Keywords
Disease Management; Fistula; Mirizzi Syndrome
INTRODUCTION
Laparoscopic cholecystectomy is the gold standard management for symptomatic gall stones. A gall stone that lies outside the gall bladder or fistulated into an adjacent organ needs further management can be is difficult to treat safely or effectively with the laparoscopic approach. Pablo Luis Mirizzi (1893 -1964) an Argentinean surgeon described Mirizzi’s Syndrome (MS) in 1948; a rare condition that occurs in approximately 1% of all cholecystectomies and affect around 0.1 % of all patients with gallstones [1]. Mirizzi’s Syndrome develops when a gallstone becomes impacted in the neck of the gallbladder or in the cystic duct causing compression of the common bile duct or common hepatic duct resulting in obstruction with or without jaundice and may progress into a cholecystocholedochal fistula. The obstructive biochemical picture can be caused by direct extrinsic compression from the impacted gall stone or from the fibrosis caused by advanced chronic cholecystitis [2]; It can also happen in post cholecystectomy patients with a long stone-containing cystic duct remnant. Identification of Mirizzi’s syndrome preoperatively will enable careful planning of the surgical procedure and reduces associated morbidity. Also, gall bladder cancer shares some of the clinical and radiological features and could co-exist [3] with Mirizzi’s syndrome adding an extra challenge and highlighting the importance of a detailed pre-operative evaluation whenever possible before embarking on surgery in such cases.
Classification of Mirizzi’s Syndrome
Various classifications were described in the literature with McSherry’s and Csendes’ being the most common; however Csendes is the only validated and most acceptable classification and hence its use for the purpose of this review [4].
Csendes classification of Mirizzi’s syndrome
Type I: Type I is divided into A and B; Type I A (Figure 1) when the extrinsic compression in the (common hepatic duct) CHD is caused by stones impacted in the cystic duct or in the infundibulum while Type IB denotes absence of cystic duct [5].
Figure 1. Type I Mirizzi’s syndrome (adopted from memoris.com).
Type II: Presence of cholecystocholedocal biliary fistula (CCBF) involving one third of the circumference of the CHD wall (Figure 2).
Figure 2. Type II Mirizzi’s syndrome (adopted from memoris.com).
Type III: Presence of cholecystocholedocal biliary fistula (CCBF) with a diameter over two thirds of the circumference of the CHD wall (Figure 3).
Figure 3. Type III Mirizzi’s syndrome (adopted from memoris.com).
Type IV: Presence of cholecystocholedocal biliary fistula (CCBF) which involves the entire circumference of the CHD wall (Figure 4).
Figure 4. Type IV Mirizzi’s Syndrome (adopted from memoris.com).
Type V: This is a new addition by the Csendes group includes any of the Mirizzi’s in the presence of a cystenteric fistula.
Csendes classification is useful in planning the management strategy; so, while simple cholecystectomy is suitable for type I patients; partial cholecystectomy adopting the fundus first dissection technique leaving a cuff of the infundibulum is needed for type II to avoid damage to the main bile ducts. Partial and subtotal cholecystectomy are terms that often used interchangeably in the literature which is inaccurate as subtotal cholecystectomy as originally described involves active dissection in Calot’s triangle to isolate the cystic duct and removal of the anterior wall of the gall bladder leaving the posterior wall behind [6] to avoid bleeding from the liver bed typically in cirrhotic livers; such technique is hazardous in Mirizzi’s syndrome where isolation of the cystic duct might not be possible and any attempt at it risks biliary ductal injury. Choledochoscoplasty (Figure 5) can be considered for type I B and is recommended for type II and early type III to restore adequate diameter of the hepatic duct; while the in the presence of bilio-enteric fistula in advanced i.e. types III and IV Mirizzi’s syndrome, Roux-en-Y hepaticojejunostomy (Figure 6) is considered the treatment of choice [7].
Figure 5. Cholecystotomy.
Figure 6. Stone extraction.
In choledochoplasty, we the utilize a pedicled graft of gall-bladder remnant in treatment of Mirizzi’s syndrome [8, 9]. In type IA, fundus-first cholecystectomy with simple closure of cystic duct while in type IB choledochoplasty using 5 mm cuff of the gall bladder is recommended. In type II lesions, the procedure depends on the size of the fistula; if it is less than one-third of the common duct diameter, choledochoplasty using 5 mm cuff of the gall bladder is recommended, and patients with fistula sizes between1/3 and 2/3 of the diameter of the common duct should undergo choledochoplasty with 10 mm cuff of the gall bladder [10] (Figures 6, 7, 8).
