Keywords
HIV; Depression; Telemedicine; Telepsychiatry
Introduction
With the advent of highly effective antiretroviral drugs, HIV has changed from an often terminal illness to a chronic disease. Consequentially, HIV is increasingly affecting older adults [1,2]. To compound this issue, older PLWH often manifest psychiatric comorbidities, with depressive disorders among the most common [3-6]. Telemedicine is an increasingly common model of care delivery, particularly for patients with logistical barriers to in-person specialty care. To date, there have been no studies reporting the use of telemedicine to assess depressive disorders in older PLWH in an urban setting.
Older PLWH: A growing demographic with more challenges
Over the past two decades, the number of PLWH who are 50 years and older has increased greatly [1,2]. This trend has been described as the “graying” of the HIV/AIDS epidemic [7]. Due to the common misperception of HIV/AIDS as a disease afflicting younger people, older PLWH have been referred to as a “hidden population” [8].
Older PLWH may experience a more acute sense of stigmatization, difference, and exclusion from their social sphere due to their age, which may discourage them from seeking treatment [9].
Compared to younger PLWH, older PLWH express greater unhappiness, negative life events, perceived stress, and negative attitudes about aging [10,11]. Additionally, older PLWH are more likely to experience social isolation, depressive symptoms [12], and HIV-related stigma, which may be associated with internalized shame and blame and reduced quality of life [13-15]. Similar results were found when comparing HIV-positive and HIV-negative older people–older PLWH reported less happiness, less resilience, lower physical and mental health, and poorer attitudes towards aging, as well as more negative life-events, anxiety, and perceived stress [16].
Depressive disorders in older PLWH
Depressive disorders represent a common psychiatric comorbidity among PLWH [3-6] and are associated with accelerated HIV disease progression [17,18], decreased immune functioning [17,19], HIV medication non-adherence [20], and premature death [21,22]. Older PLWH often experience mild to moderate depressive disorders such as dysthymic disorder and “minor” depression [23]. Some studies indicate depression prevalence as high as 52% for older PLWH [24], while others show that older PLWH are five times more likely to experience depression compared to HIV-negative peers [25]. The high rates of depression in older PLWH are especially disconcerting since this cohort is less likely than their younger counterparts to seek treatment [26].
Telemedicine as a clinical option
In order to treat the rising number of PLWH and their associated comorbidities, new models of care have been developed. The last two decades have seen a rising interest in delivering mental healthcare by means of advanced technologies. With a growing availability of modern communications technology, telemedicine– the incorporation of a telecommunication device in the diagnosis and overall care of patients who are geographically separated from the physician [27]–is a viable alternative. For the purpose of this paper, telemedicine refers to the provision of psychiatric services via live, interactive videoconferencing technology.
Previous studies have demonstrated that treatment of depression via telemedicine compared to in-person treatment resulted in comparable outcomes, including equivalent levels of patient adherence, patient satisfaction, and healthcare costs [28]. A meta-analysis conducted by Mohr et al. showed significant reductions in depressive symptoms across all assessment periods among individuals who engaged in telephone-administered psychotherapy compared to usual care [29]. Comparable results were also reflected in the accuracy of diagnosis. Singh et al. investigated psychiatric care for rural individuals and found that only 1-2% of patients were diagnosed incorrectly when using telemedicine [30].
Telemedicine has been successfully integrated into psychiatric care in several different settings, including rural areas and correctional facilities. Although individuals living in rural settings face greater barriers to healthcare access, such as geographic and transportation factors, high treatment costs, and time limitations, research has supported the use of telemedicine as a means to increase healthcare accessibility to rural residents.
Johnston and Jones noted both flexibility and improvements to accessibility that telemedicine offered to patients in a rural nursing home over a 2-year period [31].
Telemedicine has also been shown to fulfill the needs in correctional settings where lack of appropriate mental healthcare is a common issue. Khalifa et al. demonstrated that use of telemedicine can overcome issues related to travel, accessibility, continuity of care, public safety and security, and transportation costs [32]. Research on telemedical services in rural and correctional settings is well-documented; however, additional research is required to explore the impact of telemedicine in an urban setting.
Barriers to healthcare in urban settings can be just as burdensome as those seen in rural areas. Additional challenges to care delivery that are often reported, most commonly among Hispanic populations, include language barriers, immigration status, cultural practices, and unfamiliarity with maneuvering around the healthcare system [33]. This has resulted in delayed delivery of treatment in urban populations and/or use of local emergency departments for primary care [34], causing greater inefficiency and higher costs for the healthcare environment. Other barriers to obtaining in-person care in urban settings include patients with limited mobility, lack of access to an automobile, less-than-convenient access to public transit, cost of transit and parking for impoverished patients, and stigma for being seen in certain clinic settings. Spaulding et al. reported that as of 2011, only about 2% of the current publications on telemedicine programs and research described urban telemedicine health services. With a greater capacity to leverage telemedicine health for more patients and a better equipped infrastructure to provide technical and clinical support, more research needs to focus on urban telemedicine [35].
The current study aimed to analyze older PLWH with depression in an urban setting and how they perceive telemedicine. Additionally, the study examined changes in perception and acceptance of telemedicine after participants engaged in an actual telemedicine session and clinician opinion on using the Ham-D via telemedicine (with particular attention to the interpretation of items 1, 8, 9 and 10, which require clinician interpretation of the patient’s physical appearance).
Methods
The current 2-phase study sought to evaluate the provision of clinical services through home-based telemedicine (HBT) in an urban setting to a cohort of older PLWH ≥ 50 years of age with mild to moderate major depression based on the PHQ-9, or a score of 5-14, inclusive.
