Keywords
Pancreatic Neoplasms; Sarcoidosis; Steroids
INTRODUCTION
Sarcoidosis is a chronic multiorgan granulomatous disease of unknown etiology. Sarcoid granulomas are formed by infectious and non-infectious exogenous agents that stimulate auto-antigens to HLA Class II surface molecules on mononuclear cells stimulating T-helper inducer lymphocyte resulting in an exaggerated cellular immune response. Sarcoid lesions are noncaseating epithelioid cell granulomas with asteroid bodies [1, 2]. Sarcoidosis is a multiorgan disease that has a high predilection for the lymph nodes (99%), lungs (90%), myocardium (74%), liver (60%), and to a lesser extent the skin (25%) and eyes (25%) [1, 3, 4, 5]. With the exception of the liver, gastrointestinal tract involvement is uncommon. Pancreatic sarcoidosis is rare and often asymptomatic, it is often discovered on autopsy and occurs in 1-3% of cases of systemic sarcoidosis [5, 6, 7, 8]. Symptomatic pancreatic sarcoidosis has only occasionally been reported. A MEDLINE search from 1966 to 2007, using the key words pancreatic sarcoidosis revealed only 26 cases of symptomatic pancreatic sarcoidosis. We report a case of symptomatic pancreatic sarcoidosis.
CASE REPORT
A 54-year-old African American male was referred to gastroenterology clinic for the evaluation of severe fatigability, poor appetite and 3.5 kg weight loss over the past two months, and elevated alkaline phosphates and hepatic transaminases. He had no abdominal pain, nausea, vomiting, pruritus, diarrhea, yellow discoloration of skin and sclera, acholic stool or dark urine. He drank 1 to 2 cans of beer a month for 15 years, and denied smoking cigarettes. He had no history of blood transfusions, intravenous drug use or multiple sexual partners. He had not traveled outside of the United States in the past 10 years. His family history was noncontributory. His past medical history included pulmonary sarcoidosis, diabetes, hypertension, benign prostrate hypertrophy, seizure disorder, and hypercholesterolemia. His medications included levetiracetam, metformin, tolterodine, tamsulosin, glipizide, enalapril and aspirin. No allergies were reported.
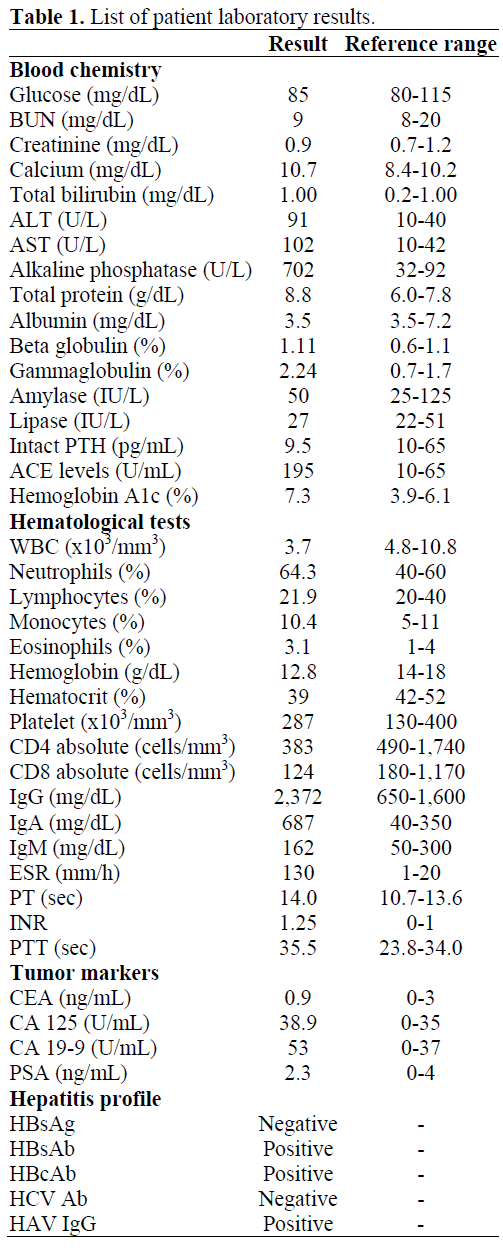
A review of systems was remarkable for a nonproductive cough and shortness of breath on exertion that waxes and wanes for the past few years. His physical exam revealed an alert and oriented male (height, 168 cm; weight 64 kg). His vitals were the following: pulse, 76/minute and regular; blood pressure, 138/76 mmHg; respiratory rate 12 breaths/minute; temperature, 36.7°C (98°F). A funduscopic examination was normal. The head and neck exam was pertinent for discrete cervical lymphadenopathy. The abdomen was soft, non-distended and non-tender with normal liver and spleen span. The neurological, cardiovascular, and chest examinations were unremarkable. He presented with leukopenia (3,700 cells/mm3; reference range: 4,800-10,800 cells/mm3), hypercalcemia (11.4 mg/dL; reference range: 8.4-10.2 U/L), elevated liver enzyme tests (AST 102 U/L and ALT 91 U/L; reference ranges: 10-42 U/L and 10-40 U/L, respectively), an elevated alkaline phosphatase (702 U/L; reference range: 32-92 U/L), and an elevated erythrocyte sedimentation rate 130 mm/h (reference range: 1-20 mm/h). His coagulation profile was slightly elevated. His renal function tests, serum glucose, and pancreatic enzymes were normal (Table 1).