Figure 7. Choledochoplasty.
Figure 8. Roux-en-Y Hepaticojejunostomy.
Aim of the Study
We aimed to conduct a systematic review of Mirizzi syndrome’s management.
METHODS
Search Strategy
We carried out a literature search in Medline and Embase data bases using Ovid search engine using the following search terms: Mirizzi’s syndrome, Mirizzi*, Treatment, Laparoscop*, endoscop*, Laparoscopic treatment, endoscopic management and difficult common bile duct stones. We retrieved 24 documents from the databases from 1948 till November 2015 (As shown in PRISMA flow chart – Figure 9) illustrating the different strategies that has been employed worldwide. The number of published articles is limited and we could only include 14 articles addressing the adopted management approach (as shown in table 1) for both qualitative and quantitative synthesis. Ten (10) documents were excluded due to lack of patients’ data.
Figure 9. A PRISMA diagram outlining the search strategy.
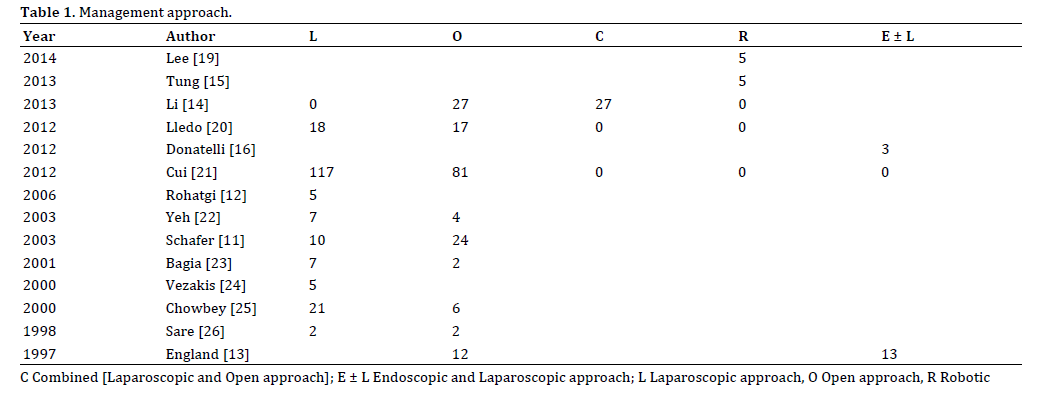
Pooling of Data: We further stratified the included articles based on the type of technique (Table 1) described in the adopted management approach of Mirizzi’s syndrome:
1) Conventional approach (laparotomy)
2) Laparoscopic approach
3) Laparoscopy, Endoscopy & Choledochoscopy
4) Robotic assisted minimal invasive approach.
5) Endoscopy ± Laparoscopic
We also assessed the outcome of the approach based on the complications and extent of morbidity reported in the literature.
RESULTS
A total of 425 patients’ data from 14 articles (Table 2) were included for qualitative synthesis; two hundred and twelve patients (212) were reported to have type I, eighty seven (87) were reported to have type II and forty six patients were reported to have type III. Eighty (80) patients’ did not have any record of Mirizzi’s type. One hundred and ninety-two (192) patients were managed with the laparoscopic approach while a hundred and seventy-five (175) patients were managed by open approach. Twentyseven (27) patients were managed by a combination of laparoscopic and open approach. Ten (10) patients were treated by laparoscopic robotic approach. A combination of endoscopic and laparoscopic approaches was employed in sixteen patients. Five (5) patients’ data were completely missing and [11] lacked the type of approach employed in the management of Mirizzi’s syndrome.