Participants and procedures: Phase I
UC San Francisco’s (UCSF) Committee on Human Research granted study approval in March 2014, after which recruitment was initiated. Initially, only patients from 360: The Positive Care Center (360) at UCSF were recruited as this clinic focused primarily on the treatment of PLWH. Based on patient records, patients at 360 who met the inclusion criteria for the study were identified and then contacted by the clinic’s social worker by telephone.
Due to slow enrollment into the study, recruitment was opened up to various HIV clinics across San Francisco in order to expedite the process.
Recruitment letters and flyers were circulated among the participating clinics and interested individuals could respond on their own initiative. A member of the research team replied to the inquiries by contacting individuals via telephone. Interested individuals were then screened and eligibility was determined based on the following: ≥50 years of age, San Francisco resident, HIV-positive, and PHQ-9 score. The research member conducted the PHQ-9, a diagnostic instrument used to screen, monitor, and measure the severity of depression, during the phone call to confirm each individual’s current psychiatric status and to ensure that each individual fell within the targeted parameters of the depression scale. Although the research member had limited clinical background, the study psychiatrist determined that screening in this fashion was still valid since the PHQ-9 is normally a self-administered test and is commonly conducted over the phone. Participants that did not fall within the desired range (a score of 5-14, inclusive) were screened out. Those whose score was greater than 14 were directed to seek psychiatric care promptly (Figure 1).
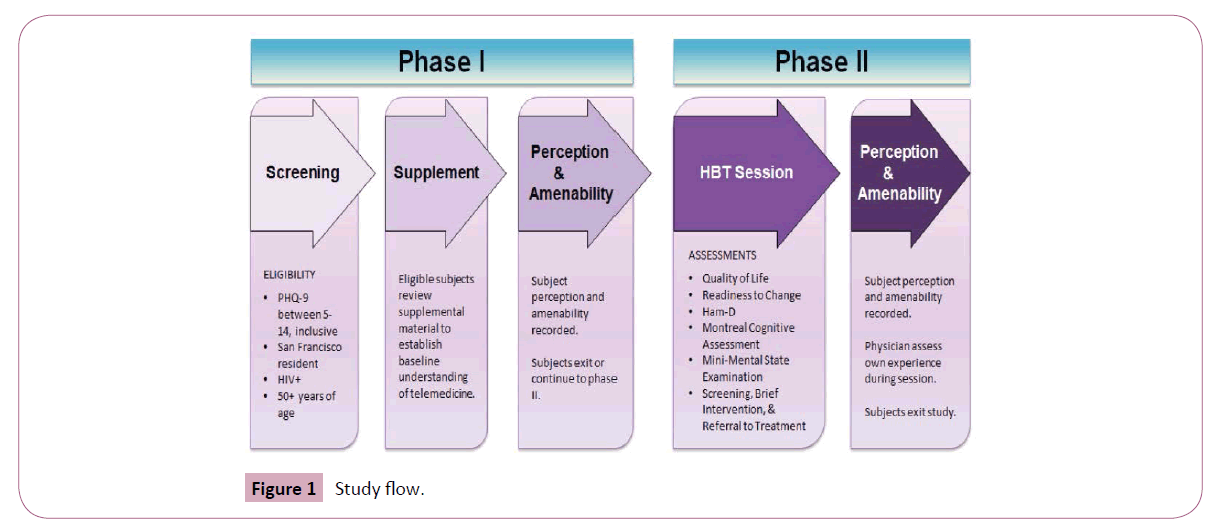
Figure 1: Study flow.
Eligible participants received informational material via email or postal delivery that further described telemedicine in order to establish a baseline level of understanding. Participants were given 3 days to review the material on their own, after which a research team member contacted them to confirm understanding of the material and to conduct the Patient Perception Questionnaire (PPQ), which aimed to assess each participant’s perception of telemedicine. Because Phase I only involved collecting participant feedback on their perceptions of and amenability toward telemedicine, individuals were not excluded from this study on the basis of alcohol or substance use disorders, cognitive status, or current psychotherapy or pharmacotherapy. Likewise, an informed consent was not conducted for Phase I as determined by UCSF’s Committee on Human Research due to the minimal risk associated with participation.
Participant amenability towards receiving telemedicine was also recorded prior to HBT session during Phase II. Amenability was defined as a participant’s willingness to participate in an actual HBT session, which would take place during Phase II of the study. Sample size for Phase I was determined by a preliminary assessment of the data after 12 months of enrollment to see whether there was statistical significance at that point in the study. Given the sample size and data at this point in the study, statistical power was confirmed. Participants received a $10 food voucher for completing Phase I of the study.
Measures
The Patient Health Questionnaire or PHQ-9 [36] is a widely used multipurpose, self-report measure for screening, diagnosing, and monitoring the severity of depression. It was conducted during the first phone call to determine the current state of mental health among respondents in order to determine eligibility. Total scores can range from 0 to 27, with higher scores indicating greater symptom severity.
The Patient Perception Questionnaire or PPQ that was administered at the end of the second phone call was based on The Duke Telemedicine Project Patient Satisfaction Survey and the UC Davis Health System Telemedicine Clinical Consultation Patient Satisfaction Survey. Permission to modify the surveys for the purposes of the study was collected from the appropriate parties before implementation. Participants were asked about their previous experience with telemedicine, then rated a series of statements regarding their perception on telemedicine on a 5-point Likert scale ranging from 1 (“Strongly Disagree”) to 5 (“Strongly Agree”) as seen in Tables 1 and 2. The PPQ concluded with a question about participant likelihood of engaging in a telemedicine consultation and an opportunity to schedule a real session with a psychiatrist to assess participant amenability.
