show a statistically significant detrimental difference in the overall survival in patients with pancreatic leaks. This was on both univariate analysis and on performing a Cox regression model multivariate survival analysis. Proteases are capable of damaging both normal cells - such as in acute pancreatitis [32] - as well as tumour cells [33]. It is therefore possible that a leak of pancreatic enzymes has the potential to destroy any tumour cells that may have been spilled in the pancreatic bed intraoperatively, and explain why the survival for those with a pancreatic anastomosis leak is similar to those without a leak. Both groups of patients had received adjuvant chemotherapy and, although statistically not significant, those in the POPF group were less likely to received adjuvant chemotherapy (35.9% No POPF versus 26.7% POPF).
An even more surprising observation was in the pancreatic ductal adenocarcinoma subgroup where those with a POPF appear to do better in terms of 5 year survival that those without a fistula. This may very well be because of the small number of patients we were dealing with.
The hypothesis that development of major surgical complications results in a temporarily impaired cellular immunity, rendering patients susceptible to early cancer recurrence and reduced survival, is gaining support [34]. One earlier clinical study found that, besides pathological variables and obtaining a R0 resection, lack of postoperative complications was associated with long-term survival following resection of pancreatic adenocarcinoma [35]. Severe postoperative complications might lead to hospital mortality. At first glance with simple statistical analysis our study is in keeping with this in both patients with ampullary lesions and those with ductal cancers. Complication rates among tumour subgroups were eventually quite similar. This parallels results observed in recent studies [2,8,9,11,13,18]. It is possible that major surgery with its inherent complications might enhance any associated co-morbidities in the patient thus reducing their overall lifespan. However, this study was neither designed nor powered to look at reduced life span from non-cancer causes. This is perhaps why on univariate analysis when we included all complications (and not subanalysing them by Clavien scores) in our model this did not reach statistical significance. When we performed a Cox regression analysis we found lymph positive status was the only one consistent predictor of long-term survival in all 3 histological subgroups.
Our study seems to corroborate the findings of others, in that a post-operative pancreatic fistula does not seem to have a negative impact on patients’ long-term survival. This appears to apply not only to pancreatic ductal cancers, but also to ampullary tumours and distal cholangiocarcinomas.
Acknowledgements
Mr Avinash Sewpaul and Mr Yasser Farooque contributed equally to the analysis of the data.
Conflict of interest
The authors have no conflict of interest to declare.
References
- Neoptolemos JP, Russell RC, Bramhall S, Theis B. Low mortality following resection for pancreatic and periampullary tumours in 1026 patients: UK survey of specialist pancreatic units. UK Pancreatic Cancer Group.Br J Surg 1997;84:1370-6. [PMID: 9361591]
- He J, Ahuja N, Makary MA, Cameron JL, Eckhauser FE, Choti MA, et al. 2564 resected periampullary adenocarcinomas at a single institution: trends over three decad`es. HPB (Oxford) 2014;16:83-90. [PMID: 23472829]
- Cameron JL, Riall TS, Coleman J, Belcher KA.One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006;244:10-5. [PMID: 16794383]
- Charnley RM, Paterson-Brown S. Surgeon volumes in oesophagogastric and hepatopancreatobiliaryresectional surgery. Br J Surg 2011;98:891-3. [PMID: 21590685]
- Young J, Thompson A, Tait I, Waugh L, McPhillips G. Centralization of services and reduction of adverse events in pancreatic cancer surgery. World J Surg 2013;37:2229-33. [PMID: 23756771]
- Chen SC, Shyr YM, Wang SE. Longterm survival after pancreaticoduodenectomy for periampullary adenocarcinomas. HPB (Oxford) 2013;15:951-7. [PMID: 23472708]
- Schnelldorfer T, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, et al. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg 2008;247:456-62. [PMID: 18376190]
- Robert PE, Leux C, Ouaissi M, Miguet M, Paye F, Merdrignac A, et al. Predictors of long-term survival following resection for ampullary carcinoma: a large retrospective French multicentric study. Pancreas 2014;43:692-7. [PMID: 24713843]
- Klein F, Jacob D, Bahra M, Pelzer U, Puhl G, Krannich A, et al. Prognostic factors for long-term survival in patients with ampullary carcinoma: the results of a 15-year observation period after pancreaticoduodenectomy. HPB Surg 2014;2014:970234. [PMID: 24723741]
- Yeo CJ, Cameron JL, Lillemoe KD, Sauter PK, Coleman J, Sohn TA, et al. Does prophylactic octreotide decrease the rates of pancreatic fistula and other complications after pancreaticoduodenectomy? Results of a prospective randomized placebo-controlled trial. Ann Surg 2000;232:419-29. [PMID: 10973392]