Tests for pancreatic exocrine insufficiency were not performed since the patient did not exhibit signs and symptoms of malabsorption. A chest roentgenograph was normal. However, a computed tomography (CT) scan of the chest demonstrated predominant peribronchial and perivascular markings involving the upper and middle lobe of the right lung with calcified subcarinal and hilar lymph nodes suggestive of sarcoidosis. A CT scan guided biopsy of enlarged cervical lymph node was consistent with a sarcoid lesion. An abdominal CT scan demonstrated a pancreatic head mass with retroperitoneal lymph node enlargement (Figure 1). Magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangio- pancreatography (ERCP) were not performed since the biliary and pancreatic ducts were not dilated and the serum bilirubin level was normal. A CT scan guided pancreatic mass biopsy demonstrated noncaseating granulomas with Langerhan giant cells and fibrosis (Figure 2). Both an acid fast bacilli stain and gram stain for a fungal infection were negative.
Figure 1. Computed tomography scan of abdomen
with pancreatic head mass.
Figure 2. Sarcoid lesion in pancreatic mass biopsy.
Oral prednisone 40 mg daily for 7 days followed by a 7 week tapering schedule was initiated. The patient’s signs and symptoms improved: his fatigability resolved and appetite improved; liver enzyme tests and serum calcium levels normalized. The patient did develop prednisone-induced hyperglycemia that was managed by titrating upwards his glipizide regimen. A repeat abdominal CT scan 4 weeks after initiation of prednisone treatment revealed no change in the size of the head of the pancreas and peripancreatic lymph nodes. After completing his 8 week course of prednisone treatment, clinically he remains stable without any abnormal laboratory parameters.
DISCUSSION
Asymptomatic Pancreatic Sarcoidosis Prevalence
In 1937, Nickerson published the first autopsy case of pancreatic involvement with noncaseating granulomas in a patient with systemic sarcoidosis [9]. Mayock et al., reported three cases of pancreatic involvement (3%) from 287 autopsies of patients known to have sarcoidosis [7]. A large autopsy series in Japan accumulated over 28 years of patients who died from sarcoidosis reported a higher incidence of pancreatic involvement at 2.1% [10]. In this Japanese autopsy series of case reports, half of those found to have pancreatic sarcoidosis were asymptomatic and died of other causes. In 2006, Caceres et al. reported 25 patients with surgically proven pancreatic sarcoidosis of which 12 cases presented with a pancreatic mass localized to the head of pancreas, and 13 cases presented with a diffusely firm nodular pancreas [4].