| Variable |
Frequency |
Percent |
| Age |
| ≤55 |
10 |
44 |
| 56-65 |
13 |
56 |
| Race |
| Caucasian |
8 |
35 |
| African American |
8 |
35 |
| Asian |
2 |
9 |
| Latino/Latina |
1 |
4 |
| Other/Multiracial |
4 |
17 |
| Gender |
| Female |
5 |
22 |
| Male |
18 |
78 |
| *Values are based on responses from 23 of the 25 participants from phase II |
Table 1: Demographic characteristics during phase II.
| Scale |
N |
Mean |
Standard Deviation |
| PHQ-9 |
| Phase I |
16 |
8.875 |
2.778 |
| Phase II |
25 |
10.800 |
2.217 |
| Phases I & II |
41 |
10.049 |
2.5976 |
| Ham-D |
| Phase II |
25 |
10.76 |
5.988 |
Table 2: Patient Health Questionnaire (PHQ-9) and Hamilton Depression Rating Scale (Ham-D): Mean and Standard Deviation.
Participants and procedures: Phase II
During this phase, amenable participants who completed Phase I engaged in an HBT session at their home. 360 was offered as an alternate, private location for those who preferred to hold the session elsewhere as the study team anticipated that some individuals may feel uncomfortable holding the study visit at their home due to lack of privacy. During the HBT session, a research member with IT specialty and a social worker set up the telecommunication devices, which included UCSF-provided laptops, WiFi, and Cisco Jabber (two-way video). Afterwards they left the room to maintain privacy between the participant and study physician. A similar protocol was followed for individuals who chose to have their session at 360 where the physician would manage the session from a private office in a separate building. Two members went together for personal safety and in case any mental health crisis arose during the interview. The members were prepared to contact the San Francisco mobile crisis team or the police in case of any suicidal ideation, homicidal ideation, or other possible psychiatric crisis.
During the session, the study physician guided the participant through an informed consent form specific to Phase II and administered the Quality of Life and the Readiness to Change surveys. Then the study physician conducted the clinical interview during which the Hamilton Rating Scale for Depression (Ham-D), a clinician-administered depression rating instrument, was administered in order to further assess depression symptoms. The clinical interview also included the Screening, Brief Intervention, and Referral to Treatment (SBIRT) in order to determine each participant's substance abuse history and an assessment for any other psychiatric co-morbidity. The Montreal Cognitive Assessment (MoCA) and the Mini-Mental State Examination (MMSE) were both administered in order to determine participants’ current cognitive status. Each participant then completed a Post-HBT Patient Perception Questionnaire (PHPPQ) regarding their satisfaction with the HBT session while the physician completed his or her own survey to collect their perspective on the session. Sample size was based on the number of participants who were amenable to continuing the study after completing Phase I. Participants received a $20 food voucher for completing Phase II of the study.
Measures
Quality of Life Enjoyment and Satisfaction Questionnaire– Short Form or Q-LES-Q-SF [37] was administered by the study psychiatrist during the HBT session. Participants were asked to rate how satisfied they were in various aspects of their life using a 5-point Likert scale ranging from 1 (“Very Poor”) to 5 (“Very Good”). Scores can range from 14 to 70, with higher scores indicating better quality of life.
The Readiness to Change survey [38] asked participants to reflect on how they felt about the ways in which they try to stay healthy. Answers were based on a 6-point Likert scale ranging from 1 (“Strongly Disagree”) to 6 (“Strongly Agree”). It was conducted by the study psychiatrist during the HBT session and helped to provide insight into how willing each participant was to adopt new practices.
The Hamilton Depression Rating Scale or Ham-D [39] is the most widely used clinician-administered assessment scale that is used to assess the severity of, and change in, depressive symptoms in adults over the past week. Participant responses were based on a Likert scale and scores range from 0 to 53, with higher scores indicating greater severity of depression.
Montreal Cognitive Assessment or MoCA [40] was designed as a rapid screening instrument for mild cognitive dysfunction. It assesses multiple cognitive domains, including attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation. Scores can range from 0 to 30 where a score of 26 or greater is considered normal.
Mini-Mental State Examination or MMSE [41] is a questionnaire used to indicate the severity and progression of cognitive impairment. The questionnaire provides measures of orientation, registration (immediate memory), short-term memory (but not long-term memory), and language functioning. Scores can range from 0 to 30 where a score of 24 or greater indicates no cognitive impairment.
Both the MoCA and MMSE are used clinically in the assessment of depression, as cases of depression often have mild impairments on these two instruments.
Screening, Brief Intervention, and Referral to Treatment or SBIRT [42] was conducted by the study psychiatrist to gather details about each participant’s history of alcohol and substance abuse.
The Post-HBT Patient Perception Questionnaire or PHPPQ measured the same items as the PPQ during Phase I; however, the questions were modified slightly to assess participant perception after engaging in an actual telemedicine session (Tables 1 and 2). Demographic data was also collected at this time as outlined in Table 3. The PHPPQ aimed to document any changes in perception toward telemedicine before and after engaging in a real HBT consultation.