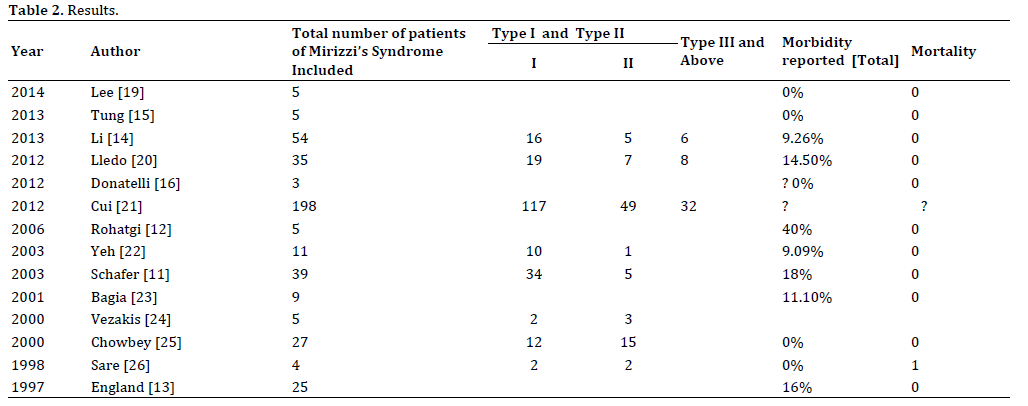
The reported morbidity for various approaches varied from 0% to 40%. The laparoscopic approach was reported to have highest morbidity (40%) [12] while the open approach had 16% morbidity [13]. The combined approach (laparoscopic converted to open) is reported to have morbidity of 9.26% [14]. The robotic approach is reported to have 0% morbidity [15] but the total number in this category was too small to enable any meaningful interpretation. And while the morbidity of the endoscopic and laparoscopic approach varied from 0% [16] to up to 16% [13], there were no deaths reported in the selected reviewed literature that are directly related to any type of management for Mirizzi’s syndrome; this may represent a limitation to data capture imposed by our protocol and our reading of the literature suggests that there is mortality of around 5% associated with surgical management of this disease.
DISCUSSION
The incidence of gall stone disease in UK as reported by NIHR (National institute for health research) is 10 to 15 % [17] with cholecystectomy being the gold standard therapy for symptomatic gall stones. One percent (1 %) of all patients undergoing cholecystectomy will present with manifestation of advanced gall stone disease i.e. Mirizzi’s syndrome which complicates the procedure and increases the risks of any intervention. Management of Mirizzi’s syndrome is technically challenging and is a common cause of postoperative bile leak. We revisited the literature to study the various described management strategies for Mirizzi’s syndrome.
Clinical features
Recurrent right upper quadrant pain, jaundice and fever associated with rigors is a typical presentation in up to 80% of the cases due to cholangitis caused by either mechanical obstruction secondary to the stones or inflammation around the common hepatic duct. Patient’s presenting with such symptoms should be further evaluated by MRCP (Magnetic resonance cholangiopancreaticography) and/or ERCP (endoscopic retrograde cholangiopancreatography) with endo-biliary stenting if required. In the remaining (20%) of patients with Mirizzi’s syndrome, they may present with biliary colic and altered liver function tests with or without concomitant evidence of luecocytosis; patients with such presentation may not be adequately assessed by transabdominal ultrasonography. These patients are at risk of complications following routine cholecystectomy including ductal injury and bile leaks if the disease is not appreciated pre- or intra-operatively. Once MS identified, a planned cholecystectomy by a specialist biliary surgeon following a thorough pre-operative evaluation by MRCP with or without pre-op ERCP offers the best chance of a favorable outcome in such difficult disease.
Diagnosis
Abdominal pain is the most common presenting symptom followed by jaundice and less commonly with the classical triad of cholangitis. And despite advances in imaging, the diagnosis of MS is still difficult and is often made intra-operatively. The diagnosis is usually suggested by biliary ultrasonography and then confirmed by MRCP or ERCP. Ultrasound diagnosis of Mirizzi’s syndrome demands presence of dilated intrahepatic ducts and common hepatic duct up to the point of external compression by the calculus where the bile duct can be seen to narrow [18]. In post cholecystectomy patients, MRCP or ERCP shows narrowing of the proximal CBD and non-filling of the cystic duct remnant. The criteria used to diagnose MS by other imaging modalities include evidence of compression of the bile duct with a stone impacted in the gallbladder neck or cystic duct with/without the presence of a cholecystocholedochal fistula.
Diagnostic Modalities
Ultrasonography or Computed Tomography (CT): May reveal stones at the junction of the cystic/common hepatic ducts associated with proximal dilation of the biliary tree. However, a dilated cystic duct can be confused with the common hepatic duct of normal diameter, thereby missing the diagnosis of this condition. Ultrasonography is poor at picking up MS and has a reported sensitivity of (<5%) [13]. The use of computed tomography (CT) for the diagnosis of MS is controversial; it may demonstrate the presence of cholecystocholedochal fistula and is of value in cases of suspected malignancy.