Symptomatic Pancreatic Sarcoidosis Prevalence
In 1950, Curran and Curran published the first surgically diagnosed case of pancreatic sarcoidosis via an exploratory laparotomy of a patient with persistent diffuse abdominal pain [11]. Noguchi et al. in 1993 reported 14 patients with pancreatic sarcoidosis [12]. Biopsy of the pancreas established the diagnosis in 7 cases; 4 were diagnosed by biopsy of the peripancreatic lymph nodes and 3 by clinical findings only. At laparotomy 6 patients showed swollen pancreas with diffuse nodular changes, 4 had enlargement of the head and only one patient had a combination of pancreatic head mass and diffuse enlargement. Peripancreatic lymphadenopathy was observed in majority of these patients. In 2006, Cacreas et al. reported 4 cases of symptomatic pancreatic sarcoidosis out of 25 patients with surgically proven pancreatic sarcoidosis [4].
Symptomatic pancreatic sarcoidosis most commonly presents with abdominal pain, weight loss, obstructive jaundice and emesis [4, 13]. Three cases of pancreatic sarcoidosis presented as acute pancreatitis [14, 15]. Pancreatic symptoms are due to organ infiltration and compression by enlarged lymph nodes [2]. Sarcoidosis presenting as a mass in the pancreas is less in common but does occur [13, 16, 17, 18, 19].
Our patient with a known history of pulmonary sarcoidosis presented with constitutional symptoms and a pancreatic mass on CT scan of abdomen. Our patient’s clinical condition and liver enzyme tests improved with corticosteroid treatment (prednisone). A follow up CT scan of the abdomen 8 weeks after presentation and during prednisone treatment showed no change in the size of pancreatic head. In this setting, pancreatic sarcoidosis is likely and a laparotomy with standard pancreaticoduodenectomy may not be necessary. However, since our patient only had pancreatic head involvement, a biopsy of the pancreatic head is necessary to rule out a malignancy and to establish the diagnosis of pancreatic sarcoidosis. If the pancreatic head mass caused significant obstruction of the common bile duct, ERCP with brushing of the pancreatic and biliary duct with possible pancreatic and biliary stent placement could be considered in addition to medical treatment. Our patient is being followed clinically with monitoring of liver enzyme tests every 6 months; cancer antigen 19-9 (CA 19-9), serum angiotensin converting enzyme (ACE) levels, and CT scan of abdomen to detect any change in size of pancreatic head, involvement of body and tail of pancreas and other abdominal visceras by sarcoidosis or malignancies are being evaluated annually.
Pharmacotherapy
There are no standard guidelines for treating pancreatic sarcoidosis and the prognosis of the disease is variable. Corticosteroids is the pharmacotherapy of choice for the management of sarcoidosis [3, 20, 21, 22]. Corticosteroids are indicated for ocular, cardiac and central nervous system involvement, stage 2 pulmonary disease, and patients presenting with malignant hypercalcemia or constitutional symptoms. Corticosteroids therapy has been effective in many cases, however, occasionally achieving only spontaneous remission [15, 16]. Chronic corticosteroid use can be associated with hypertension, cushingoid effects, psychosis, osteoporosis, glaucoma, cataracts, hypokalemia, glucose intolerance, telangiectasis, acne, and gastropathy. Due to the deleterious effects of chronic corticosteroid pharmacotherapy, its use should be employed only after careful considering its risks and benefits. After discontinuing corticosteroids, the recurrence rate of pancreatic sarcoidosis in severe symptomatic cases is 100% [22].
CONCLUSION
Sarcoidosis is a chronic multiorgan disease that uncommonly involves the pancreas. Pancreatic involvement is usually asymptomatic and discovered on autopsy. However, clinicians should be cognizant that sarcoidosis can present with symptomatic pancreatic mass, albeit rarely.
References
- Crystal RG. Sarcoidosis. In: Fauci AS, Braunwald E, Isselbacher KJ, et al. eds. Harrison's Principles of Internal Medicine. 15th Ed. New York, NY, USA: McGraw-Hill Inc, 2001:1969-1974.