| |
Comment (Pre-Questionnaire/Post) |
Strongly Agree |
Agree |
Undecided (3) |
Disagree (2) |
Strongly Disagree (1) |
N/Mean |
N/Mean |
Mean Difference |
P-Value |
| -5 |
-4 |
PRE-QUESTIONNAIRE |
POST-QUESTIONNAIRE |
POST-PRE |
CHI-SQUARED |
| 1 |
I would be able to talk freely over telemedicine/I felt like I could talk freely over telemedicine |
| Post Phase I |
11 |
8 |
2 |
4 |
0 |
25/4.040 |
23/4.696 |
0.739 |
0.026 |
| Post Phase II |
16 |
7 |
0 |
0 |
0 |
| 2 |
I would be/was satisfied with the overall quality of care provided through telemedicine |
| Post Phase I |
1 |
10 |
9 |
3 |
2 |
25/3.200 |
22/4.682 |
1.546 |
p < 0.001 |
| Post Phase II |
15 |
7 |
0 |
0 |
0 |
| 3 |
I would be/was satisfied with the mental health or substance abuse services given through telemedicine |
| Post Phase I |
5 |
14 |
2 |
3 |
1 |
25/3.760 |
22/4.409 |
0.682 |
0.028 |
| Post Phase II |
12 |
7 |
3 |
0 |
0 |
| 4 |
I feel my time with the physician would be/was private |
| Post Phase I |
6 |
9 |
2 |
5 |
3 |
25/3.400 |
22/4.545 |
1.182 |
0.015 |
| Post Phase II |
15 |
6 |
0 |
0 |
1 |
| 5 |
I feel like the physician would be able to thoroughly explain/thoroughly explain what was being done for my medical condition |
| Post Phase I |
5 |
13 |
3 |
3 |
1 |
25/1.061 |
23/4.391 |
0.696 |
0.037 |
| Post Phase II |
13 |
6 |
4 |
1 |
1 |
| 6 |
I feel like it would be/was easy for me to talk to a physician via telemedicine equipment |
| Post Phase I |
8 |
12 |
0 |
4 |
1 |
25/3.880 |
23/4.783 |
0.957 |
0.009 |
| Post Phase II |
18 |
5 |
0 |
0 |
0 |
| 7 |
I feel like the sound quality would be/was good |
| Post Phase I |
3 |
11 |
7 |
2 |
2 |
25/3.440 |
23/4.609 |
1.174 |
0.001 |
| Post Phase II |
16 |
6 |
0 |
1 |
0 |
| 8 |
I feel like the image quality would be/was good |
| Post Phase I |
2 |
13 |
7 |
2 |
1 |
25/3.520 |
23/4.522 |
1 |
0.001 |
| Post Phase II |
15 |
6 |
1 |
1 |
0 |
| 9 |
Overall, I would be/was satisfied with a/the telemedicine visit |
| Post Phase I |
4 |
13 |
4 |
1 |
2 |
24/3.667 |
23/4.783 |
1.136 |
0.001 |
| Post Phase II |
18 |
5 |
0 |
0 |
0 |
| 10 |
I would prefer/prefer to use telemedicine instead of going to see a psychiatrist in-person |
| Post Phase I |
4 |
2 |
6 |
9 |
4 |
25/2.720 |
21/4.810 |
2.048 |
p < 0.001 |
| Post Phase II |
18 |
2 |
1 |
0 |
0 |
| 11 |
Telemedicine is of value to me and my community |
| Post Phase I |
6 |
13 |
5 |
1 |
0 |
25/3.960 |
22/4.545 |
0.546 |
0.047 |
| Post Phase II |
13 |
8 |
1 |
0 |
0 |
Table 3: Patient responses regarding their perception of a telemedicine session pre/post phase II intervention.
The Provider Questionnaire assessed the perspective of the physician who conducted the telemedicine session during Phase II of the study. Study psychiatrists were asked to rate several statements, as outlined in Table 4, based on a 5-point Likert scale ranging from 1 (“Disagree”) to 5 (“Agree”). It was completed after each telemedicine session in order to validate the use of the Ham-D via telemedicine.
| Comment (Pre-Questionnaire/Post) |
Strongly Agree
-5 |
Agree
-4 |
Undecided (3) |
Disagree (2) |
Strongly Disagree
-1 |
P-Value |
| 1 |
I feel my time with the physician would be/was private |
| Phase I Only (non-amenable) |
1 |
8 |
7 |
0 |
0 |
0.011 |
| Phase II (amenable) |
6 |
9 |
2 |
5 |
3 |
| 2 |
I would be able to understand/understood the recommendation(s) of the physician |
| Phase I Only (non-amenable) |
5 |
8 |
3 |
0 |
0 |
0.046 |
| Phase II (amenable) |
7 |
16 |
0 |
2 |
0 |
| 3 |
I feel like it would be/it was easy for me to talk to a physician via telemedicine equipment |
| Phase I Only (non-amenable) |
1 |
13 |
2 |
0 |
0 |
0.026 |
| Phase II (amenable) |
8 |
12 |
0 |
4 |
1 |
Table 4: Patient responses regarding their perception of a telemedicine session pre/post phase II intervention: phase I only vs. phase II patients.
Statistical analysis
Data were initially summarized and reported by age group, race and gender. The Hamilton Depression Rating Scale was summarized by score and with the mean and standard deviation for Phase I, Phase II and for both phases combined. Analyses of the questionnaire used a Chi-squared test to compare pre- and post-phase responses for all patients and in a paired analysis looking only at patients completing both phases. All analyses used p<0.05 as the criterion for statistical significance. Data were analyzed using Stata 14.0 (StataCorp, College Station, TX).
Results
Quantitative analysis
Of the 41 participants that completed Phase I, 37 were initially amenable to telemedicine and expressed interest in continuing on to Phase II telemedicine. However, due to logistical delay in initiating Phase II, only 25 participants completed Phase II. Based on the parameters that were set forth at the beginning of the study, amenable participants were defined as those who engaged in an actual telepsychiatry session; thus, the individuals who initially agreed to continue on to Phase II, but later declined to continue were included in the non-amenable group. Specifically, 4 participants initially exited the study after completing Phase I. Eventually an additional 12 participants exited the study before completing Phase II, citing reasons that included: Moving out of state, having other conflicting social issues, and failing to respond (either due to loss of interest or outdated contact information). When analyzing the data, the 25 participants who completed Phase II were classified as amenable and the remaining 16 participants were considered non-amenable. Demographic characteristics are shown in Table 3 and are based on those who participated in Phase II, although 2 individuals during Phase II did not complete the demographic data section and were excluded from analyses. Most participants were either African American (35.0%) or Caucasian (35.0%) with a greater male preponderance. More than half (56.0%) were ≥ 56 years of age. Demographics for Phase I were not tabulated (Table 3).