- Haddad LB, Scatton O, Randone B, Andraus W, Massault PP, Dousset B, et al. Pancreatic fistula after pancreaticoduodenectomy: the conservative treatment of choice. HPB (Oxford) 2009;11:203-9. [PMID: 19590648]
- BalcomJHt, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg 2001;136:391-8. [PMID: 11296108]
- Reid-Lombardo KM, Farnell MB, Crippa S, Barnett M, Maupin G, Bassi C, et al. Pancreatic anastomotic leakage after pancreaticoduodenectomy in 1,507 patients: a report from the Pancreatic Anastomotic Leak Study Group. J GastrointestSurg 2007;11:1451-8, discussion 9. [PMID: 17710506]
- Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg 2011;253:890-9. [PMID: 21394013]
- Krarup PM, Nordholm-Carstensen A, Jorgensen LN, Harling H. Anastomotic leak increases distant recurrence and long-term mortality after curative resection for colonic cancer: a nationwide cohort study. Ann Surg 2014;259:930-8. [PMID: 24045445]
- Tokunaga M, Tanizawa Y, Bando E, Kawamura T, Terashima M. Poor survival rate in patients with postoperative intra-abdominal infectious complications following curative gastrectomy for gastric cancer. Ann SurgOncol 2013;20:1575-83. [PMID: 23076557]
- van der Gaag NA, Harmsen K, Eshuis WJ, Busch OR, van Gulik TM, Gouma DJ.Pancreatoduodenectomy associated complications influence cancer recurrence and time interval to death. Eur J SurgOncol 2014;40:551-8. [PMID: 24388408]
- Ausania F, Cook N, Jamieson N, Huguet E, Jah A, Praseedom R. Impact of pancreatic leaks on survival following pancreaticoduodenectomy. JOP 2010;11:226-9. [PMID: 20442516]
- Murakami Y, Uemura K, Sudo T, Hashimoto Y, Kondo N, Nakagawa N, et al. Is Pancreatic Fistula Associated with Worse Overall Survival in Patients with Pancreatic Carcinoma? World J Surg 2014; 39:500-8. [PMID: 25315091]
- Assifi MM, Zhang S, Leiby BE, Pequignot EC, Xia B, Rosato E, et al. Tumor recurrence is independent of pancreatic fistula in patients after pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. Journal of the American College of Surgeons 2013;217:621-7. [PMID: 23810574]
- Nagai S, Fujii T, Kodera Y, Kanda M, Sahin TT, Kanzaki A, et al. Recurrence pattern and prognosis of pancreatic cancer after pancreatic fistula. Ann SurgOncol 2011;18:2329-37. [PMID: 21327822]
- Mansfield SD, Scott J, Oppong K, Richardson DL, Sen G, Jaques BC, et al. Comparison of multislice computed tomography and endoscopic ultrasonography with operative and histological findings in suspected pancreatic and periampullary malignancy. Br J Surg 2008;95:1512-20. [PMID: 18942059]
- Ausania F, Snowden CP, Prentis JM, Holmes LR, Jaques BC, White SA, et al. Effects of low cardiopulmonary reserve on pancreatic leak following pancreaticoduodenectomy. Br J Surg 2012;99:1290-4. [PMID: 22828960]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138:8-13. [PMID: 16003309]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205-13. [PMID: 15273542]
- Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA 2010;304:1073-81. [PMID: 20823433]
- Neoptolemos JP, Dunn JA, Stocken DD, Almond J, Link K, Beger H, et al. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: a randomised controlled trial. Lancet 2001;358:1576-85. [PMID: 11716884]
- Callery MP, Pratt WB, Kent TS, Chaikof EL, Vollmer CM, Jr. A prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatoduodenectomy. Journal of the American College of Surgeons 2013;216:1-14. [PMID: 23122535]
- Weber CE, Bock EA, Hurtuk MG, Abood GJ, Pickleman J, Shoup M, et al. Clinical and pathologic features influencing survival in patients undergoing pancreaticoduodenectomy for pancreatic adenocarcinoma. J GastrointestSurg 2014;18:340-7. [PMID: 24272772]
- Ishikawa O, Wada H, Ohigashi H, Doki Y, Yokoyama S, Noura S, et al. Postoperative cytology for drained fluid from the pancreatic bed after "curative" resection of pancreatic cancers: does it predict both the patient's prognosis and the site of cancer recurrence? Ann Surg 2003;238:103-10. [PMID: 12832972]
- Skipper D, Jeffrey MJ, Cooper AJ, Taylor I, Alexander P. Preferential growth of bloodborne cancer cells in colonic anastomoses. Br J Cancer 1988;57:564-8. [PMID: 3408643]
- Sah RP, Dawra RK, Saluja AK.New insights into the pathogenesis of pancreatitis.CurrOpinGastroenterol 2013;29:523-30. [PMID: 23892538]
- Pan XQ. The mechanism of the anticancer function of M1 macrophages and their use in the clinic. Chin J Cancer 2012;31:557-63. [PMID: 23149314]
- Marik PE, Flemmer M. The immune response to surgery and trauma: Implications for treatment. J Trauma Acute Care Surg 2012;73:801-8. [PMID: 22976420]
- Howard TJ, Krug JE, Yu J, Zyromski NJ, Schmidt CM, Jacobson LE, et al. A margin-negative R0 resection accomplished with minimal postoperative complications is the surgeon's contribution to long-term survival in pancreatic cancer. J GastrointestSurg 2006;10:1338-45; discussion 45-6. [PMID: 17175452]