- Bacal D, Hoshal VL Jr, Schaldenbrand JD, Lampman RM. Sarcoidosis of pancreas: case report and review of literature. Am Surg 2000; 66:675-6. [PMID 10917480]
- Mikami R, Hosoda H, Odaka M. Sarcoidosis. Jpn J Clin Med 1983; 41:1443.
- Caceres M, Sabbaghian MS, Braud R, Wilks S, Boyle M. Pancreatic sarcoidosis: unusual presentation resembling a periampullary malignancy. Curr Surg 2006; 63:179-85. [PMID 16757369]
- Siavelis HA, Herrmann ME, Aranha GV, Garcia G, Eubanks T, Reyes CV. Sarcoidosis and the pancreas. Surgery 1999; 125:456-61. [PMID 10216537]
- Ricker W, Clark M. Sarcoidosis. A clinicopathological review of three hundred cases, including twenty two autopsies. Am J Clin Pathol 1949; 19:725.
- Mayock RL, Bertrand P, Morrison CE, Scott JH. Manifestations of sarcoidosis. Analysis of 145 patients with a review of nine series selected from the literature. Am J Med 1963; 35:67-89. [PMID 14046006]
- Longcope WT, Freiman DG. A study of sarcoidosis. Medicine (Baltimore) 1952; 31:1-132. [PMID 14899212]
- Nickerson DA. Boeck's sarcoid. Arch Pathol Lab Med 1937; 24:19-29.
- Iwai K, Tachibana T, Hosoda Y, Matsui Y. Sarcoidosis autopsies in Japan. Frequency and trend in the last 28 years. Sarcoidosis 1988; 5:60-5. [PMID 3881021]
- Curran JF Jr, Curran JF Sr. Boeck's sarcoid of the pancreas. Surgery 1950; 28:574-8. [PMID 14776666]
- Noguchi H, Hirai K, Seo A, Yoshitake M, Sakai T, Abe H, et al. Sarcoidosis accompanied by pancreatic impairment. Intern Med 1993; 32:15-20. [PMID 8495038]
- Ryrie DR. Sarcoidosis with obstructive jaundice. Proc R Soc Med 1954; 47:879. [PMID 13215528]
- McCormick PA, Malone D, Fitzgerald MX, Fitzgerald O. Pancreatitis in sarcoidosis. Br Med J (Clin Res Ed) 1985, 290:1472-3. [PMID 3922537]
- McCormick PA, O'Donnell M, McGeeney K, Fitzgerald O, McCormick DA, Fitzgerald MX. Sarcoidosis and the pancreas. Ir J Med Sci 1988; 157:181. [PMID 2460419]
- Sagalow BR, Miller CL, Wechsler RJ. Pancreatic sarcoidosis mimicking pancreatic cancer. J Clin Ultrasound 1988; 16:13-134. [PMID 3130406]
- Stampfl DA, Grimm IS, Barbot DJ, Rosato FE, Gordon SJ. Sarcoidosis causing duodenal obstruction: case report and review of gastrointestinal manifestations. Dig Dis Sci 1990: 35:526-32. [PMID 2180656]
- Brady MS, Garfein CF, Klimstra D, Brenann MF. Sarcoidosis of the pancreas. J Surg Oncol 1993; 54:132-7. [PMID 8412160]
- Rodriguez J, Dyck WP. An unusual case of pancreatic sarcoidosis presenting as a pancreatic mass. Am J Gastroenterol 1996; 91:2253-4. [PMID 8855773]
- Yamamoto M. Clinical studies on sarcoidosis. J Jpn Soc Intern Med 1987; 76:1497. [PMID 3325587]
- Izumi T. Sarcoidosis in Kyoto (1963-1986). Jpn J Thorac Dis 1987; 5:142-6. [PMID 3227188]
- Takada K, Ina Y, Noda M, Morishta M. The treatment, course and prognosis of sarcoidosis cases. Jpn J Thorac Dis 1990; 28:92.