As shown in Table 2, the mean PHQ-9 score of participants who only engaged in Phase I of the study was 8.875 ± 2.778, whereas the mean PHQ-9 score of participants who moved on to Phase II was 10.800 ± 2.217. The overall mean for all 41 participants was 10.049 ± 2.5976. In Phase II, the mean Ham-D score was 10.76 ± 5.988. A total of 7 participants had a Ham-D score of 16 or greater, consistent with the literature for a diagnosis of major depression. Based on the Ham-D scores, the majority of the patients completing the interview would be classified as dysthymic disorder or depressive disorder NOS (minor depression). PHQ-9 and Ham-D score breakdown are available upon request (Table 5).
| |
Question |
Agree |
Moderately Agree |
Neutral |
Moderately Disagree |
Disagree |
Better than in Person |
Same as in Person |
Not as Good as in Person |
Image did not allow adequate observation to interpret behavior |
Image significantly affected my ability to interpret behavior |
Image slightly affected my ability to interpret behavior |
Image was not as good as in-person encounter, but did not affect my ability to interpret behavior |
Image was essentially indistinguishable from in-person encounter |
| 1 |
Overall, I was satisfied with the telemedicine visit |
| Frequency |
14 |
9 |
1 |
1 |
0 |
- |
- |
- |
- |
- |
- |
- |
- |
| N/Percent |
25/56% |
25/36% |
25/4% |
25/4% |
25/0% |
- |
- |
- |
- |
- |
- |
- |
- |
| 2 |
I would prefer to use telemedicine to treat patients instead of seeing the patient in-person |
| Frequency |
2 |
1 |
4 |
15 |
3 |
- |
- |
- |
- |
- |
- |
- |
- |
| N/Percent |
25/8% |
25/4% |
25/16% |
25/60% |
25/12% |
- |
- |
- |
- |
- |
- |
- |
- |
| 3 |
Telemedicine is of value to me and my community |
| Frequency |
25 |
0 |
0 |
0 |
0 |
- |
- |
- |
- |
- |
- |
- |
- |
| N/Percent |
25/100% |
25/0% |
25/0% |
25/0% |
25/0% |
- |
- |
- |
- |
- |
- |
- |
- |
| 4 |
I think the quality of medical care given through telemedicine is… |
| Frequency |
- |
- |
- |
- |
- |
1 |
15 |
9 |
- |
- |
- |
- |
- |
| N/Percent |
- |
- |
- |
- |
- |
25/4% |
25/60% |
25/36% |
- |
- |
- |
- |
- |
| 5 |
Q1: Depressed mood |
| Frequency |
- |
- |
- |
- |
- |
- |
- |
- |
0 |
0 |
0 |
7 |
18 |
| N/Percent |
- |
- |
- |
- |
- |
- |
- |
- |
25/0.00% |
25/0.00% |
25/0.00% |
25/25.00% |
25/72.00% |
| 6 |
Q8: Retardation |
| Frequency |
- |
- |
- |
- |
- |
- |
- |
- |
0 |
0 |
2 |
8 |
15 |
| N/Percent |
- |
- |
- |
- |
- |
- |
- |
- |
25/0.00% |
25/0.00% |
25/8.00% |
25/32.00% |
25/60.00% |
| 7 |
Q9: Agitation |
| Frequency |
- |
- |
- |
- |
- |
- |
- |
- |
0 |
0 |
0 |
11 |
14 |
| N/Percent |
- |
- |
- |
- |
- |
- |
- |
- |
25/0.00% |
25/0.00% |
25/0.00% |
25/44.00% |
25/56.00% |
| 8 |
Q10: Anxiety Psychic |
| Frequency |
- |
- |
- |
- |
- |
- |
- |
- |
0 |
0 |
0 |
8 |
17 |
| N/Percent |
- |
- |
- |
- |
- |
- |
- |
- |
25/0.00% |
25/0.00% |
25/0.00% |
25/32.00% |
25/68.00% |
Table 5: Provider questionnaire responses post-intervention during phase II.
Pre- and post-session data among those who completed both phases were analyzed using paired t-tests and chi-squared tests. All tests were 2-sided and p<0.05 was the criterion for statistical significance. As illustrated in Table 1 (chi-squared), 11 variables (comments #1-11) show significant p-values, indicating a significant shift in positive outlook towards telemedicine before and after the Phase II telemedicine session. Among the significant variables were: ability to talk freely over telemedicine (p=0.026), sense of privacy (p=0.015), ease with talking to a physician via telemedicine (p=0.009), quality of sound and image (p=0.001 for both), overall satisfaction with the telemedicine visit (p=0.001), preference for telemedicine over in-person consultation (p<0.001), and personal and community value of telemedicine (p=0.047). Additionally, participants were more likely to agree that the quality of medical care given through telemedicine is the same as or better than an in-person consultation after having completed an actual telemedicine session compared to before completing one (81.82% vs. 48.00%, p=0.011). Table 3 does not include the following data: standard deviation, chi-squared value, degrees of freedom, percent breakdown for each response, and values for non-significant variables; however, these values are available upon request (Table 1).