Magnetic Resonance Imaging: All patients with deranged LFTs should undergo magnetic resonance cholangiopancreaticography (MRCP) as this would confirm the diagnosis and guide therapy. Cholangioresonance is the best non-invasive imaging modality for diagnosis of Mirizzi’s syndrome. It can demonstrate with precision the presence of biliary dilation, degree of obstruction, intra luminal or external location of the biliary stones, and also identifies and evaluates the degree of inflammation around the gallbladder. It can also demonstrate any extrinsic narrowing of the common bile duct, reveal complications such as fistulae and helps to identify any anatomical variants.
Endoscopic Ultrasonography (EUS): Mirizzi’s syndrome is usually encountered intra-operatively in cases of long standing gall bladder diseases that would have been typically assessed by ultrasonography +/- MR cholangiography (cholangioresonance). And while EUS is an important diagnostic modality in ultrasound negative cases of suspected biliary pancreatitis i.e. for microlithiasis. And while endoscopic ultrasonography is used in some units for confirmation of choledocholithiasis prior to therapeutic ERCPs, it does not seem to play any major role in the diagnostic or management planning protocols of Mirizzi’s syndrome. On the other hand, intra-operative laparoscopic ultrasound if available could diagnose MS and aid management planning.
Endoscopic Retrograde Cholangiopancreatography (ERCP): may reveal narrowing or compression of the common hepatic duct. The diagnosis is traditionally made by endoscopic retrograde cholangiopancreatography (ERCP) during evaluation of the biliary tree in jaundiced patients. Lateral filling gap of the common hepatic duct and central dilation of the biliary tree on ERCP provide a strong suspicion of the syndrome. ERCP may also assist in differentiating benign from malignant strictures by smooth outline of the stricture and delineation of a cholecystocholedochal fistula; it can also play an important temporizing or a definitive therapeutic role in high risk surgical candidates through biliary drainage for cholangitis and jaundice.
Intraoperative Cholangiography or Ultrasonography: Intra-operatively, the presence of Mirizzi’s syndrome should be suspected upon finding of intense adhesion between the gallbladder and the common hepatic duct in the hepato-duodenal ligament or near Calot's triangle. The diagnosis could be confirmed by intra operative ultrasonography or cholangiography provided both the skills and equipment are available.
MANAGEMENT
The impacted cystic duct stones tend to be either inaccessible or irremovable endoscopically and although endoscopic lithotripsy (mechanical, electro-hydraulic and extra-corporeal shock wave) was attempted at our unit without success, other units reported variable level of success with such strategy. Endoscopic stenting is a valuable temporizing measure for surgically fit candidates and an appropriate definitive therapy for unfit ones, but surgery remains to be the treatment of choice for fit patients with Mirizzi’s syndrome. One must remember that operative management is a true surgical challenge for the most able especially in the presence of a fistula i.e. type II McSherry or Csendes type II-IV. Surgical treatment of Mirizzi’s syndrome includes careful dissection of biliary structures, complete removal of the stones from the biliary tract, and identification of the common hepatic duct. Surgical approach often demands an incision in the gallbladder fundus and removal of the impacted stone, a gush of bile indicates the presence of a fistula. The gall bladder is often very fibrosed and contracted so that fundic traction provides relatively poor exposure of the hepatobiliary triangle posing a critical limitation for the laparoscopic approach and could lead to damage of hepatic duct when a normal caliber hepatic duct may be mistaken for a dilated cystic duct that runs parallel to it and hence the laparoscopic approach should be used exclusively for Csendes type I with minimal inflammation. Intra-operative ultrasonography or cholangiography should be utilized whenever possible to reduce the risk of misidentification biliary ductal injury. Complete removal of the gallbladder in patients with Mirizzi syndrome can be difficult due to intense inflammation around Calot's triangle and other management options should be explored depending on the severity of the on the Mirizzi’s syndrome.
Csendes type I
Cholecystectomy, as an isolated surgical procedure is performed in patients with Mirizzi syndrome Csendes type I where recurrent inflammation of the distended gallbladder results in compression of common hepatic duct by the tense Hartmann’s pouch. In the absence of cholecystobiliary fistula (Csendes type I), cholecystectomy and removal of the biliary stones is the standard treatment. In the presence of choledocholithiasis and when choledochotomy presents technical difficulties, postoperative endoscopic extraction of ductal calculi is a safer alternative. Several methods for handling the residual choledochal defects are employed ranging from direct suturing to flap choledochoplasty or hepaticojejunostomy.