Table 2 compares responses between amenable participants (i.e., those who completed Phase I and were willing to continue the study into Phase II) and participants who were not amenable to an HBT session (i.e., those who completed Phase I only and declined to participate in Phase II of the study). Compared to amenable participants, those who were not amenable to scheduling an HBT session were more likely to be unsure about the privacy of such sessions (43.8% vs. 8.0%, p=0.011), less likely to agree about their ability to understand physician recommendations via telemedicine (50.0% vs. 64.0%, p=0.046), and less likely to strongly agree about the ease with which they could talk to a physician via telemedicine (6.30% vs. 32.0%, p=0.026). Interestingly, when participants were asked whether, if given the chance, they would theoretically engage in a telemedicine session and whether they would like to continue the study by scheduling a real telemedicine session, the former question was found to be statistically non-significant while the latter was significant (p=0.004). Furthermore, among the 16 nonamenable participants who completed only Phase I, 12 answered yes to the theoretical question of engaging in a telemedicine session; however, they ultimately declined to continue. On most items listed in Table 2, there were no significant differences between amenable and non-amenable participants. Table 2 does not include the following data: Chi-squared value, degrees of freedom, percent breakdown for each response, and values for non-significant variables; however, these values are available upon request (Table 2).
On Table 4, the physician responses following the Phase II HBT sessions are tabulated. After 25 Phase II sessions, the physicians either agreed or moderately agreed that they were satisfied with the quality of the telemedicine session, all responses agreed that telemedicine was of value as a care medium, and 15 of the responses (60.0%) indicated that telemedicine was of similar quality to in-person care. Eighteen physician responses (72.0%) said they would not prefer telemedicine over in-person care. When assessing ability to interpret patient behavior on items 1, 8, 9, and 10 on the Ham-D, 18 responses (72.0%) indicated that the image was essentially the same as an in-person encounter when assessing depressed mood (item 1), 15 responses (60.0%) marked the same answer when assessing psychomotor retardation (item 8), 14 response (56.0%) selected this when assessing agitation (item 9), and 17 responses (68.0%) marked this when assessing anxiety (item 10). There were no physician responses reporting that the image significantly impacted ability to interpret behavior for any of these items (Table 4).
Qualitative observations
The majority of patients who participated in the study were low-income and living in public or subsidized housing in San Francisco. Out of the 25 participants who engaged in Phase II, 15 chose to hold their HBT session at their home while the remaining 10 opted to hold the session at 360. Although telemedicine enables participants to receive care from the convenience of their home, we offered the clinic as an alternate, private location in case participants preferred to hold their session elsewhere. Participants that chose to have their session at the clinic still engaged in a telepsychiatric interview using UCSF-issued devices; however, the physicians conducted the sessions from outside the clinic to maintain consistency with the delivery of treatment. Reasons for holding the telemedicine session at the clinic included issues with housing, such as difficulties with housing management or lack of adequate space, and personal preference. Several participants were uncomfortable with allowing research members into their home to set up the telecommunication equipment, sometimes citing uneasiness with strangers or embarrassment about the condition of their living space.
Those who opted for an HBT session at home were welcoming to the research members. Although many cleaned their homes in anticipation for the visit, the research members were faced with a variety of home scenarios: One participant answered the door in undergarments; another had smoking paraphernalia exposed on his coffee table; a third participant’s home was thick with cigarette smoke, making it difficult to breathe. Fortunately, no mental health crisis arose during the study. However, having two research members was optimal as it allowed one member to set up equipment while the other engaged with the patient. This dynamic proved useful especially at times when it took up to 45 min of troubleshooting to establish connection via Jabber.
Discussion
Principal results
The early results from this study have affirmed the feasibility of using telemedicine as a viable alternative to normal standard of care for HIV-positive patients over the age of 50 with mild-moderate depressive symptoms in an urban setting. Despite limitations in sample size, this study offers insight into the feasibility of telepsychiatry, demonstrating statistically significant changes in perception favoring telepsychiatry. Showing feasibility, even in a small group, is the first step leading to a larger study in a broader group of patients. The benefit of using 2-way video in the delivery of psychiatric care is that the physician is able to analyze the nuances of patient communication to a greater extent, such as having the ability to view facial expressions and body language.
The completion of standardized clinical psychometric measures (including the Ham-D, MoCA, and MMSE) through the medium of telemedicine was supported by this study. The MoCA and MMSE were included as part of the overall psychiatric evaluation; however, the study did not specifically measure the clinicians’ views on administering these assessments as was done for the Ham-D. Clinician rating of the reliability of these instruments via telemedicine was sufficient such that these results can be considered reliable. This will become important when longitudinal studies are conducted through telemedicine for detailed analysis of outcomes in mood disorders.
Relatively few patients had a Ham-D score >16, despite the screening PHQ-9. This suggests that the PHQ-9 range chosen under-called MDD, suggesting either a placebo response to the telemedicine encounter or patients over-endorsing symptoms on the PHQ-9.
The results from this study, especially those that were found in the pre- and post-session questionnaire comparison, suggested significant improvement of the perception towards telemedicine after the HBT session by this patient population. In one case, a participant who had openly expressed skepticism pre-session commented that, “If I had a hat, I would eat it” upon completion of his HBT session.
This study demonstrated that telemedicine can be an accepted medium for psychiatric care in the PLWH population. There may be patients who are reluctant to attend a psychiatric clinic (for fear of “stigma” for seeking psychiatric treatment) and even resist seeking care from a psychiatrist in an embedded care model within HIV care models. In addition, psychiatric symptoms/illness may make patients more reticent to leave home to seek any clinical care.
Although preference for holding the telemedicine session at the clinic may have posed additional inconveniences for participants in this study, current technology allows patients to download and utilize free software, eliminating any discomfort associated with welcoming individuals into the privacy of one’s home. Young et al. found that most barriers to adopting home-based health information technology for older adults fell into one of four categories: technological discomfort, privacy or security concerns, lack of relative advantage, and the undesirable perception of users of such systems. In order to alleviate these challenges, telemedicine systems can incorporate familiar computer applications, address privacy and security concerns, and align with older adults’ self-image and identity [43]. For those willing to have psychiatric care conducted via telemedicine while remaining at home and who have the appropriate technology available, this model may represent a viable alternative.