Csendes type II
In patients with Csendes type II and III, where erosion of the gallbladder and common hepatic duct wall by the impacted stone resulted in a small cholecysto-choledochal fistula, partial cholecystectomy with choledochoplasty using a cuff of the gallbladder remnant may be more appropriate. The technique is described by Sandblom [9], in which an initial partial cholecystectomy is performed anterogradely, with preservation of the infundibulum, followed by opening of the bottom of the gallbladder and removal of the stones from its interior.
Choledochoplasty (Figure 7) is completed by suturing the fistulous orifice in the wall of the duct to the remaining gallbladder using absorbable sutures. A T-tube is introduced into the common hepatic duct with the top end extending above the repair site. Closure of the defect in the common hepatic duct should be completed without tension and with the mucous membrane of the gallbladder stump juxtaposed to the mucous membrane of the duct.
Using the infundibulum of the gallbladder to close to the orifice in the common hepatic duct has the advantage of being vascularized and of similar mucous membrane to that of the biliary duct. This is a specialist skill and even when performed well this technique has inherent tendencies towards fibrosis and stenosis (stricture formation) at the suture lines.
In advanced disease, the inflamed tissues do not allow healing following primary closure of the fistula due to the tissue’s poor ability of holding sutures leading to post-operative biliary leak and late bile duct strictures. An anastomosis between healthy bile duct tissue and Roux-Y jejunal loop is the the safest alternative in such circumstances (Figure 8).
Csendes type III / IV
Biliary –enteric Anastomosis: In Csendes type IV, the gallbladder is removed or left in situ due to absence of dissection planes between the gallbladder and the common hepatic duct and biliary reconstruction is then accomplished by side-to-side (or end to side if cholecystectomy is achieved) choledochoduodenostomy, Roux-en-Y choledochojejunostomy or hepaticojejunostomy (Figure 8) but the latter (hepaticojejunostomy) is the preferred option if possible.
Minimal Access Surgery in Mirizzi’s Syndrome
The role of minimally access surgery in treatment of Mirizzi syndrome remains controversial. Some authors consider such a condition to be inappropriate or even a contraindicatio for laparoscopic surgery as the scarring and inflammatory tissue near Calot's triangle cause difficulty in dissection. Others have reported that a laparoscopic approach, especially for Csendes type I lesions, is feasible but technically demanding, however, conventional laparotomy seems to be necessary in the vast majority of cases requiring the correction of cholecystocholedochal fistula.
Endoscopic Therapy in Mirizzi’s Syndrome
In patients with Mirizzi syndrome, satisfactory results can be obtained through biliary drainage by endoscopic papillotomy and placement of biliary endoscopic stents. These procedures confirm the diagnosis, alleviate jaundice, relieve cholangitis and allow resolution of the local inflammatory process in preparation for a subsequent definitive elective surgical intervention if appropriate. If ERCP is to be used as a definitive therapy, other procedures may be needed including use of “a mother and baby scope” and electrohydraulic or laser lithotripsy.
Prognosis
Chronic obstruction of the biliary tract may cause permanent hepatic damage, especially when there is some degree of chronic infection. Such situations lead to epithelial biliary ductal proliferation which could be followed by portal fibrosis [19]. Prolonged cholestasis may eventually cause secondary biliary cirrhosis; however timely relief of cholestasis by a successful intervention may lead to regression of the hepatic damage with disappearance of the infiltration of biliary pigments.
CONCLUSION
Mirizzi syndrome continues to be a diagnostic and a management challenge and the condition may not be recognized by routine preoperative imaging and becomes evident at the time of surgery suggested by the dense adhesions around Calot's triangle.
The reported post-operative surgical mortality rates of 8% reflect the complexity of managing such patients with this serious biliary tract disorder. The postoperative morbidity includes mainly the development of external biliary fistula, bile peritonitis and sub phrenic abscess.
Maintaining a high index of suspicion as a differential to all patients with obstructive biochemical or clinical picture ensures accurate preoperative diagnosis combined; the aforementioned combined with intra-operative recognition of the condition and individualized therapeutic strategy based on a detailed work up by USS, MRCP +/- ERCP, and/or intra-operative imaging remain key for a successful outcome. Failure of recognition increases the risk of biliary ductal injury. An attempt at definitive surgical therapy in advanced cases by non-specialists particularly when hepatico-jejunostomy is required may lead to sub-optimal results.
Conflict of Interest
The authors declare that there is no conflict of interests regarding the publication of this paper.
References
- Hazzan D, Golijanin D, Reissman P, Adler SN, Shiloni E. Combined endoscopic and surgical management of Mirizzi syndrome. Surg Endosc 1999; 13:618–20. [PMID: 10347304]
- Leopardi LN, Maddern GJ. Pablo Luis Mirizzi: The man behind the syndrome. ANZ Journal of Surgery 2007; 77:1062–4. [PMID: 17973667]
- Redaelli CA, Büchler MW, Schilling MK, Krähenbühl L, Ruchti C, Blumgart LH, et al. High coincidence of Mirizzi syndrome and gallbladder carcinoma. Surgery 1997; 121:58–63. [PMID: 9001552]
- Beltrán MA. Mirizzi syndrome: History, current knowledge and proposal of a simplified classification. World J Gastroenterol 2012; 18:4639. [PMID: 23002333]
- Csendes a, Díaz JC, Burdiles P, Maluenda F, Nava O. Mirizzi syndrome and cholecystobiliary fistula: a unifying classification. Br J Surg 1989; 76:1139–43. [PMID: 2597969]
- Katsohis C, Prousalidis J, Tzardinoglou E, Michalopoulos A, Fahandidis E, Apostolidis S, et al. Subtotal Cholecystectomy. HPB Surg 1996; 9:133–6. [PMID: 8725451]
- Aydin Ü, Yazici P, Özsan I, Ersöz G, Özütemiz Ö, Zeytunlu M, Coker A. Surgical management of Mirizzi syndrome. Turk J Gastroenterol 2008; 19:258–63. [PMID: 19119478]
- Strugnell NA, Sali A. Choledochoplasty for cholecystocholedochal fistula (Mirizzi syndrome type II): a case report and literature review. Aust N Z J Surg 1995; 65:285–8. [PMID: 7717951]
- Sandblom P, Tabrizian M. [Plastic repair of choledochus using a biliary vesicle pedicle flap]. Helv Chir Acta 1974; 41:789–92. [PMID: 4448673]
- Shah OJ, Dar MA, Wani MA, Wani NA. Management of Mirizzi syndrome: A new surgical approach. ANZ J Surg 2001; 71:423–7. [PMID: 11450919]
- Schäfer M, Schneiter R, Krähenbühl L. Incidence and management of Mirizzi syndrome during laparoscopic cholecystectomy. Surg Endosc 2003; 17:1186–90; discussion 1191–2. [PMID: 12739118]
- Rohatgi A, Singh KK. Mirizzi syndrome: laparoscopic management by subtotal cholecystectomy. Surg Endosc 2006; 20:1477–81. [PMID: 16865619]
- England RE, Martin DF. Endoscopic management of Mirizzi’s syndrome. Gut 1997; 40:272–6. [PMID: 9071944]
- Li B, Li X, Zhou W-C, He M-Y, Meng W-B, Zhang L, et al. Effect of endoscopic retrograde cholangiopancreatography combined with laparoscopy and choledochoscopy on the treatment of Mirizzi syndrome. Chin Med J (Engl) 2013; 126:3515–8. [PMID: 24034100]
- Tung KLM, Tang CN, Lai ECH, Yang GPC, Chan OCY, Li MKW. Robotassisted laparoscopic approach of management for Mirizzi syndrome. Surg Laparosc Endosc Percutan Tech 2013; 23:e17–21. [PMID: 23386165]
- Donatelli G, Dhumane P, Dallemagne B, Ludovic M, Delvaux M, Gay G, et al. Double-cannulation and large papillary balloon dilation: Key to successful endoscopic treatment of mirizzi syndrome in low insertion of cystic duct. Dig Endosc 2012; 24:466–9. [PMID: 23078442]
- Brazzelli M, Cruickshank M, Kilonzo M, Ahmed I, Stewart F, McNamee P, Elders A, et al. Clinical effectiveness and cost-effectiveness of cholecystectomy compared with observation/conservative management for preventing recurrent symptoms and complications in adults presenting with uncomplicated symptomatic gallstones or cholecystitis: a syste. Health Technol Assess 2014; 18:1–102. [PMID: 25164349]
- Dewbury KC. The features of the Mirizzi syndrome on ultrasound examination. Br J Radiol [Internet]. 1979; 52:990–2. [PMID: 526803]
- Schweizer W, Schott G, Zimmermann A, Triller J, Blumgart LH. [Clinical significance and histological classification of atrophy/hypertrophy complexes of the liver]. Schweiz Med Wochenschr 1993; 123:1598–603. [PMID: 8378760]