The current study extends prior work on telemedicine for the care of depression in rural and correctional settings by studying a particular demographic in an urban area. As many urban dwelling patients still face barriers to obtaining in-person clinical services (e.g. transportation barriers, physical or financial limitations, difficulty navigating in-person systems of care), the potential demand for telemedicine services in an urban area may prove to be significant. This study is also the first to specifically analyze depression in older HIV+adults, a group often considered to be underserved in models of care. The use of telemedicine for the care of depressive disorders in this population may prove to be a viable policy option for urban care systems serving HIV patients.
Future studies may be considered to generalize the conclusions of this study beyond the assessment of depressive disorders in PLWH. Many PLWH may experience trauma and stressor-related disorders, anxiety disorders, neurocognitive disorders, bipolar disorders, and psychotic disorders. Application of this clinical paradigm of telemedicine to these other psychiatric illness groups would be the logical next step in developing a more comprehensive range of psychiatric services by telemedicine.
The broader issue of providing home-based telemedicine service is a compelling one. Issues of computer access, privacy/security concerns, and the logistics of having a clinical team going on-site to provide a secure computer system to complete telemedicine interviews would need to be addressed from a legal, logistical, and regulatory point of view before such a model could become a more routine method of clinical service. Issues pertaining to costs of supporting telemedicine as a routine clinical intervention would also need to be addressed in a systematic way before this delivery of care could be generalized to routine models of care in non-research settings.
Conclusion
Given the high prevalence of depressive disorders in older PLWH, alternative care models may be developed to deliver high quality and patient-centered care in the context of overall medical interventions. HBT for the assessment of depressive disorders in older PLWH in an urban setting shows significant promise as an alternative care delivery model for the comprehensive psychiatric and systemic medical care for this patient group.
Limitations
Limitations of the study include a focus on a specific systemic illness and psychiatric illness co-morbidity in an older population in an urban setting. It may be that in rural settings, where there is limited local access to in-person psychiatric services, there may be a greater acceptance of telemedicine than in an urban setting, where such services may be at least physically proximate. A comparison study of the same patient demographic in a rural setting could address this issue. It may also be that HIV patients with mood disorders experience “double stigma” associated with having two illnesses, which may affect their acceptance of novel medical interventions in ways that need further elucidation. Other limitations include small sample size and the use of multiple forms of technology, including email, phone, and laptop, which may have influenced overall patient satisfaction or perception.
Author Contributions
1. Jessica Y Rhee: Research design, study recruitment, data collection, overall project coordinator, critical revision of manuscript.
2. Eric J Chan: Clinical interviews, critical revision of manuscript.
3. Paul M Elizondo III: Clinical interviews, critical revision of manuscript.
4. James A Bourgeois: Research design, clinical interviews, critical revision of manuscript.
5. Cameron W Foreman: Study equipment preparation, critical revision of manuscript.
6. Lisa Dazols: Study equipment preparation, critical revision of manuscript.
7. Jorien G Breur: Clinical interviews, critical revision of manuscript.
8. Joseph K Shemuel: Study equipment preparation, critical revision of manuscript.
9. Amanda R Martin: Study equipment preparation, critical revision of manuscript.
10. Sharonya Shrivastava: Study equipment preparation, critical revision of manuscript 11. Isabel E Allen: Data analysis and interpretation, critical revision of manuscript.
12. Malcolm D John: Research design, critical revision of manuscript.
Funding Sources
This study was locally funded by the Departments of Internal Medicine and Psychiatry at UC San Francisco.
References
- Centers for Disease Control and Prevention (2008) HIV/AIDS among persons aged 50 and older. CDC HIV/AIDS facts. Atlanta pp: 1-2.
- Mack KA, Ory MG (2003) AIDS and older Americans at the end of the twentieth century. J Acquir Immune Def Syndr 33: S68-S75.
- Kalichman SC, Benotsch E, Suarez T, Suarez T, Catz S, et al. Health literacy and health-related knowledge among persons living with HIV/AIDS. Am J Preventive Med 18: 325-331.
- Ciesla JA, Roberts JE (2001) Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry 158: 725-730.
- Kilbourne AM, Justice AC, Rabeneck L, Barradas MR, Weissman S, et al. (2001) General medical and psychiatric comorbidity among HIV-infected veterans in the post-HAART era. J Clin Epidemiol 54: S22-S28.
- Rabkin JG (2008) HIV and depression: 2008 review and update. Curr HIV/AIDS Rep 5: 163-171.
- Gorman C (2006) The graying of AIDS. Time 168: 54-56.
- Emlet CA (1997) HIV/AIDS in the elderly: A hidden population. Home Care Provider 2: 69-75.
- Schrimshaw EW, Siegel K (2003) Perceived barriers to social support from family and friends among older adults with HIV/AIDS. J Health Psychol 8: 738-752.
- Rueda S, Law S, Rourke SB (2014) Psychosocial, mental health, and behavioral issues of aging with HIV. Curr Opin HIV AIDS 9: 325-331.
- Do AN, Rosenberg ES, Sullivan PS, Beer L, Strine TW, et al. (2014) Excess burden of depression among HIV-infected persons receiving medical care in the United States: Data from the medical monitoring project and the behavioral risk factor surveillance system. PLoS ONE 9: e92842.
- Klug G, Lacruz ME, Emeny RT, Häfner S, Ladwig KH, et al. (2014) Aging without depression: A cross-sectional study. Psychdyn Psychiatry 42: 5-22.
- Foster PP, Gaskins SW (2009) Older African Americans’ management of HIV/AIDS stigma. AIDS Care21: 1306-1312.
- Emlet CA (2005) Measuring stigma in older and younger adults with HIV/AIDS: An analysis of an HIV stigma scale and initial exploration of subscales. Res Soc Work Pract 15: 291-300.
- Sherbourne CD, Hays RD, Fleishman JA, Vitiello B, Magruder KM, et al. (2000) Impact of psychiatric conditions on health-related quality of life in persons with HIV infection. Am J Psychiatry 157: 248-254.
- Moore RC, Moore DJ, Thompson WK, Vahia Ipsit V, Grant I, et al. A case-controlled study of successful aging in older HIV-infected adults. J Clin Psychiatry 74: e417-e423.
- Leserman J (2003) HIV disease progression: Depression, stress, and possible mechanisms. Biol Psychiatry 54: 295-306.
- Lyketsos CG, Hoover DR, Guccione M, Senterfitt W, Dew MA, et al. (1993) Depressive symptoms as predictors of medical outcomes in HIV infection. Multicenter AIDS cohort study. JAMA270: 2563-2567.
- Evans DL, Ten Have TR, Douglas SD, Gettes DR, Morrison M, et al. (2002) Association of depression with viral load, CD8 T lymphocytes, and natural killer cells in women with HIV infection. Am J Psychiatry 159: 1752.
- Singh N, Squier C, Sivek C, Wagener M, Nguyen MH, et al. (1996) Determinants of compliance with antiretroviral therapy in patients with human immunodeficiency virus: Prospective assessment with implications for enhancing compliance. AIDS Care 8: 261-269.
- Farinpour R, Miller EN, Satz P, Selnes OA, Cohen BA, et al. (2003) Psychosocial risk factors of HIV morbidity and mortality: findings from the multicenter AIDS cohort study (MACS). J Clin Exp Neuropsychol 25: 654-670.
- Moskowitz JT (2003) Positive affect predicts lower risk of AIDS mortality. Psychosomatic Med 65: 620-626.
- Ciechanowski P, Wagner E, Schamling K, Schwartz S, Williams B, et al. (2004) Community-integrated home-based depression treatment in older adults. JAMA 291: 1569-1577.
- Lyketsos CG, Hutton H, Fishman M, Schwartz J, Treisman GJ (1996) Psychiatric morbidity on entry to an HIV primary care clinic. AIDS 10: 1033-1039.
- Applebaum A, Brennan M (2009) Mental health and depression. In: Brennan M, Karpiak SE, Shippy RA, Cantor MH, edn. Older Adults with HIV: An In-depth Examination of an Emerging Population. NY, USA: Nova Science Publishers pp: 27-34.
- Zanjani F, Saboe K, Oslin D (2007) Age difference in rates of mental health/substance abuse and behavioral care in HIV-positive adults. AIDS Patient Care STDS 21: 347-355.
- Deslich S, Stec B, Tomblin S, Coustasse A (2013) Telepsychiatry in the 21st century: Transforming healthcare with technology. Perspect Health Inf Manag.
- Ruskin PE, Silver-Aylaian M, Kling MA, Reed SA, Bradham DD, et al. (2004) Treatment outcomes in depression: Comparison of remote treatment through telepsychiatry to in-person treatment. Am J Psychiatry 161: 1471-1476.
- Mohr D, Vella L, Hart SL, Heckman T, Simon GE (2008) The effect of telephone-administered psychotherapy on symptoms of depression and attrition: a meta-analysis. Clin Psychol15: 243-253.
- Singh SP, Arya D, Peters T (2007) Accuracy of telepsychiatric assessment of new routine outpatient referrals. BMC Psychiatry 7: 1-13.
- Johnston D, Jones BN (2001) Telemedicine consultation to a rural nursing facility: A 2-year experience. J Geriatr Psychitary Neorol 14: 72-75.
- Khalifa N, Saleem Y, Stankard P (2008) The use of telepsychiatry within forensic practice: a literature review on the use of videolink. J Forens Psychiatry Psychol 19: 2-13.
- Saywell RM, Sevilla JF, Zollinger TW, Przybylski MJ, Zoppi K, et al. (2005) Barriers to health care access among urban Hispanics. Presented at the 133rd Annual Meeting & Exposition of the American Public Health Association. Philadelphia.
- Moon TD, Laurens MB, Weimer SM, Levy JA (2005) Nonemergent emergency room utilization for an inner-city pediatric population. Pediatr Emerg Care 21: 363-366.
- Spaulding R, Cain S, Sonnenschein K (2011) Urban telemedicine: uncommon service for a common need. Child Adolesc Psychiatric Clin N Am pp: 29-39.
- Kroenke K, Spitzer R, Williams W (2001) The PHQ-9: Validity of a brief depression severity measure. JGIM 16: 606-616.
- Endicott J, Nee J, Harrison W, Blumenthal R (1993) Quality of life enjoyment and satisfaction questionnaire: a new measure. Psychopharmacol Bull 29: 321-326.
- Fleury J (1994) The index of readiness: development and psychometric analysis. J Nurs Meas Winter 2: 143-154.
- Hamilton M (1960) A rating scale for depression. J Neurol Neurosurg Psychiatry 23: 56-62.
- Nasreddine Z (2004) Montreal Cognitive Assessment (MoCA).
- Folstein MF, Folstein SE, McHugh PR (1975) Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: 189-198.
- Smith P, Schmidt S, Allensworth-Davies D, Saitz R (2010) A single-question screening test for drug use in primary care. Arch Intern Med 170: 1155-1160.
- Young R, Willis E, Cameron G, Geana M (2014) “Willing but unwilling”: attitudinal barriers to adoption of home based health information technology among older adults. Health Informatics J 20: 127-135.

